



Case Report - Year 2026 - Volume 41Issue 1
Microsurgical Cathedral-Shaped Free Flap Reconstruction Following Resection of Tongue Carcinoma: Case Report
Reconstrução microcirúrgica com retalho livre em forma de catedral após ressecção de carcinoma da língua: Relato de caso
Mario Augusto Ferrari de Castro1 ; Kauê de Carvalho Moura2; Bruno Pelinson Fogaça Duarte1,; Rogério Aparecido Dedivitis3
; Kauê de Carvalho Moura2; Bruno Pelinson Fogaça Duarte1,; Rogério Aparecido Dedivitis3
ABSTRACT
Large lesions to the tongue pose a significant challenge, requiring meticulous threedimensional reconstruction to achieve oncological resection and optimal speech and swallowing function for the patient. In the current case report, we present a reconstruction using a microsurgical, anterolateral, thigh free flap shaped like a cathedral to restore the anterior two-thirds of the tongue and the floor of the oral cavity following advanced tongue cancer resection. The patient experienced rapid recovery and restoration of physiological function.
Keywords: tongue neoplasms; head and neck neoplasms; free tissue flaps; mouth neoplasms; microsurgery
RESUMO
As grandes lesões da língua representam um desafio significativo, que exige uma reconstrução tridimensional minuciosa para alcançar a ressecção oncológica e as funções ideais de fala e deglutição para o paciente. Neste relato de caso, apresentamos uma reconstrução por meio de um retalhomicrocirúrgico livre anterolateral da coxa em forma de catedral para restaurar os dois terços anteriores da língua e o assoalho da cavidade oral após a ressecção de câncer de língua avançado. O paciente teve uma rápida recuperação e restauração da função fisiológica.
Palavras-chave: neoplasias da língua; neoplasias de cabeça e pescoço; retalhos de tecido livre; neoplasias da boca; microcirurgia
Introduction
Oral cavity cancer, predominantly squamous-cell carcinoma, carries significant morbidity and mortality, with the tongue being a common site of occurrence.1,2 Surgery remains the primary treatment method, often complemented by radiotherapy and chemotherapy in cases with a high risk of recurrence. Consequently, there is considerable emphasis on the surgical technique to ensure oncological clearance while optimizing postoperative quality of life and functional rehabilitation.3,4
In cases requiring extensive tongue resection, the free flap reconstruction described by Leymarie et al.5 emerges as a highly-effective option. Common donor sites include the radial forearm (RF) and anterolateral thigh (ALT), with careful consideration to factors such as defect size, donorsite morbidity, adjacent-structure reconstruction, flap-reinnervation potential, and simultaneous oncological resection.2 The outcome of the flap reconstruction may vary, for it is generally influenced by its shape. Numerous designs for flaps and techniques for their placement have been developed to replicate the intricate three-dimensional structure of the tongue.6 We herein present a case of an advanced malignant tongue neoplasm that was successfully reconstructed with an ALT free flap shaped like a cathedral.
Case Report
A 65-year-old male patient, with a long history of smoking, presented with an ulcerated, painful lesion on the lingual surface associated with dysphagia and weight loss that had begun 3 months before. Biopsy confirmed squamous-cell carcinoma. A physical examination revealed an ulcerated, infiltrative lesion extending beyond the midline on the right border and ventral surface of the tongue (►Fig. 1). There were no lumps on the neck.


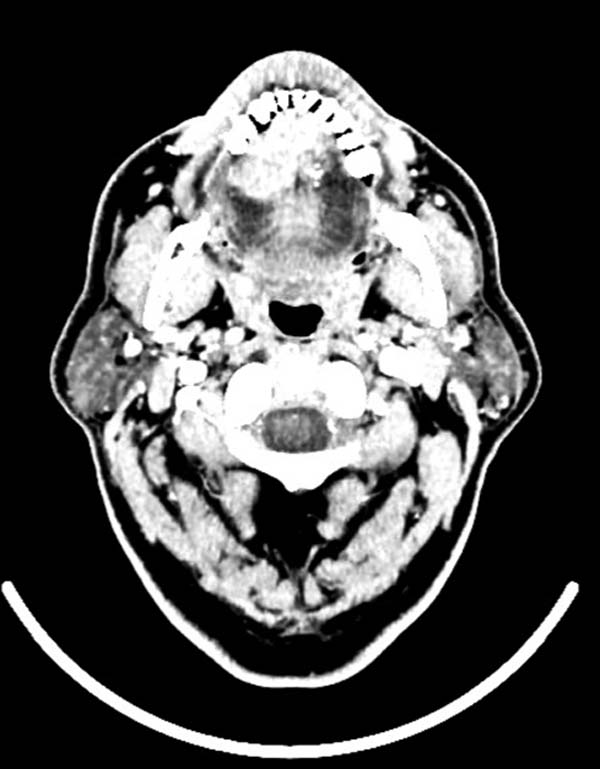
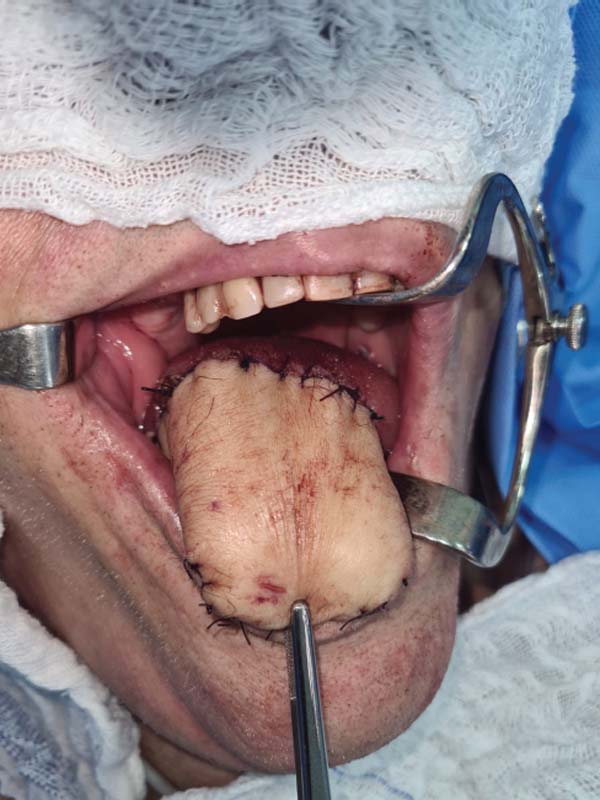
A neck computed tomography scan revealed a lesion measuring 2.1 × 3.1 × 1.7 cm at the center of the right anterior tongue (►Fig. 2). Nasofibrolaryngoscopy revealed no lesion at the base of the tongue. The patient underwent type-IVa subtotal glossectomy with bilateral supraomohyoid neck dissection. Reconstruction employed a microsurgical ALT flap shaped like a cathedral (►Figs. 3–7). The patient was discharged on the seventh postoperative day (see ►Fig. 8).












On the fifteenth day, the nasoenteral tube was removed, and the patient transitioned from a nasoenteral to an oral diet within 30 days. On the thirtieth postoperative day (►Fig. 9), the patient presented with good swallowing and no changes, with a very intelligible voice, presenting only a possible hematoma in the posterior region. After this evaluation, the patient was lost to follow-up. A histopathological analysis revealed invasive, well-differentiated keratinizing squamous cell carcinoma measuring 2.5 cm with a 10-mm depth of invasion. The margins were clear, and there was no lymph node involvement (tumor [T], node [N], and metastasis [M] classification: T3N0MX).7 Adjuvant radiotherapy was administered.


Discussion
Tongue defects are primarily associated with oncological resections.2 These lesions often occur on the lateral border in the first two-thirds of the tongue, and in about 75% of the cases, there is no contralateral invasion of the organ.7 Even in cases of small oncological resections, reconstruction using local, pedicle, or free flaps may be necessary to maintain a safety margin of 1.5 to 2 cm.2 Although glossectomy refers only to the resection of the tongue, the surgical procedure may involve adjacent structures as well, potentially extending beyond the oral portion to include the tongue base. Therefore, more elaborate flap techniques are often required to restore the ability to swallow and phonate as closely as possible to the physiological form.2,4
For smaller lesions, healing through second intention, simple sutures, skin grafts, or local flaps may be considered.2,8 Nevertheless, in cases in which a hemiglossectomy is indicated, a more complex flap is typically required. The selection of the appropriate flap depends on various factors, such as the size of the lesion, evaluation of donor vessels in the neck, invasion of the floor of the mouth, invasion of the pharynx, and involvement of the mandible.
Microsurgical reconstruction for oral cavity defects was introduced in 1983 using an RF free flap. Since then, the technique has become increasingly widespread and has evolved over time. Nowadays, microsurgical reconstruction is the preferred method for larger tongue defects, with the RF and ALT being the most commonly selected donor sites for the free flaps.2,7
Immediate reconstruction should be considered because it leads to superior functional outcomes, and also because oncology patients may require postoperative radiotherapy. The benefits of the ALT flap include minimal morbidity at the donor site and the availability of a substantial volume of tissue for flap creation. This makes it an excellent choice to address extensive tongue defects, even those affecting more than half of the tongue.2,6
Some authors7,8 argue that the size of the ALT flap may lead to a new tongue with reduced mobility. Several studies have indicated that, when compared to the RF flap, the ALT flap demonstrates comparable outcomes in postoperative factors such as speech intelligibility, mobility, and swallowing. Consequently, given its lower morbidity at the donor site, the ALT flap may be considered a preferable option over the RF flap.7,8 The design of the flap should be customized to meet the specific needs of each patient. Several shapes described in the literature6 have shown similar functional outcomes and mobility. Therefore, the context of the resection stands as one of the most crucial factors to consider when determining the shape of the flap.
In the case herein reported, we chose the cathedral shape because of its ability to fulfill the large volume of tissue that was resected and the possibility of restoring mobility to an almost-physiological level. The presence of good swallowing and fairly-intelligible speech in the late postoperative period were probably due to the preservation of the base of the tongue, with reconstruction performed only on the oral tongue, which provided adequate movement for phonation and swallowing. In addition to the surgical aspect, successful outcomes are associated with patients who have strong motivation, family support, access to speech therapy during rehabilitation, and consistent oncological follow-up with the surgical team.8
Final Considerations
The ALT flap, shaped like a cathedral, can be considered a favorable option for larger tongue defects. It provides ample tissue volume and can be customized to match the patient’s resection requirements, resulting in favorable physiological outcomes and a speedy recovery.
REFERENCES
1. Zanoni DK, Montero PH, Migliacci JC, et al. Survival outcomes after treatment of cancer of the oral cavity (1985-2015). Oral Oncol 2019;90:115–121. Doi: 10.1016/j.oraloncology.2019.02.001
2. Vincent A, Kohlert S, Lee TS, Inman J, Ducic Y. Free-Flap Reconstruction of the Tongue. Semin Plast Surg 2019;33(01):38–45. Doi: 10.1055/s-0039-1677789
3. Cervenka B, Pipkorn P, Fagan J, et al. Oral cavity cancer management guidelines for low-resource regions. Head Neck 2019;41 (03):799–812. Doi: 10.1002/hed.25423
4. Ansarin M, Bruschini R, Navach V, et al. Classification of GLOSSECTOMIES: Proposal for tongue cancer resections. Head Neck 2019; 41(03):821–827. Doi: 10.1002/hed.25466
5. Leymarie N, Karsenti G, Sarfati B, Rimareix F, Kolb F. Modification of flap design for total mobile tongue reconstruction using a sensitive antero-lateral thigh flap. J Plast Reconstr Aesthet Surg 2012;65(07):e169–e174. Doi: 10.1016/j.bjps.2011.11.012
6. Choi JW, Alshomer F, Kim YC. Evolution and current status of microsurgical tongue reconstruction, part II. Arch Craniofac Surg 2022;23(05):193–204. Doi: 10.7181/acfs.2022.00857
7. Baas M, Duraku LS, Corten EML, Mureau MAM. A systematic review on the sensory reinnervation of free flaps for tongue reconstruction: Does improved sensibility imply functional benefits? J Plast Reconstr Aesthet Surg 2015;68(08):1025–1035. Doi: 10.1016/j.bjps.2015.04.020
8. Amer IA. New modification of flap design for total and near-total mobile tongue reconstruction using anterolateral thigh flap. Egypt J Surg 2021;40(01):330–341. Doi: 10.4103/ejs.ejs_350_20
1. Universidade Metropolitana de Santos, Santos, SP, Brazil
2. Department of Head and Neck Surgery, Hospital Ana Costa, Santos, SP, Brazil
3. Department of Head and Neck Surgery, Hospital das Clínicas, Faculdade de Medicina,
Universidade de São Paulo (HCFMUSP), São Paulo, SP, Brazil
Address for correspondence Bruno Pelinson Fogaça Duarte, Undergraduate Medicine Student, Rua Eduardo Risk 86, Enseada, Guarujá, SP, CEP: 11441–140, Brazil (e-mail: bruno_duarte72@yahoo.com.br).
Article received: June 05, 2025.
Article accepted: January 13, 2026.
Conflict of Interests
The authors have no conflict of interests to declare..
Editor-in-Chief: Dov Charles Goldenberg.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket