



Original Article - Year 2026 - Volume 41Issue 1
Latissimus Dorsi Thoracolateral Flap: A New Option for Total Autologous Breast Reconstruction
Retalho do músculo latíssimo do dorso toracolateral (LDTL): Uma nova opção para a reconstrução autóloga da mama
Eduardo Montag1, ; Eduardo Gustavo Pires de Arruda2; Leonardo Martinez Domingues3; Esther Mihwa Choi1; Thiago Ueda1; Alexandre Mendonça Munhoz1; Fábio de Freitas Busnardo3; Rolf Gemperli3
; Eduardo Gustavo Pires de Arruda2; Leonardo Martinez Domingues3; Esther Mihwa Choi1; Thiago Ueda1; Alexandre Mendonça Munhoz1; Fábio de Freitas Busnardo3; Rolf Gemperli3
ABSTRACT
Introduction Mastectomy for breast cancer has a significant psychological impact, making breast reconstruction an essential component of comprehensive care. Techniques using tissue expanders and implants have become widely adopted due to their accessibility; however, they may be associated with complications such as capsular contracture, infection, and implant rupture. In contrast, autologous reconstruction provides greater naturalness, consistency, and long-term durability. The latissimus dorsi musculocutaneous flap, first described by Tansini and popularized in the 1970s, has evolved through technical modifications and the incorporation of fat grafting, enabling its use as a standalone method. The thoracolateral latissimus dorsi (TLLD) flap was introduced in 2016. The current study describes its anatomical characteristics, surgical technique, and clinical outcomes.
Materials and Methods The present descriptive study was based on a review of medical records and a prospective database of patients who underwent breast reconstruction with the TLLD flap at Instituto do Câncer do Estado de São Paulo (ICESP) between 2017 and 2023.
Results In total, 95 patients underwent surgery, with a mean age of 43.5 years and a mean body mass index (BMI) of 32.8 kg/m2. Delayed reconstruction was performed in 70% of the cases. The main indications were recurrent capsular contracture, implant infection or rupture, and contraindication to abdominal flaps. Fat grafting was performed in 16% of the patients. Complications, including seroma, wound dehiscence, and epidermolysis, occurred in 11 cases.
Conclusion The LDTL flap proved to be an effective and safe alternative for breast reconstruction, particularly in cases of previous reconstructive failure or complications related to alloplastic materials, establishing itself as a versatile salvage technique.
Keywords: breast neoplasms; mammaplasty; surgical flaps; myocutaneous flap; anatomy
RESUMO
Introdução A mastectomia para o tratamento do câncer de mama provoca grande impacto psicológico, e a reconstruçãomamária é fundamental. As técnicas com expansores e implantes se popularizaram pelo fácil acesso, mas podem apresentar complicações como contratura capsular, infecção e ruptura. Em contrapartida, as reconstruções autólogas oferecem naturalidade, consistência e durabilidade. O retalho miocutâneo do músculo latíssimo do dorso, descrito por Tansini e difundido na década de 1970, evoluiu com modificações técnicas e o uso de lipoenxertia, o que possibilita o seu emprego isolado. Em 2016, foi proposta uma variação: o retalho do músculo latíssimo do dorso toracolateral (LDTL), que expandiu as indicações para a reconstrução total da mama. Este estudo descreve as suas características, a técnica cirúrgica e os resultados clínicos.
Materiais e Métodos Trata-se de estudo descritivo, baseado na revisão de prontuários de pacientes submetidas à reconstrução como retalho LDTL no Instituto do Câncer do Estado de São Paulo (ICESP) entre 2017 e 2023.
Resultados Ao todo, foram operadas 95 pacientes, com idade média de 43,5 anos e índice de massa corporal (IMC) médio de 32,8 kg/m2. A reconstrução tardia foi realizada em 70% dos casos. As principais indicações foram contratura capsular recidivante, infecção ou ruptura de implantes e impossibilidade de uso de retalhos abdominais. A lipoenxertia foi aplicada em 16% das pacientes. Complicações, incluindo seroma, deiscência e epidermólise, ocorreram em 11 casos.
Conclusão O retalho LDTL demonstrou ser alternativa eficaz e segura para a reconstrução mamária, especialmente em situações de falhas reconstrutivas ou complicações associadas a materiais aloplásticos, de modo que se configura como técnica versátil e de resgate.
Palavras-chave: neoplasias da mama; mamoplastia; retalho miocutâneo; retalhos cirúrgicos; anatomia
Introduction
The psychological impact of breast loss on the mental health of women undergoing treatment for breast cancer is immea-surable. Breast reconstruction is an integral component of comprehensive breast cancer treatment, providing physical and psychological benefits.
The advent of reconstructive techniques using alloplastic materials has enabled broader access to reconstruction for many women. Despite the technological advances in the development of tissue expanders and implants, reconstruction with these materials may result in complications, including capsular contracture, rupture, infection, and loss of esthetic outcome, which may compromise patients’ quality of life.
Autologous reconstruction provides several advantages, including greater naturalness, consistency, and long-term maintenance of results. Multiple studies comparing autolo-gous and alloplastic reconstructions demonstrate the advan-tages of flap-based techniques with respect to quality of life and durability of outcomes.
The latissimus dorsi musculocutaneous flap was first described by Tansini,1 and it became widely-adopted in the 1970s in association with implants for volume augmen-tation. Subsequent modifications in flap design, dissection technique, and incorporation of fat grafting enabled breast-volume reconstruction using the flap in isolation, without the need for implants.
In 2016 at our institution, Arruda proposed a modification to the flap design, incorporating the cutaneous portion located anteriorly to the anterior border of the muscle. This new design expanded the indications for total breast reconstruction. The modified flap was named TLLD, reflecting the combination of the thoracolateral flap and the latissimus dorsi flap.
Objective
The current study aims to describe the anatomical character-istics of the TLLD flap, the technical aspects of the surgical dissection, the complications, and the main indications.
Methods
The present descriptive study was based on a review of data obtained from a prospectively-maintained database and the medical records of patients who underwent breast recon-struction using the TLLD flap at Instituto do Câncer do Estado de São Paulo (ICESP) from 2017 to 2023.
Flap design
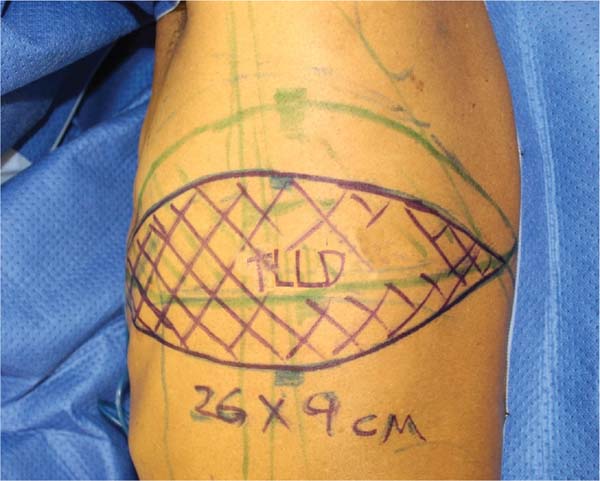
With the patient in the standing position, anatomical land-marks are delineated, including the inferior border of the scapula, the posterior axillary line, and the posterosuperior iliac spine. The flap axis corresponds to the projection of the inframammary fold. The cutaneous component extends from the dorsal midline to the midmammary line, following the specific indication in each case. A bidigital pinch test deter-mines the appropriate width of the cutaneous portion of the flap (►Fig. 1).


Dissection technique
With the patient in lateral decubitus, infiltration is per-formed using an anesthetic solution containing epinephrine at a concentration of 1:100 thousand throughout the planned incision area. Flap elevation is initiated superiorly in the plane superficial to the muscle, with creation of a subcutaneous tunnel toward the breast when indicated. The segment located anteriorly to the border of the latissimus dorsi muscle is dissected in the subfascial plane. Dissection then proceeds distally until an adequate amount of muscular tissue is obtained, according to the requirements of each case. Following division of the distal portion, dissection continues along the deep surface of the muscle toward the vascular pedicle. After ligation of the branch to the serratus anterior muscle, the main pedicle is isolated, and the thor-acodorsal nerve is divided. The humeral insertion is subse-quently released, and the flap is rotated into the breast region (►Figs. 2-3). The inset is performed using absorbable sutures. The donor site is closed with the aid of adhesion sutures using VICRYL 2-0 (Ethicon Inc.). A #15 Blake drain (Ethicon Inc.) is placed in the reconstructed breast and axillary tunnel. The tendinous portion of the muscle is secured to the lateral chest wall to protect the vascular pedicle (►Fig. 4).





Results
Between 2017 and 2023, 95 patients underwent reconstruc-tion using this technique. They had a mean age of 43.5 (range: 34-75) years, and a mean body mass index (BMI) of 32.8 (range: 22.5-34.2) kg/m2. In total, 12 patients were smokers, and 83 were non-smokers. Overall, 75% of the patients presented with at least 1 comorbidity, including arterial hypertension, diabetes, hypothyroidism, and cardiac conditions.
Most reconstructions were performed in the delayed setting (70%), whereas 30%, at the time of mastectomy. The main indications for the technique were recurrent capsular contracture, expander/implant infection, rupture, desire to change the reconstructive method, failure of another autol-ogous flap, and comorbidities precluding the use of an abdominal flap, such as morbid obesity.
A total of 15 patients (16%) underwent fat grafting of the flap, with injected volumes ranging from 90 to 200 mL. The de-epithelialized area was total in 54 cases (56%) and partial in 41 (44%). Flap dimensions ranged from 22 to 49 cm in length and from 8 to 18 cm in width.
Eleven patients developed complications, including do-nor-site seroma (2 cases), epidermolysis (3 cases), wound dehiscence (2 cases), wound infection (1 case), and vascular compromise (3 cases), including one case of venous conges-tion and one case of partial necrosis (4 × 2 cm).
Discussion
Despite its description in the early twentieth century,1,3 the latissimus dorsi flap was popularized for breast reconstruc-tion by Bostwick et al.2 in 1978. Numerous modifications have since been described, expanding its indications.
Its consistent anatomy and robust vascularization enable its application in various breast and thoracic reconstructive scenarios. It may be used as a muscular, musculocutaneous, or osteomyocutaneous flap.
Following its initial description in breast reconstruction, several authors introduced modifications aimed at increas-ing flap dimensions and volume. In 1987, Hokin and Silfver-skiold4 proposed the inclusion of the lumbar fascia. In 1996, Germann and Steinau5 reported inclusion of the scapular fascia and fat. In 1998, Papp and McCraw6 described enlarge-ment of the cutaneous component using an anchor-shaped incision. In 1995, Angrigiani et al.7 presented the extended thoracodorsal artery perforator flap, incorporating the scap-ular and lumbar fasciae. In 2012, Tame and Ledo8 described the dorsum-epigastric flap, expanding the limits of the cutaneous portion while reducing the muscular component used. In 2019, Koonce et al.9 incorporated indocyanine green angiography and defined vascular territories within the cutaneous portion. In 1996, Barnett and Gianoutsos10 reported the use of fat grafting for volumetric augmentation, thereby eliminating the need for implants.
The design modification described in the present study encompasses the lateral thoracic region, incorporating the cutaneous portion of the lateral thoracic flap (Holmström and Lossin, 1986).11 The extent of the muscular component is variable and depends on individual patient requirements. The tendinous portion located near the posterosuperior iliac spine should not be included because it has relatively limited vascularization, represents a suboptimal recipient bed for fat grafting, and increases the risk of lumbar hernia.12 In addi-tion to volumetric enhancement of the flap, mobilization of tissue from the lateral region may improve regional body contour in obese patients or those with excess lateral skin and adiposity.
The dimensions of the cutaneous portion, the volume of the adipose pad, and the possibility of fat grafting enabled fully-autologous reconstruction, achieving natural results with breast symmetry. The indications for the flap include immediate and delayed reconstructions requiring volume and/or cutaneous coverage. Among the procedures per-formed, 36 patients underwent removal of an expander or implant with replacement by the flap due to infection, rupture, exposure, or capsular contracture. The contraindi-cations are consistent with those of the traditional latissimus dorsi flap, and they include prior thoracic surgeries with incisions within the flap territory and previous ligation of the vascular pedicle.
The advantages of the TLLD flap include rapid dissection, technical simplicity, avoidance of a microsurgical procedure, adequate flap volume, and reduced donor-site morbidity compared with pedicled abdominal flaps. The main disad-vantage is the presence of a dorsal scar; however, this scar is linear and positioned at bra level, according to the flap design. Other disadvantages, such as decreased shoulder strength and flap atrophy, are well established in the literature.
A subgroup warranting particular attention consists of patients with morbid obesity, who, due to specific characteristics such as increased breast volume, ptosis, and elevated intra-abdominal pressure, are poor candi-dates for reconstruction using either alloplastic materials or abdominal flaps. Flap use enables total reconstruction of large and ptotic breasts without the risks of abdominal hernia or complications associated with alloplastic materials.
In the present study, the overall complication rate was of 32%. The complications were either minor, including epi-dermolysis, wound dehiscence (a single case required resu-turing under local anesthesia), wound infection, and donor-site seroma (8%), or major, such as vascular compromise (5%). No flap loss occurred. These findings are consistent with those of previously-published studies that report complica-tion rates of up to 34.9%.
According to Pirro et al. (2017),13 patients undergoing breast reconstruction with autologous tissue report greater satisfaction with the breast outcomes compared with alloplastic reconstruction after the application of the BREAST-Q. This satisfaction is attributed to more durable and predictable results, improved outcomes in patients with complex cases and/or undergoing radiation therapy, and absence of anaplastic large cell lymphoma risk.
Conclusion
The TLLD flap is an option for immediate or delayed autolo-gous breast reconstruction. It represents an additional sal-vage alternative in patients with prior reconstructive failure, infection related to alloplastic materials, or recurrent capsu-lar contracture.
References
1. Tansini I. Sopra il mio nuovo processo di amputazione della mamella. Riforma Med 1906;12:757
2. Bostwick J III, Vasconez LO, Jurkiewicz MJ. Breast reconstruction after a radical mastectomy. Plast Reconstr Surg 1978;61(05): 682-693. Doi: 10.1097/00006534-197805000-00004
3. Maxwell GP. Iginio Tansini and the origin of the latissimus dorsi musculocutaneous flap. Plast Reconstr Surg 1980;65(05): 686-692. Doi: 10.1097/00006534-198005000-00027
4. Hokin JA, Silfverskiold KL. Breast reconstruction without an implant: results and complications using an extended latissimus dorsi flap. Plast Reconstr Surg 1987;79(01):58-66
5. Germann G, Steinau HU. Breast reconstruction with the extended latissimus dorsi flap. Plast Reconstr Surg 1996;97(03):519-526. Doi: 10.1097/00006534-199603000-00004
6. Papp C, McCraw JB. Autogenous latissimus breast reconstruction. Clin Plast Surg 1998;25(02):261-266
7. Angrigiani C, Grilli D, Siebert J. Latissimus dorsi musculocuta-neous flap without muscle. Plast Reconstr Surg 1995;96(07): 1608-1614. Doi: 10.1097/00006534-199512000-00014
8. Tame JLH, Ledo GJM. Descripción anatómico-quirúrgica del col-gajo dorsoepigástrico: una opción diferente en reconstrucción mamaria. Cir Plást Iberolatinoam 2012;38(01):27-34. Doi: 10.4321/S0376-78922012000100003
9. Koonce SL, Barnavon Y, Newman MI, Hwee YK. Perfusion Zones of Extended Transverse Skin Paddles in Muscle-Sparing Latissimus Dorsi Myocutaneous Flaps for Breast Reconstruction. Plast Reconstr Surg 2019;143(05):920e-926e. Doi: 10.1097/PRS.0000000000005520
10. Barnett GR, Gianoutsos MP. The latissimus dorsi added fat flap for natural tissue breast reconstruction: report of 15 cases. Plast Reconstr Surg 1996;97(01):63-70. Doi: 10.1097/00006534-199601000-00010
11. Holmström H, Lossing C. The lateral thoracodorsal flap in breast reconstruction. Plast Reconstr Surg 1986;77(06):933-943. Doi: 10.1097/00006534-198606000-00010
12. Munhoz AM, Montag E, Arruda EG, Sturtz G, Gemperli R. Man-agement of giant inferior triangle lumbar hernia (Petit’s triangle hernia): A rare complication following delayed breast reconstruc-tion with extended latissimus dorsi myocutaneous flap. Int J Surg Case Rep 2014;5(06):319-323. Doi: 10.1016/j.ijscr.2014.03.026
13. Pirro O, Mestak O, Vindigni V, et al. Comparison of Patient-reported Outcomes after Implant Versus Autologous Tissue Breast Reconstruction Using the BREAST-Q. Plast Reconstr Surg Glob Open 2017;5(01):e1217. Doi: 10.1097/GOX.0000000000001217
1. Breast Reconstruction Group, Instituto do Câncer do Estado de São Paulo, São Paulo,
SP, Brazil
2. Private Practice, São Paulo, SP, Brazil
3. Plastic Surgery Program, Hospital das Clínicas da Faculdade de Medicina da Universidade
de São Paulo, São Paulo, SP, Brazil
Address for correspondence Eduardo Montag, Avenida Doutor Arnaldo 251, Cerqueira César, São Paulo, SP, CEP: 01246-000, Brazil (e-mail: e.montag@hc.fm.usp.br e.montag@mac.com).
Artigo submetido: 20/03/2025.
Artigo aceito: 15/12/2025.
Editor-in-Chief: Dov Charles Goldenberg.
Conflict of Interests
The authors have no conflict of interests to declare.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket