ISSN Online: 2177-1235 | ISSN Print: 1983-5175
Giant lipoma of the lower limb and its impact on the vascular system
Lipoma gigante de membro inferior com repercussão no sistema vascular
Case Report -
Year2013 -
Volume28 -
Issue
3
José Carlos Daher1; Jefferson Di Lamartine Galdino Amaral2 Marcela Caetano Cammarota2; Alberto Benedik Neto3; Cesar Augusto Daher Ceva de Faria3
ABSTRACT
Lipomas are the most common mesenchymal tumors, which may develop in different parts of the body. However, giant lipomas are rare and sometimes difficult to diagnose owing to their location and the presenting clinical consequences. In this report, we present the case of a patient with a giant lipoma in the left popliteal region that was surgically treated after a detailed radiological assessment. Further, we discuss the preoperative diagnosis and its difficulties, often caused by the deep localization of the tumor and the impossibility of obtaining a conclusive radiological diagnosis. Moreover, we describe the successful treatment, along with the step-by-step surgical approach and the final outcome achieved.
Keywords:
Lipoma. Neoplasms, adipose tissue. Soft tissue neoplasms.
RESUMO
Os lipomas são os tumores mesenquimais mais frequentes e podem ocorrer em diversas partes do corpo. Entretanto, lipomas gigantes são raros, por vezes de difícil diagnóstico, em decorrência de sua localização, e com consequências clínicas. Neste artigo é apresentado um caso de lipoma gigante em região poplítea esquerda, tratado cirurgicamente após detalhado estudo radiológico. São discutidos o diagnóstico pré-operatório e suas dificuldades, muitas vezes causadas pela localização profunda e pela impossibilidade de diagnóstico conclusivo pela imagem. O tratamento foi concluído com sucesso, sendo descritos a abordagem cirúrgica passo a passo e o resultado final.
Palavras-chave:
Lipoma. Neoplasias lipomatosas. Neoplasias de tecidos moles.
INTRODUCTION
Lipomas are tumors of mesenchymal origin that are the most commonly observed neoplasms, accounting for 10% of cases1. Lipomas may develop in any organ of the human body that contains adipose tissue, from the viscera to the brain. They are histologically composed of mature adipocytes, although their etiology remains unknown. No recurrence is observed after complete surgical removal. The most common clinical manifestation of lipomas is the appearance of tumors in the subcutaneous tissue; in most cases, lipomas are painless and cause discomfort only when they become large enough to cause aesthetic or functional disorders.
The present study focused on giant lipomas, which are traditionally defined as tumors larger than 10 cm and/or weighing more than 1000 g2. The diagnosis usually relies on clinical examination results, which are based on easily visible and palpable tumors in the subcutaneous tissue. However, when tumors are located deep into the muscular fasciae, they may remain unnoticed for a long period owing to the tensile strength of the fasciae and aponeurosis. Giant lipomas may develop because of functional alterations of the affected organ, mass effect production, and compression of noble structures such as vessels and nerves3. In such cases, the diagnosis is performed by radiological examinations, and confirmation is obtained by histopathological assessment4,5. The natural history of appearance, evolution, and incidence of recurrences are still unknown.
In this report, we present the case of a patient with a giant lipoma of the lower limb that was surgically treated after a meticulous radiological investigation, and we discuss the functional implications of the disease.
CASE REPORT
A 70-year-old retired man from Brasília presented the following complaints at the time of surgery: feelings of heaviness and pain, discomfort and swelling of the left lower limb, difficulty in flexing the left leg and walking, and the presence of varicose veins in the leg and left popliteal region (Figure 1).

Figure 1 - Preoperative aspect of the lipoma located in the posterior muscles of the left thigh.
Two years prior, the patient underwent surgery for the treatment of the varicose veins in both his lower limbs. However, because of recurrence in the left leg, the patient had to undergo another surgical procedure.
When referred to our service center, the patient underwent computed tomography (CT) and bilateral phlebography of the lower limbs.
The CT scan revealed a mass with septations and well-defined contours, which was located between the posterior muscles of the thigh, compressing the popliteal vessels (Figure 2). The presence of a giant lipoma was suspected. Venography (Figure 3) and magnetic resonance imaging (MRI) revealed interrupted the flow to the popliteal veins on the left side and the development of a collateral network, which confirmed compression of the popliteal vessels by the tumor.
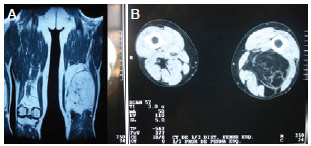
Figure 2 - A, Magnetic resonance image revealing the lipomatous lesion in the posterior muscles of the left thigh. B, Computed tomographic scan revealing the lipomatous lesion.

Figure 3 - Venographic image showing the disruption of the flow of the popliteal veins to the left and the development of a collateral network that confirmed compression of the popliteal vessels.
Although the final diagnosis of the lesion was not obtained, based on the combination of the radiological aspects of the mass, such as the well-defined contours and absence of invasive characteristics, and the long evolution period, also suggestive of the benign nature of the tumor, we decided to perform complete or partial resection of the tumor. The tumor was then evaluated through a histopathological analysis.
An incision of approximately 9 cm was planned, with the consideration of the possibility of a longer incision, if necessary. After performing the incision of the skin and subcutaneous tissue, another incision was made in the aponeurotic plane to reveal the distal end of the posterior muscles of the thigh, which were subsequently separated. Ectoscopy of the exposed surface of the tumor and its palpation suggested a lipoma. The cleavage plane was well defined and better released after saline injection under pressure, an approach used for blunt dissection in areas outside the visual field.
Expansion of the incision was not necessary for the removal of the tumor, which measured 20 x 10 x 8 cm3 (weight, 2400 g) and presented lipomatous characteristics (Figure 4). A plane closure was performed to prevent postoperative formation of hematomas and seroma. Vacuum drainage was applied for 24 hours, and postural measures were adopted to prevent deep venous thromboembolism and pulmonary embolism. Low-weight heparin was administered during the 2 days of hospitalization.
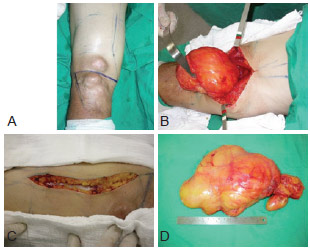
Figure 4 - Intraoperative aspect. A, Preoperative delimitation. B, Exposure of the tumor. C, Approximation of the margins of the incision after the removal of the tumor. D, The removed tumor.
The postoperative evolution was favorable, with complete functional recovery and remission of all signs and symptoms (Figure 5). The histopathological report confirmed the diagnosis of lipoma.
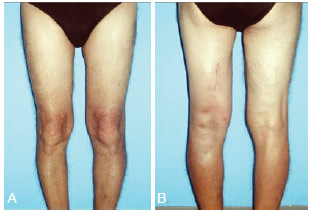
Figure 5 - Postoperative appearance. A, Anterior view. B, Posterior view.
DISCUSSION
The term lipoma is used to designate a tumor that develops from the adipose tissue and may affect any organ. Given that the adipose tissue is ubiquitous in the human body, as it is present from the bone marrow to the brain, lipomas may be observed in the most varied locations4,6. The most common characteristics of these tumors are that they are soft, small, solitary, and easily resectable, as they present a well-defined capsule. When small and located in the subcutaneous tissue, they are removed mainly under local anesthesia and without any complications. Lipomas are more frequently observed in women and young individuals. They develop from mesenchymal cells, and as such, may differentiate into fibrolipomas, lipoxanthomas, and so on. Lipomas are commonly asymptomatic and usually removed for aesthetic reasons.
Though rarer than giant lipomas, several lipomatous syndromes may cause severe, sometimes disabling, deformities. The best known example is Madelung's disease, which was first described in 1888 by Otto Madelung as a clinical condition of unknown etiology, in which a symmetric deposition of adipose tissue on the neck, retroauricular, supraclavicular, and posterior regions of the neck was observed. Another clinical disorder also triggered by lipomas is the painful adipose tissue or Dercum's disease, characterized by multiple subcutaneous lipomas, which cause articular pain, especially in obese postmenopausal women.
Giant lipomas are deeply localized and may be found in intramuscular (infiltrating lipomas) and intermuscular tissues7. They are not common, accounting only for fewer than 5% of all lipoma cases8,9. Giant lipomas commonly develop in the cervical region, chest, and lower limbs (inguinal region and thigh). Malignant transformation is rare; however, these tumors should always be histopathologically assessed and differentiated from liposarcomas, fibrous histiocytoma, or other soft tissue tumors that are also clinically represented as large masses. In case of rapid growth, early recurrence or skin ulceration should increase the suspicion of malignancy5,7. Giant lipomas mostly develop between the sixth and seventh decades of life and unlike the common lipomas, predominantly affect men10. Besides aiding with diagnosis, radiological examinations clarify the involvement of adjacent structures, facilitating the definition of the operative plan and the choice of the best access route. Dynamic tests such as the echo Doppler cardiogram and other imaging modalities such as MRI may aid in the assessment of the extent of impairment of the vascular system. However, only histopathological examinations are able to provide a definitive diagnosis2,5,8,9.
Soft tissue sarcomas (liposarcomas, rhabdomyosarcomas, and leiomyosarcomas) are generally insidious and asymptomatic in their initial phase. They develop early metastases and present an irregular contour on radiological examination. The neoplastic transformation of giant lipomas is rare; however, its occurrence is associated with early recurrences, skin ulcerations, and poor cleavage plane during surgery.
The case described in this report is that of a giant intermuscular lipoma, the location of which (i.e., posteriorly and anteriorly between the strong fascia of the flexor muscles of the thigh and the femur, respectively) compressed the popliteal vessels resulting in venous stasis upstream from the tumor. This caused the patient to undergo two inappropriate surgical procedures because of the misdiagnosis.
Giant lipomas, though rare, are clinical conditions of great importance, as they can affect any organ. In addition, they may not be perceived in the early stages, only revealed at the onset of impairment in organ function or shape, when they are already deeply localized, that is, in the advanced stages. We should consider the importance of including giant lipomas in the differential diagnosis to avoid misdiagnosis and inappropriate treatments.
REFERENCES
1. Terzioglu A, Tuncali D, Yuksel A, Bingul F, Aslan G. Giant lipomas: a series of 12 consecutive cases and a giant liposarcoma of the thigh. Dermatol Surg. 2004;30(3):463-7.
2. Sanchez MR, Golomb FM, Moy JA, Potozkin JR. Giant lipoma: case report and review of the literature. J Am Acad Dermatol. 1993;28(2 Pt 1):266-8.
3. Botwin KP, Shah CP, Zak PJ. Sciatic neuropathy secondary to infiltrating intermuscular lipoma of the thigh. Am J Phys Med Rehabil. 2001;80(10):754-8.
4. Davis C Jr, Gruhn JG. Giant lipoma of the thigh. Arch Surg. 1967;95(1):151-6.
5. Hakim E, Kolander Y, Meller Y, Moses M, Sagi A. Gigantic lipomas. Plast Reconstr Surg. 1994;94(2):369-71.
6. Bloom RA, Gomori JM, Fields SI, Katz E. Abdominal wall lipoma: CT and MRl appearance. Comput Med Imaging Graph. 1991;15(1):37-9.
7. Kindblom LG, Angervall L, Stener B, Wickbom I. Intermuscular and intramuscular lipomas and hibernomas. A clinical, roentgenologic, histologic, and prognostic study of 46 cases. Cancer. 1974;33(3):754-62.
8. Fletcher CD, Martin-Bates E. Intramuscular and intermuscular lipoma: neglected diagnoses. Histopathology. 1988;12(3):275-87.
9. Behrend EM. Intermuscular lipomas. Am J Surg. 1929;7:857-60.
10. Nishida J, Morita T, Ogose A, Okada K, Kakizaki H, Tajino T, et al. Imaging characteristics of deep-seated lipomatous tumors: intramuscular lipoma, intermuscular lipoma, and lipoma-like liposarcoma. J Orthop Sci. 2007;12(6):533-41.
1. Plastic surgeon, member of the Brazilian Society of Plastic Surgery (BSPS), regent of the Plastic Surgery Service of Hospital Daher, Brasília, DF, Brazil
2. Plastic surgeon, member of the BSPS, member of the Plastic Surgery Service of Hospital Daher, Brasília, DF, Brazil
3. Medical resident at the Plastic Surgery Service of Hospital Daher, aspirant member of the BSPS, Brasília, DF, Brazil
Correspondence to:
José Carlos Daher
Department of Plastic Surgery - Hospital Daher Lago Sul
SHIS QI 7 - conj. F - Lago Sul
Brasília, DF, Brazil - CEP 71615-205
E-mail: daher@hospitaldaher.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: 8/19/2010
Article accepted: 12/31/2010
This study was performed at the Investigations Center of Hospital Daher, Brasília, DF, Brazil.
 All scientific articles published at www.rbcp.org.br are licensed under a Creative Commons license
All scientific articles published at www.rbcp.org.br are licensed under a Creative Commons license


