ABSTRACT
INTRODUCTION The treatment of acquired immunodeficiency syndrome has undergone important advances since the introduction of highly active antiretroviral therapy (HAART). This treatment led to the elimination of the virus in the bloodstream and increased survival; however, metabolic and structural changes became evident. One of these changes is lipodystrophy, the redistribution of body fat. With one of the largest samples worldwide, the aim of this work was to present some of the various surgical alternatives as well as the results obtained for minimizing the impact of lipodystrophy.
METHOD: From July 2005 to July 2013, 510 patients with HAART-associated lipodystrophy underwent surgery in the Clinic of Plastic Surgery, Heliópolis Hospital. All patients submitted to prior clinical and immunological assessments made with the aid of the infectious diseases team. The present study was approved by the Research Ethics Committee of the ABC Foundation.
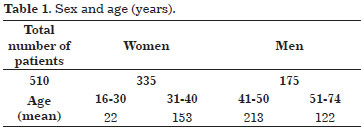
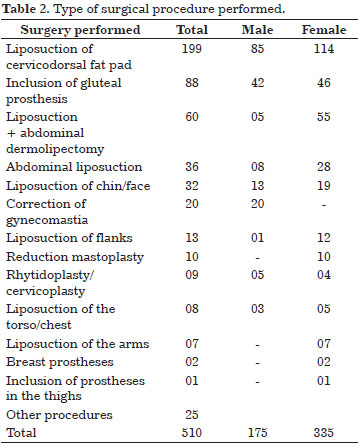
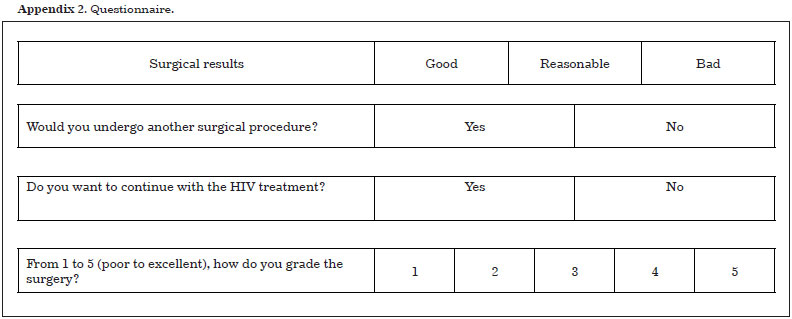
RESULTS: The 510 patients included 335 women and 175 men with an age range of 16-74 years. Liposuction of the cervicodorsal fat pad (buffalo hump) was predominant (199 cases). With regard to the response stimulated through a subjective questionnaire, a high degree of satisfaction was observed with a significant increase in self-esteem and greater adherence to antiretroviral treatment.
CONCLUSION: The surgical correction of body lipodystrophy demonstrably improves the aesthetics of patients using HAART; however, its psychological and social effects are even more important since self-esteem increases and stigma decreases, which leads to better adherence to antiretroviral treatment.
Keywords:
Lipodystrophy; HIV infections; Serodiagnosis of AIDS; Lipectomy; Body composition.
RESUMO
INTRODUÇÃO O tratamento da Síndrome da Imunodeficiência Adquirida vem sofrendo importantes avanços desde a introdução da terapia antirretroviral altamente ativa, conhecida como HAART (high active antirretroviral therapy). Este tratamento levou à eliminação do vírus na corrente sanguínea e ao aumento na sobrevida, entretanto alterações metabólicas e estruturais tornaram-se evidentes. Uma dessas alterações é a redistribuição de gordura corpórea, também denominada lipodistrofia. Com uma das maiores casuísticas mundiais, o objetivo deste trabalho é demonstrar algumas das alternativas cirúrgicas, bem como os resultados obtidos na tentativa de minimizar o impacto da lipodistrofia.
MÉTODO: No período de julho de 2005 a julho de 2013, 510 pacientes portadores de lipodistrofia secundária ao uso de HAART foram operados pela Clínica de Cirurgia Plástica do Hospital Heliópolis. Todos esses pacientes foram submetidos à prévia avaliação clínica e imunológica, sob auxílio da equipe de Infectologia. O presente trabalho foi aprovado pelo Comitê de Ética em Pesquisa da Fundação do ABC.
RESULTADO: Dentre os 510 pacientes, 335 eram do sexo feminino e 175 do sexo masculino, com idades variando entre 16 e 74 anos. Quanto aos procedimentos, destacou-se lipoaspiração da giba e dorso, com 199 casos. Quanto à resposta estimulada através de questionário subjetivo, observou-se elevado grau de satisfação, aumento significativo da autoestima e maior adesão ao tratamento antirretroviral.
CONCLUSÃO: A correção cirúrgica da lipodistrofia corporal comprovadamente melhora o aspecto estético do paciente que faz uso da HAART; porém, o efeito psicológico e social é ainda mais importante, elevando a autoestima, com diminuição dos estigmas, e proporcionando uma maior adesão ao tratamento antirretroviral.
Palavras-chave:
Lipodistrofia; Infecções por HIV; Sorodiagnóstico da AIDS; Lipectomia; Composição corporal.