



Original Article - Year 2026 - Volume 41Issue 1
Impact of Vacuum Therapy on Traumatic Wound Reconstruction - A Single-Center Experience
Impacto da terapia de pressão negativa na reconstrução de feridas traumáticas - Experiência unicêntrica
André Luiz Bilieri Pazio1 ; Pietro Maran Novais2,; Leticia Fernandes de Souza Porto3; Gabriel Victor Werner3; Isabella Correa de Oliveira4; Maitê Mateus4; Kevin Gollo4; Daniela Thais Lorenzi Pereira4; Renato da Silva Freitas1
; Pietro Maran Novais2,; Leticia Fernandes de Souza Porto3; Gabriel Victor Werner3; Isabella Correa de Oliveira4; Maitê Mateus4; Kevin Gollo4; Daniela Thais Lorenzi Pereira4; Renato da Silva Freitas1
ABSTRACT
Introduction Negative Pressure Wound Therapy (NPWT) stimulates the wound healing process, being an ally to plastic surgeons in the reconstruction of traumatic injuries. However, its impact on the time and complexity of reconstruction has only been vaguely investigated.
Objectives To evaluate the success and associated factors in short-termreconstruction of traumatic wounds using NPWT, when compared with traditional gauze dressing.
Materials and Methods Prospective cohort of adult patients with traumatic wounds in the upper and lower extremities, treated by plastic surgery, from December 2022 to February 2024. Patients were followed-up in the traditional and NPWT groups, from the first assessment until 15 days after reconstructive surgery. The variables were evaluated through statistical tests, and logistic regression was performed.
Results There were 18 patients and 32 wounds included in the traditional group, while 15 patients and 18 wounds were included in the NPWT group. There was a higher wound resolution in the NPWT group (83.3 vs. 50%, p=0.02). This treatment also reduced complexity of reconstruction in 61.1% of the cases (p=0.005) and increased the chance of successful healing by six times (OR=5.993). Delayed time to first reconstructive surgery reduced short-term healing success by 6.5% per day (OR =0.935). No differences were observed in the number of debridement performed, type of reconstruction, and complications/infections.
Conclusion Delaying surgery negatively influences the success of traumatic wound reconstruction. The use of NPWT increases the short-term success in closing these injuries and reduces the complexity of reconstruction.
Keywords: wounds and injuries; lower extremity; reconstructive surgery; negative pressure wound therapy; limbs
RESUMO
Introdução A terapia de pressão negativa (TPN) em feridas estimula o processo de cicatrização, sendo uma aliada de cirurgiões plásticos na reconstrução de lesões traumáticas. Ainda assim, seu impacto no tempo e na complexidade da reconstrução tem sido pouco investigado.
Objetivos Este estudo avaliou o sucesso e os fatores associados na reconstrução em curto prazo de feridas traumáticas utilizando TPN em comparação aos curativos tradicionais com gaze.
Materiais e Métodos Este é um estudo de coorte prospectiva de pacientes adultos com feridas traumáticas nos membros superiores e inferiores tratados pela cirurgia plástica de dezembro de 2022 a fevereiro de 2024. Os pacientes submetidos ao tratamento tradicional ou à TPN foram acompanhados desde a primeira avaliação até 15 dias após a cirurgia reconstrutiva. As variáveis foram avaliadas por meio de testes estatísticos, incluindo regressão logística.
Resultados O grupo tradicional incluiu 18 pacientes e 32 feridas, enquanto o grupo TPN incluiu 15 pacientes e 18 feridas. A resolução da ferida foimaior no grupoTPN (83,3 vs. 50%, p=0,02). Esse tratamento também reduziu a complexidade da reconstrução em 61,1% dos casos (p=0,005) e aumentou a probabilidade de cicatrização bemsucedida em seis vezes (razão de chance [OR]=5,993). O atraso no primeiro procedimento reconstrutivo reduziu o sucesso da cicatrização em curto prazo em 6,5% por dia (OR=0,935). Não foram observadas diferenças no número de desbridamentos realizados, tipo de reconstrução e complicações/infecções.
Conclusão A realização tardia da cirurgia influencia negativamente o sucesso da reconstrução de feridas traumáticas. O uso de TPN aumenta o sucesso do fechamento dessas lesões em curto prazo e reduz a complexidade da reconstrução.
Palavras-chave: ferimentos e lesões; extremidade inferior; cirurgia reconstrutiva; tratamento de feridas por pressão negativa; membros
Introduction
Trauma is the leading cause of death in people under 45-years-old worldwide. In Brazil, the most common affected area for traumatic injuries is the lower limb, leading to surgical intervention in up to 89.5% of the cases. This epidemiology is a reason for concern, since the morbidity generated by these events has a direct impact on the economically active population.1–4
In cases of severe trauma, 85% of patients develop combined limb fractures, most of which are associated with extensive soft tissue injuries. Along with the systemic inflammatory response generated by the trauma, this increases the risk of complications, thus requiring a multi-disciplinary approach.1–4
Plastic surgery plays a fundamental role in the reconstructive process of traumatic limb wounds, from initial care with serial debridement and dressing guidance to the final stage of reconstruction, with the use of grafts and/or flaps. This action aims to treat wounds to rehabilitate the patient, allowing them to return to their activities, and often avoiding drastic measures, such as amputation.1,3,5,6
Negative pressure wound therapy (NPWT), or vacuum therapy, popularly known as vacuum dressing, is a type of “bridge” treatment, that is, a temporary measure used to optimize the wound bed, preparing it for the final reconstructive stage. Although it has been known and used for almost 30 years,7 there are not many conclusive studies that evaluate the outcome of its use in traumatic limb injuries, when compared with traditional dressings, mainly in terms of wound closure and stepping down in the reconstructive ladder.8–10
Therefore, the objective of this study was to compare the use of NPWT and common dressings in traumatic limb wounds, regarding the impact on the planning and choice of definitive reconstructive treatment, and on the success of reconstruction, thus determining the applicability of this therapy.
Materials and Methods
This study is a prospective cohort study that uses convenience sampling, conducted at the Plastic Surgery Department of the Hospital do Trabalhador in Curitiba, PR, Brazil. It was approved by the hospital’s ethics committee (CAAE: 64896022.3.0000.5225), following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.11
The Hospital do Trabalhador is a level 1 trauma center. The hospital keeps a Plastic Surgery team specialized in complex wounds, with 60% of the physicians qualified in microsurgery.
The inclusion criteria were patients aged 18 years or older; male and female genders; who agreed to participation and signed the Informed Consent Form (authorization to collect data and photographs); with presence of traumatic injuries in the lower and upper limbs, with loss of soft tissue or exposure of noble tissues, whose primary closure would not be possible or was contraindicated, and with the first evaluation by Plastic Surgery performed between December, 2022 and February, 2024. The exclusion criteria were injuries whose etiology was burns (thermal, electrical, or chemical) or the action of venomous animals; those with vasculitis; and those lost to follow-up.
The patients accepted and in agreement with the study were followed up in two groups, with one using traditional dressing and the other vacuum dressing. The choice of dressing type was made by plastic surgeons from the service, not involved in the study. At the time of the first evaluation, images of the wounds and patients’ clinical records were independently evaluated by two of our plastic surgeons. Each one established the reconstructive technique that they would use (initial plan), with complete agreement between them, before the decision to traditional dressing or NPWT.
The date of traditional dressing use (dry gauze, cotton wool, and bandages) and the time of use until the first reconstructive surgery were assessed for patients in the traditional group. In the NPWT group, information was collected regarding the time from trauma to placement of vacuum dressings in a sterile environment, number of changes, and time of use until the first reconstructive surgery. According to the service protocol, vacuum dressings are kept in continuous mode, 24 hours a day, at a pressure of 125 mmHg, with a polyurethane sponge (►Fig. 1). Reconstructive surgery was defined as those that were not purely debridement or placement of a vacuum dressing and which involved the use of a reconstructive ladder technique.12


In both groups, the following data were collected from medical records: sex; age; comorbidities; etiology of the injury; region of the injury; initial size of the wound, with the width measured from medial to lateral and length from cranial to caudal; depth of the maximum layer of the lesion; other associated lesions; date of first hospital admission in the emergency room; date of plastic surgery consultation request; date of first plastic surgery evaluation; date of first reconstructive surgery; number of debridement; time between admission and plastic surgery consultation request; time between first admission and first reconstructive surgery; reconstructive option performed; whether full wound closure was achieved within 15 days of the first reconstructive surgery (short-term success); total number of reconstructive surgical procedures, including the first, within 15 days; and local wound complications (infection, hematoma, partial flap dehiscence, total flap loss, total graft loss, and thromboembolic events).
For this research, data were collected up to 15 days after the first reconstructive surgery, or 30 days after consultation, whichever was greater. After this period, patients continued to receive care from plastic surgery and other specialties, if necessary, but without new data collection by the researchers.
Data were collected and stored in a Microsoft Excel (Microsoft Corp.) spreadsheet. Inferential analysis for quantitative variables was tested for normality using the Kolmogorov-Smirnov test, followed by Student’s t or Mann-Whitney’s U tests, depending on normality, expressed as mean ± standard deviation (SD) or median and interquartile range (IQR). The qualitative variables were assessed using the Chi-Squared or Fisher exact tests, as indicated, expressed as absolute numbers and percentages.
To assess the difference between the reconstructive type performed, independently decided by plastic surgery physicians, and the initial technique evaluated, the techniques were ordinally organized in whole numbers (1 = closure by 2nd intention; 2 = primary closure; 3 = closure by 3rd intention; 4 = skin graft; 5 = local flap; 6 = regional flap; 7 = tissue expander; 8 = microsurgical flap)12 and compared in pairs (technique performed and initial plan, respectively) within groups by the Wilcoxon signed rank test.13
A stepwise backward binary logistic regression model was created by likelihood ratio, and odds ratio (OR) values with 95% confidence intervals (95% CI) were estimated to evaluate factors associated with short-term closure, being significant if X2(5) = 42.539, p < 0.001, R2 Nagelkerke = 0.516. All tests were two-tailed and p-values < 0.05 were considered significant. Data analysis was performed with the IBM SPSS Statistics (IBM Corp.) software, version 29.0.
Results
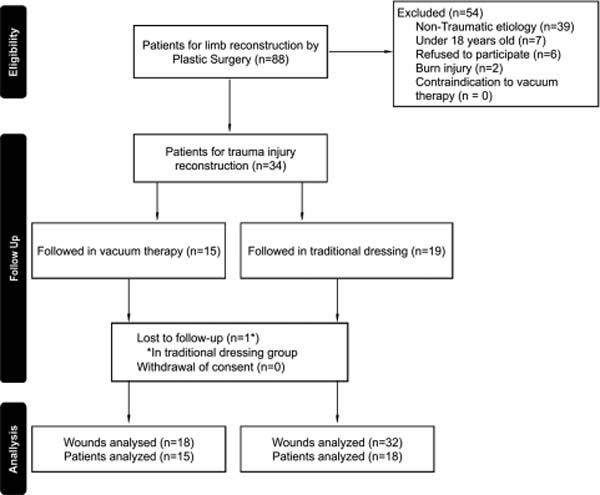
Of the 88 patients who underwent upper and lower limb reconstruction for complex wounds by the plastic surgery team during the period described above, 34 patients were included in the study. As one patient was lost to follow-up, the final sample consisted of 33 patients and 50 wounds analyzed (►Fig. 2).

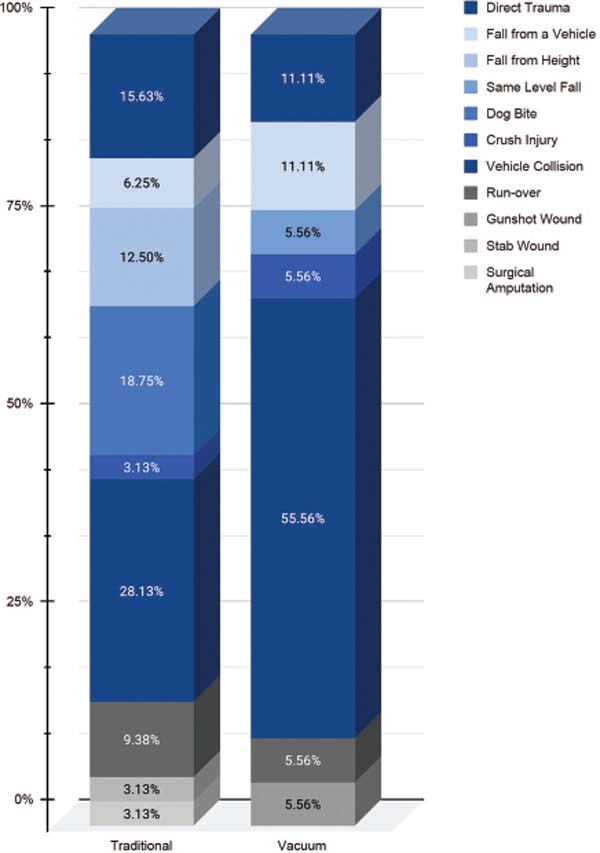
The groups were similar in terms of the number of men and women, age, presence of comorbidities, number of wounds, and size of wounds (►Table 1). In contrast, the NPWT group had a higher proportion of wounds reaching the bone layer, while the traditional group had a higher rate reaching the subcutaneous layer. The time intervals were all similar, showing that the use of NPWT did not delay reconstruction (►Table 1). Orthopedic injuries were present in 58% of the wounds. The etiologies of the injuries were not different between the groups (p = 0.127; ►Fig. 3).
| Patients’ characteristics | Group n (%) | p-value | |
|---|---|---|---|
| Traditional | Vacuum | ||
| Sex | 1.000a | ||
| Masculine | 13 (72.3) | 10 (66.7) | |
| Feminine | 5 (27.7) | 5 (33.3) | |
| Comorbidity | 11 (61.2) | 6 (40) | 0.227b |
| Smoking | 7 (38.8) | 2 (13.3) | 0.134a |
| Diabetes mellitus | 2 (11.1) | 2 (13.3) | 1.000a |
| Corticoid use | 1 (5.6) | 1 (6.7) | 1.000a |
| Age, years (mean SD) | 45.33 4.53 | 43.73 5.45 | 0.823c |
| Number of wounds (mean SD) | 1.72 0.27 | 1.27 0.11 | 0.421d |
| Width, cm median (IQR) | 6.62 (5–11.5) | 8.81 (4.27–12.86) | 0.739d |
| Length, cm median (IQR) | 7.15 (4.0316.07) | 9.6 (5.5–13.44) | 0.467d |
| Pre-operative infection‡ | 21 (65.6) | 14 (77.8) | 0.368a |
| Injury depth | 0.033a* | ||
| Dermis | 1 (3.1) | 0 | |
| Subcutaneous | 7 (21.9) | 0 | |
| Muscular | 16 (50) | 8 (44.4) | |
| Bone | 8 (25) | 10 (55.6) | |
| Interval, daysd Median (IQR) | |||
| Admission—Consultation request | 4 (0–7.25) | 9.5 (0–17.5) | 0.303 |
| Consultation request—PS evaluation | 1.5 (0.75–2) | 1 (0–2.75) | 0.487 |
| PS evaluation—1st reconstructive surgery | 10 (7–20.5) | 17 (14–21) | 0.153 |
| Dressing—1st reconstructive surgery | 13 (6.75–22) | 9 (7–14) | 0.305 |
| Admission—1st reconstructive surgery | 22 (13.75–33.75) | 27.5 (18.25–37.25) | 0.210 |


Regarding outcome, the wounds in the NPWT group achieved short-term full wound closure (after 15 days of the first reconstructive surgery) in a greater proportion than the wounds in the traditional dressing group (83.3 vs. 50%, p = 0.02). There was no difference in the proportions between complications, number of debridement, or number of surgical procedures required to complete the reconstruction (►Table 2).
| Outcomes and complications | Group | p-value | |
|---|---|---|---|
| Traditional | Vacuum | ||
| Dressing changes | 11 (6–22.8) | 0 (0–1) | < 0.001a* |
| Debridements | 2 (1–2.75) | 2.5 (2–3) | 0.084a |
| Reconstructive surgeries | 2 (1–2) | 1 (1–2) | 0.219a |
| Complications | 10 (31.2) | 3 (16.7) | 0.328b |
| Postoperative infection‡ | 6 (18.8) | 1 (5.6) | 0.398b |
| Full wound closure at 15 days | 16 (50) | 15 (83.3) | 0.020c* |

From the surgical procedures performed, in the traditional group the split thickness skin graft (STSG) was chosen in 62.5% of the wounds, followed by the regional flap in 28.1% of the cases. In the NPWT group, STSG was chosen in 61.1% of the wounds, followed by 33.3% with a regional flap (►Table 3). However, there was a greater reduction in complexity in the reconstructive ladder in the NPWT group (p = 0.005), and greater maintenance in the traditional group, but without significant difference (p = 0.107), as shown in ►Table 4.
| Reconstructive procedure | Initial plan n (%) | Performed n (%) | ||
|---|---|---|---|---|
| Traditional | Vacuum | Traditional | Vacuum | |
| Closing by 2nd intention | 2 (6.3) | 0 | 1 (3.1) | 1 (5.6) |
| Closing by 3rd intention | 0 | 0 | 1 (3.1) | 0 |
| Skin graftb | 16 (50) | 5 (27.8) | 20 (62.5) | 11 (61.1) |
| Local flap | 2 (6.3) | 1 (5.6) | 1 (3.1) | 0 |
| Regional flap | 8 (25) | 3 (16.7) | 9 (28.1) | 6 (33.3) |
| Microsurgical flap | 4 (12.5) | 9 (50) | 0 | 0 |
| p-valuea | 0.055 | 1.000 | ||


A binary logistic regression model was performed to assess factors associated with successful reconstruction, including wound depth, dressing allocated, and time from admission to reconstructive surgery. The model had an accuracy of 82%. The use of NPWT, compared with the traditional dressing, increased the chance of successful short-term healing by nearly six times (OR = 5.993; 95% CI: 1.058–33.962). Furthermore, each additional day of the time between the first day of hospitalization and the first reconstructive surgery reduced successful short-term healing by 6.5% (OR = 0.935, 95% CI: 0.889–0.985). Finally, wounds affecting the bone and subcutaneous layer, in comparison to lesions affecting the muscular layer, had a higher success rate in short-term healing (OR = 25.921, p = 0.011; and OR = 19.223, p = 0.037; respectively), as shown in ►Table 5.
| Variable | Short-term full wound closure, %(n) | p-value | OR (95% CI) |
|---|---|---|---|
| Vacuum dressinga | 83.3% (15) | 0.043* | 5.993 (1.058–33.962) |
| Injury depth | |||
| Muscular | 46% (11) | – | – |
| Dermisb | 100% (1) | 0.995 | – |
| Subcutaneousb | 57% (4) | 0.037* | 19.223 (1.191–310.275) |
| Boneb | 83% (15) | 0.011* | 25.921 (2.131–315.286) |
| Length of stay until surgery, days (x̅ ± SD) | 29.7 ± 23 | 0.011* | 0.935 (0.889–0.985) |
| Closure (x̅ ± SD) | 24.48 ± 15.28 | – | – |
| No closure (x̅ ± SD) | 38.81 ± 30.42 | – | – |

Discussion
Traumatic wounds include a group of acute wounds, usually extensive, associated or not with fractures. As a tool that stimulates the wound healing process, NPWT can be very useful in cases of trauma with loss of substance. This therapy works through the direct effect of macro and micromechanical deformations in all layers of the injury.
Macrodeformations are caused by the negative pressure itself on the edges of the wound, creating centripetal forces that help with the contraction and reduction of the wounds’ dimensions. Microdeformations, also on the edges of the wound, are the vacuum forces acting on the cytoskeleton, promoting cell division and migration, release of growth factors (with direct influence on angiogenesis and formation of granulation tissue), and reduction of inflammatory cells and markers. The drainage of exudate provided by the equipment reduces edema, toxic substrates, and bacterial load.7,8,14–17
These beneficial effects accelerate the wound healing process, enabling less complex reconstruction in many cases, possibly leading to a higher success rate in the NPWT group of the study in short-term closure (15 days), with 62% of all wounds having healed by the end of this period. In studies involving other types of complex wounds, the use of NPWT has been shown to be effective in healing pressure ulcers,18 as well as healing diabetic foot ulcers and reducing the length of hospital stay.19 In our previous experience, this dressing also boosted a high granulation tissue in wound dehiscence and Fournier gangrene.20 However, these comparisons between NPWT and traditional dressings, especially in traumatic wounds, have been rarely evaluated in studies of vacuum therapy.8–10,21
A factor that directly impacts on the evolution and outcome of wounds is the time between the patient’s arrival at the emergency room and the request of plastic surgery’s consultation. For our 33 patients, the average time between admission and the first evaluation by the team was 9 days, but other studies have shown a range from 7 to 39 days.3,22,23
Unfortunately, this long interval goes against the consensus in the literature, which shows that wounds with significant soft tissue involvement should be addressed within approximately 12 to 72 hours.5,24 Early coverage of open wounds reduces hydroelectrolytic disturbances, as well as basal energy expenditure, the need for dressing changes, costs, anesthetic risk, length of hospital stay, and functional sequelae.5 However, even after this critical period, it is still possible to obtain satisfactory results with microsurgical flaps.23
Another relevant interval was between the day of hospital admission and the final reconstructive surgery, since our study demonstrated that each additional day of hospitalization until reconstruction reduced short-term healing success by 6.5%.
In other similar studies, the average of this time interval can reach up to 48.15 days.3 In our study, we obtained an average of 1 month for this interval. This is probably related to both the delay in requesting a plastic surgery team for the first evaluation (average of 9 days) and the dressing time before reconstructive surgery (average of 16 days), either to delimit the area of necrosis of the wound, or due to changes of the vacuum dressing every 48 to 72 hours.8,14 One proposal to counterbalance these factors would be to call the plastic surgery team earlier, as previously mentioned.
There are concerns that the use of NPWT would further delay reconstructive surgery. In our study, the median was lower, at 9 days, but it was not statistically significant. Other studies on the use of NPWT have also shown no difference in dressing time in comparison with wounds treated with traditional dressings for reconstructive surgery,25 or, even with a longer time. In traumatic wounds they had rates of 90 to 100% of full wound closure in the short term (10–12 days).16,26 Diehm et al.27 showed that the use of NPWT in dermal substitutes (DS) reduced the mean time of application for STSG by 4.67 days (p = 0.031) and total healing by 6.16 days (p = 0.00015), thus achieving closure in approximately 4.77 days.
Another relevant finding was the relation between the depth affected of lesion and short-term healing success. Wounds that reached the bone layer had a higher success rate in healing than those that reached other layers, besides dermis. Although this result seems contradictory, given shallower injuries would be expected to have faster positive outcome, it is probably associated with the fact that wounds that affected the bone layer were more commonly treated with NPWT dressings, leading to shorter treatment times until improvement of the injury and until reconstructive surgery was performed. This means that use of NPWT can be more significant than depth in determining wound resolution.
This is so because, in our study, allocation to the vacuum therapy group, compared with the traditional dressing group, increased the chance of successful short-term healing by almost six times. Similar studies have shown shorter treatment time in acute and chronic wounds (15.3 days NPWT vs. 36.5 days control, p = 0.013) with the vacuum dressing.28 Other studies indicate that, in lower limb ulcers, there is a higher closure rate in the NPWT group (OR = 2.63; 95% CI: 1.87–3.70), with this proportion increasing the earlier the dressing is applied (OR = 3.38 for early and 2.18 for intermediate).29
Regarding the stepping down in complexity, this has been poorly and indirectly evaluated in studies, but there may be an association with mechanisms already mentioned.10,30 In our study, the traditional group presented a reduction in complexity at 18.75% in the reconstructive ladder and maintenance of the type at 71.88%, while in the NPWT group there was a 61.1% reduction and only 33.4% maintenance. Furthermore, even with access to a qualified team, out of the 13 lesions that were candidates for microsurgical flaps, none were performed.
Argenta and Morykwas had already initially shown that acute and subacute wounds treated with NPWT did not require microsurgical flaps.7 Other studies have also shown greater use of STSG for lesions treated with vacuum, ranging from 56 to 61.1%, similar to our result,26,31 which is higher than the 32.69% in our previous work.20 Thus, showing a possible impact of NPWT in reducing the complexity of reconstruction.
Our study has some limitations. The hospital has only three NPWT machines, which is incompatible with a referral service in trauma, with nursing and plastic surgery teams specializing in managing complex traumatic wounds. This would explain the preference for using NPWT for deeper lesions with exposed bone, and why only 36% of the traumatic wounds received this treatment, though still higher than that of our previous experience (15.38%).20
Additionally, a clinical trial was not conducted to assess whether wounds that are candidates for the same reconstructive technique would have changes in the final result when using NPWT. The results found here highlight an association based on experts’ opinion, and not a direct cause-effect. Vacuum therapy should be considered a great ally in plastic surgery,1 and its high initial cost is offset in the long term by positive outcome in wound management,30,32,33 or can be reduced with low-cost models.28,34
Additionally, studies with a larger number of evaluated wounds and a longer follow-up period are necessary to determine longer-term comparisons between vacuum therapy and traditional dressings, regarding healing of difficultto-manage wounds, reconstructive ladder, total length of hospital stay, hospital costs, as well as complications and sequelae.
Conclusion
The length of hospital stay for patients with traumatic limb injuries has a direct negative influence on the success rate of reconstruction. Therefore, systematization of care with early assessment by the plastic surgery team should be a priority.
The use of NPWT led to a higher success rate in the management of these wounds in the short term, and it reduced complexity in the reconstructive ladder, but did not impact on the number of surgical procedures required. Its use should always be considered in the management of trauma in limbs with soft tissue loss.
Acknowledgments
The present paper was part of PMN’s undergraduate research program for Sociedade Brasileira de Cirurgia Plástica under ALBP’s supervision.
REFERENCES
1. Coltro PS, Ferreira MC, Batista BPdSN, Nakamoto HA, Milcheski DA, Tuma P Jr. Atuação da cirurgia plástica no tratamento de feridas complexas [Role of plastic surgery on the treatment complex wounds]. Rev Col Bras Cir 2011;38(06):381–386. Doi: 10.1590/s0100-69912011000600003
2. Costa ML, Achten J, Knight R, et al; WHIST Trial Collaborators. Effect of Incisional Negative Pressure Wound Therapy vs Standard Wound Dressing on Deep Surgical Site Infection After Surgery for Lower Limb Fractures Associated With Major Trauma: The WHIST Randomized Clinical Trial. JAMA 2020;323(06):519–526. Doi: 10.1001/jama.2020.0059 Erratum in: JAMA 2021;326(3):279 DOI: 10.1001/jama.2021.7433
3. Motoki TH, Carvalho KC, Vendramin FS. Perfil de pacientes vítimas de trauma em membro inferior atendidos pela equipe de cirurgia reparadora do Hospital Metropolitano de Urgência e Emergência [A profile of patients with lower limb trauma treated by the Hospital Metropolitano de Urgência e Emergência reconstructive surgery team]. Rev Bras Cir Plást 2013;28(02):276–281. Doi: 10.1590/S1983-51752013000200018
4. Santos LFS, Fonseca JMA, Cavalcante BLS, Lima CM. Estudo epidemiológico do trauma ortopédico em um serviço público de emergência [Epidemiologic of orthopedic trauma study in a public emergency]. Cad Saude Colet 2016;24(04):397–403. Doi: 10.1590/1414-462X201600040128
5. Mello DF, Assef JC, Soldá SC, Helene A Jr. Degloving injuries of trunk and limbs: comparison of outcomes of early versus delayed assessment by the plastic surgery team. Rev Col Bras Cir 2015;42 (03):143–148. Doi: 10.1590/0100-69912015003003
6. Milcheski DA, Ferreira MC, Nakamoto HA, Pereira DD, Batista BN, Tuma P Jr. Uso da terapia por pressão subatmosférica em feridas traumáticas agudas [Subatmospheric pressure therapy in the treatmentof traumatic soft tissue injuries]. Rev Col Bras Cir 2013;40(05): 392–397. Doi: 10.1590/s0100-69912013000500008
7. Argenta LC, Morykwas MJ. Vacuum-assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg 1997;38(06):563–576, discussion 577
8. Poteet SJ, Schulz SA, Povoski SP, Chao AH. Negative pressure wound therapy: device design, indications, and the evidence supporting its use. Expert Rev Med Devices 2021;18(02): 151–160. Doi: 10.1080/17434440.2021.1882301
9. Iheozor-Ejiofor Z, Newton K, Dumville JC, Costa ML, Norman G, Bruce J. Negative pressure wound therapy for open traumatic wounds. Cochrane Database Syst Rev 2018;7(07):CD012522. Doi: 10.1002/14651858.CD012522.pub2
10. Krug E, Berg L, Lee C, et al; International Expert Panel on Negative Pressure Wound Therapy [NPWT-EP]. Evidence-based recommendations for the use of Negative Pressure Wound Therapy in traumatic wounds and reconstructive surgery: steps towards an international consensus. Injury 2011;42(Suppl 1):S1–S12. Doi: 10.1016/S0020-1383(11)00041-6
11. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JPSTROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 2007;370 (9596):1453–1457. Doi: 10.1016/S0140-6736(07)61602-X
12. Brandão CM, Weimann ETdS, Terzian LR, Machado CDS Filho, Paschoal FM, Criado PR. Menos é mais: estudo das diferentes formas de fechamento de feridas operatórias após cirurgia micrográfica de Mohs [Keep it simple. A ten-year experience in reconstructions after Mohs micrographic surgery]. An Bras Dermatol 2020;95(06):714–720. Doi: 10.1016/j.abd.2020.05.004
13. Divine G, Norton HJ, Hunt R, Dienemann J. Statistical grand rounds: a review of analysis and sample size calculation considerations for Wilcoxon tests. Anesth Analg 2013;117(03): 699–710. Doi: 10.1213/ANE.0b013e31827f53d7
14. Lima RVKS, Coltro PS, Farina JA Jr. Negative pressure therapy for the treatment of complex wounds. Rev Col Bras Cir 2017;44(01): 81–93. Doi: 10.1590/0100-69912017001001
15. Normandin S, Safran T, Winocour S, et al. Negative pressure wound therapy: mechanism of action and clinical applications. Semin Plast Surg 2021;35(03):164–170. Doi: 10.1055/s-0041-1731792
16. Bassetto F, Lancerotto L, Salmaso R, et al. Histological evolution of chronic wounds under negative pressure therapy. J Plast Reconstr Aesthet Surg 2012;65(01):91–99. Doi: 10.1016/j.bjps.2011.08.016
17. Chen L, Li G, Liu S, et al. Comparison of negative pressure wound therapy and conventional therapy for cranial bone-exposed wounds in rabbits. Ann Plast Surg 2017;79(04):397–403. Doi: 10.1097/SAP.0000000000001074
18. Sahin E, Rizalar S, Özker E. Effectiveness of negative-pressure wound therapy compared to wet-dry dressing in pressure injuries. J Tissue Viability 2022;31(01):164–172. Doi: 10.1016/j. jtv.2021.12.007
19. Wu Y, Shen G, Hao C. Negative pressure wound therapy (NPWT) is superior to conventional moist dressings in wound bed preparation for diabetic foot ulcers: A randomized controlled trial. Saudi Med J 2023;44(10):1020–1029. Doi: 10.15537/smj.2023.44.20230386
20. Berri DT, Freitas RS, Salles GS Jr, Balbinot P, Lopes MAC, Scomação I. Experiência do grupo de feridas complexas da disciplina de cirurgia plástica do hospital de clínicas e hospital do trabalhador de Curitiba. Arq Catarin Med 2012;41:1–6
21. Kunze KN, Hamid KS, Lee S, Halvorson JJ, Earhart JS, Bohl DD. Negative-Pressure wound therapy in foot and ankle surgery. Foot Ankle Int 2020;41(03):364–372. Doi: 10.1177/1071100719892962
22. Macedo JLS, Rosa SC, Botelho DL, Santos CPd, Queiroz MNd, Gomes TGACB. Lower extremity reconstruction: epidemiology, management and outcomes of patients of the Federal District North Wing Regional Hospital. Rev Col Bras Cir 2017;44(01):9–16. Doi: 10.1590/0100-69912017001003
23. Steiert AE, Gohritz A, Schreiber TC, Krettek C, Vogt PM. Delayed flap coverage of open extremity fractures after previous vacuum-assisted closure (VAC) therapy - worse or worth? J Plast Reconstr Aesthet Surg 2009;62(05):675–683. Doi: 10.1016/j.bjps.2007.09.041
24. Godina M. Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986;78(03):285–292. Doi: 10.1097/00006534-198609000-00001
25. Yin R, Gursky A, Falade I, et al. The utility of Prevena negative pressure wound therapy on groin incisions for critical limbthreatening ischemia. Ann Plast Surg 2024;92(5S, Suppl 3) S331–S335. Doi: 10.1097/SAP.0000000000003802
26. Gabriel A, Heinrich C, Shores J, et al. Outcomes of vacuum-assisted closure for the treatment of wounds in a paediatric population: case series of 58 patients. J Plast Reconstr Aesthet Surg 2009;62 (11):1428–1436. Doi: 10.1016/j.bjps.2008.06.033
27. Diehm YF, Fischer S, Gazyakan E, et al. Negative pressure wound therapy as an accelerator and stabilizer for incorporation of artificial dermal skin substitutes - A retrospective, non-blinded, and non-randomized comparative study. J Plast Reconstr Aesthet Surg 2021;74(02):357–363. Doi: 10.1016/j.bjps.2020.08.041
28. Hariri M, Maaz B, Natfagi M, et al. Validation of a manual negative pressure wound therapy device (PragmaVAC) for acute and chronic wounds: a prospective, randomized, controlled trial. World J Surg 2022;46(12):2946–2953. Doi: 10.1007/s00268-022-06713-8
29. Yao M, Fabbi M, Hayashi H, et al. A retrospective cohort study evaluating efficacy in high-risk patients with chronic lower extremity ulcers treated with negative pressure wound therapy. Int Wound J 2014;11(05):483–488. Doi: 10.1111/j.1742-481X.2012.01113.x
30. Birke-Sorensen H, Malmsjo M, Rome P, et al; International Expert Panel on Negative Pressure Wound Therapy [NPWT-EP]. Evidence-based recommendations for negative pressure wound therapy: treatment variables (pressure levels, wound filler and contact layer)–steps towards an international consensus. J Plast Reconstr Aesthet Surg 2011;64(Suppl):S1–S16. Doi: 10.1016/j.bjps.2011.06.001
31. Mouës CM, van den Bemd GJCM, Heule F, Hovius SER. Comparing conventional gauze therapy to vacuum-assisted closure wound therapy: a prospective randomized trial. J Plast Reconstr Aesthet Surg 2007;60(06):672–681. Doi: 10.1016/j.bjps.2006.01.041
32. Ferraz EM, Lira CHA, Martins JPC, Maricevich JP, Pradines SMS, Granja LG Filho. Uso do sistema VAC no tratamento da fascite necrosante da parede abdominal [Vacuum assisted closure sistem in the treatment of necrotizing fasciitis of abdominal wall]. Rev Col Bras Cir 2007;34 (04):264–271. Doi: 10.1590/S0100-69912007000400012
33. Mouës CM, van den Bemd GJ, Meerding WJ, Hovius SE. An economic evaluation of the use of TNP on full-thickness wounds. J Wound Care 2005;14(05):224–227. Doi: 10.12968/jowc.2005.14.5.26776
34. Souza SC, Mendes CMC, Meneses JVL, Menezes RD. Curativo a vácuo simplificado: estudo de viabilidade operacional e financeira no tratamento de feridas [Simplified vacuum dressing system: operational and financial feasibility study in the management of wounds]. Rev Bras Cir Plast 2023;38(03):e0731. Doi: 10.5935/2177-1235.2023RBCP0731-EN
1. Department of Plastic Surgery, Complexo Hospitalar do Trabalhador (CHT), Curitiba,
PR, Brazil
2. Department of Medicine, Universidade Positivo (UP), Curitiba, PR, Brazil
3. Department of Medicine, Pontifícia Universidade Católica do Paraná (PUCPR), Curitiba,
PR, Brazil
4. Department of Plastic Surgery, Complexo do Hospital de Clínicas, Universidade Federal
do Paraná (CHC-UFPR), Curitiba, PR, Brazil
Address for correspondence Pietro Maran Novais, Complexo Hospitalar do Trabalhador, Avenida República Argentina, 4406–Novo Mundo, Curitiba – PR, CEP: 81050-000, Brazil (e-mail: pietromarannovais@gmail.com).
Article received: October 12, 2025.
Article accepted: November 24, 2025.
Conflict of Interests The authors have no conflict of interests to declare.
Editor-in-Chief: Dov Charles Goldenberg.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket