



Original Article - Year 2026 - Volume 41Issue 1
Oncoplastic Reconstruction of the Contralateral Breast Using the Liacyr Pedicle without Prosthetic Implants
Reconstrução oncoplástica da mama contralateral com pedículo de Liacyr não associado a próteses
Ivan Demolinari de-Miranda1, ; Gabriel Neves dos Santos Mosqueira Gomes1; Ana Beatriz Gomes Almeida1; João Medeiros Tavares-Filho1
; Gabriel Neves dos Santos Mosqueira Gomes1; Ana Beatriz Gomes Almeida1; João Medeiros Tavares-Filho1
ABSTRACT
Introduction Autologous breast reconstruction is advantageous as it can restore volume and skin defects, in addition to shaping the breast. Furthermore, with this reconstruction, there are no foreign bodies, which avoids patient exposure to risks and presenting a more natural-looking result. In this context, the Liacyr pedicle, a dermolipoglandular flap from the base of the breast, is commonly adopted. The literature praises it for its outcomes, technique, and wide range of applications, both in the reconstructive and esthetic contexts.
Objective To discuss the esthetic and functional outcomes of breast reconstruction using a Liacyr pedicle and no prostheses.
Materials and Methods The current retrospective, observational study is a case series involving 13 female patients submitted to breast reconstruction using Liacyr I or III pedicles. The objective esthetic analysis of the breasts used the "Breast Idea" web application, while the subjective analysis employed a questionnaire based on the BREAST-Q model.
Results In the BREAST-Q assessment, themedian value for simplified satisfaction with the breasts was of 71 (range: 0-100). The median psychosocial well-being score was of 87 (range: 0-100), with no significant difference between the groups. The questionnaire regarding satisfaction with the information provided by themedical teamyielded positive results, with amedian score of 85 (range: 0-100) and a mode of 100 (range: 0- 100).
Conclusion Breast reconstruction using autologous tissue is widely available, reproducible, and associated with low complication rates and high satisfaction levels.
Keywords: mammaplasty; quality of life; breast neoplasms; surgery, plastic; surgical flaps
RESUMO
Introdução A reconstrução autóloga da mama é vantajosa, pois pode restaurar o volume e os defeitos de pele, além de moldar o formato do seio. Além disso, com essa reconstrução, não há corpos estranhos ao organismo, o que evita a exposição do paciente a riscos e apresenta resultado de aspecto mais natural. Nesse contexto, o pedículo de Liacyr, retalho dermolipoglandular da base da mama, é comumente adotado. Na literatura, é consagrado por seus resultados, técnica e ampla possibilidade de aplicações, tanto no contexto reconstrutor quanto estético.
Objetivo Discutir os resultados estético e funcional da reconstrução mamária com pedículo de Liacyr sem o uso de próteses.
Materiais e Métodos Realizou-se um estudo observacional retrospectivo em uma série de casos de 13 pacientes do sexo feminino submetidas à reconstrução mamária com os pedídulos I ou III de Liacyr. A análise estética objetiva das mamas foi feita por meio do aplicativo da web "Breast Idea", e, para a análise subjetiva, foi aplicado um questionário desenvolvido a partir do modelo BREAST-Q.
Resultados Na avaliação do BREAST-Q, a mediana de satisfação simplificada com as mamas foi de 71 (variação: 0-100). No questionário sobre bem-estar psicossocial, a mediana foi de 87 (variação: 0-100), sem nenhuma diferença expressiva entre os grupos. O questionário sobre satisfação com a informação fornecida pela equipe médica tiveram os resultados muito positivos, com mediana de 85 (variação: 0-100), sendo a moda 100 (variação: 0-100).
Conclusão A reconstrução de mama com tecido autólogo é altamente disponível e reprodutível, e apresenta baixas taxas de complicação e boas taxas de satisfação.
Palavras-chave: mamoplastia; qualidade de vida; neoplasias da mama; cirurgia plástica; retalhos cirúrgicos
Introduction
Autologous breast reconstruction is advantageous because it can simultaneously restore volume and skin defects.1,2 It also enables sculpting the breast shape and, when successful, it can yield long-lasting outcomes.1 Autologous breast recon-struction is associated with greater longevity and higher success rates in complex cases.1 Furthermore, as it does not involve a foreign body, it offers a more natural esthetic result.1,2
The latissimus dorsi flap, adopted as the first step of the surgical reconstruction discussed in the current article, is a favorable option due to its accessibility and reliable vascular support. It includes skin, fat, muscle, and vascular supply, which contributes to high success rates and graft volume. This flap is safe and robust; however, it has disadvantages related to scarring and asymmetry, especially in cases of unilateral reconstruction.1
Tissue expanders are also suitable alternatives for the first surgical step, although they are more limited than the latissimus dorsi flap. More recent models incorporate sur-face texturing to prevent malposition and improve capsule quality, in addition to expanding the lower pole to achieve a more natural shape. However, the disadvantages include high cost, poor adherence in some patient groups, and limited volume.3
In this context, the Liacyr pedicle-a dermolipoglandular from the base of the breast-is commonly used to correct tissue insufficiency, and it has the additional advantage of minimizing breast rotation.4 The Liacyr pedicle, with its five categories, is widely accepted and provides excellent out-comes, even when associated with breast implants (►Table 1). It holds a prominent position in the literature,4 and it is well established due to its outcomes, technical reliability, and broad range of applications in reconstructive and esthetic contexts.
| Category | Features |
|---|---|
| Type-I Liacyr pedicle | Shape: rectangular Dimensions: approximately 9 x 6 x 3 cm (height, width, and thickness); Vasculature: 4th to 7th intercostal spaces (the 5th intercostal space is the main one) - perforating branches of the mammary artery |
| Type-III Liacyr pedicle | Shape: triangular or trapezoidal Dimensions: approximately 3 cm in thickness; its base extends from the horizontal branch to 2 to 3 cm from the areola-nipple complex (ANC); Vasculature: 5th to 7th intercostal spaces - perforating branches of the mammary |

Despite its high efficacy, its association with implants may increase the risks due to prosthesis-related limitations.4 The most significant complication is implant loss, often with wound dehiscence.
It is worth mentioning the risk of developing breast implant-associated anaplastic large cell lymphoma. Al-though rare, this complication from textured implants is highly concerning. Other types of implants, such as smooth implants, tend to provide limited esthetic outcomes and may also result in complications.3
Objective
The present study aims to discuss the esthetic and functional outcomes of breast reconstruction using the Liacyr pedicle with no prosthetic implants.
Materials and Methods
The current retrospective observational case series study involved 13 female patients aged 28 to 82 years who under-went surgery from January 2016 to January 2020 at the same institution (Hospital Alcides Carneiro, Petrópolis, Rio de Janeiro, Brazil). All patients had previously undergone mas-tectomy, with breast reconstruction in two to three surgical steps. Reconstruction initially involved either a latissimus dorsi flap or a tissue expander, followed by contralateral reconstruction with mastopexy without implants, and final-ized with nipple reconstruction performed either during the same procedure or in a third step.
The initial analysis considered all 16 patients who under-went reconstruction with type-I or -III Liacyr pedicles by the same surgical team (principal surgeon and assistant), re-gardless of tumor histological type. Two patients were excluded due to insufficient data and an inability to establish contact. One patient declined participation by refusing to sign the informed consent form (ICF). As a result, the final study population consisted of 13 women (►Fig. 1).
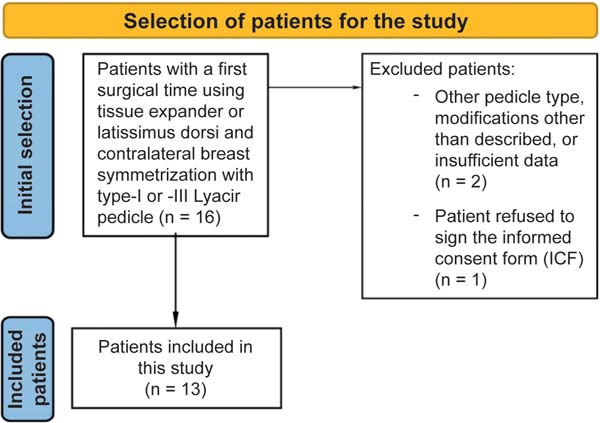

Table 2 presents the variables for analysis, including comorbidities, patient age, and body mass index (BMI). The objective esthetic evaluation of the breasts was performed using the web application “Breast Idea”, based on patient photographs and adopting the quick assessment model.
| Patient age (years) and initials | Body mass index (kg/m2) | Comorbidities | Histological type of the tumor | Type of flap | First surgical step |
|---|---|---|---|---|---|
| 68; TSE | 30.9 | DM and SAH | Invasive interductal papillary carcinoma | Liacyr I; size: 6 x 6 cm |
Latissimus dorsi |
| 54; AMM | NR | None | NR | Liacyr I; size: 8 x 9 cm |
Latissimus dorsi |
| 79; DPB | 27 | SAH | Infiltrative ductal carcinoma | Liacyr I; size: 10 x 10 cm |
Latissimus dorsi |
| 65; NMLG | 30.85 | SAH | Infiltrative ductal carcinoma | Liacyr I; size: 10 x 8 cm |
Latissimus dorsi |
| 66; JAC | NR | DM and SAH | NR | Liacyr I; size: 9 x 12 cm |
Latissimus dorsi |
| 49; AMS | NR | None | NR | Liacyr I; size: 8 x 12 cm |
Tissue expander |
| 50; CAO | 28.1 | None | NR | Liacyr I; size: 7 x 9 cm |
Tissue expander |
| 41; BBBG | NR | None | Infiltrative ductal carcinoma | Liacyr I; size: 8 x 12 cm |
Tissue expander |
| 61; MAQM | 30.8 | DM and SAH | NR | Liacyr III; size: 10 x 13 cm |
Latissimus dorsi |
| 82; OSC | NR | None | NR | Liacyr III; size: 6 x 8 cm | Latissimus dorsi |
| 76; GMS | NR | SAH | NR | Liacyr III; size: 17 x 14 cm |
Latissimus dorsi |
| 56; SLPC | NR | SAH | NR | Liacyr III; size: 10 x 17 cm |
Tissue expander |
| 28; ALRAT | NR | None | NR | Liacyr III; size: 9 x 11 cm |
Tissue expander |
Abbreviations: DM, Diabetes mellitus; NR, not reported; SAH, systemic arterial hypertension.

The subjective analysis was conducted using question-naires developed from the BREAST-Q model, which were administered between 3 and 5 years after surgery. We used four questionnaires that addressed different areas: physical and personal limitations (►Table 3), sexual activity and discomforts such as dry mouth and pain (►Table 4), overall satisfaction levels, including satisfaction with the surgeons (►Table 5), and a modified version of the Breast-Q that was translated to Portuguese (►Table 6).
| 1 - Not at all |
|---|
| 2 - A little |
| 3 - Very much |
| 4 - A lot |
| Any problems with strenuous activities? |
| Any problems with long walks? |
| Any problems with short walks? |
| Do you need to stay in bed or in a chair during the day? |
| Do you need help eating, cleaning yourself, and using the bathroom? |
| DURING THE PAST WEEK |
| Did you experience limitations in any daily activities? |
| Did you experience limitations during any hobbies? |
| Did you experience shortness of breath at any point? |
| Did you feel pain? |
| Did you need to rest? |
| Did you have any trouble sleeping? |
| Did you feel weak? |
| Did you lose your appetite? |
| Did you vomit at any point? |
| Did you experience constipation? |
| Did you have diarrhea? |
| Were you tired? |
| Did the pain interfere with your activities? |
| Did you have any difficulty concentrating? |
| Did you feel tense? |
| Were you worried about something? |
| Did you feel irritated? |
| Did you feel depressed? |
| Has your family life been affected by the illness? |
| Has your social life been affected by the illness? |
| Has your financial life been affected by the illness? |
| How would you rate your health over the past week (1-7)? |
| How would you rate your quality of life over the past week (1-7)? |

| DURING THE PAST WEEK: |
|---|
| Did you experience dry mouth? |
| Did foods or drinks taste different? |
| Did you have eye pain, irritation, or something similar? |
| Did you lose hair? |
| If you have experienced hair loss, did it stress you out? |
| Did you feel sick or unwell? |
| Did you experience hot flashes? |
| Did you experience a headache? |
| Did you feel less attractive? |
| Did you feel less feminine? |
| Did you have trouble looking at yourself in the mirror? |
| Are you dissatisfied with the outcome? |
| Are you worried about your future health? |
| DURING THE PAST MONTH: |
| Were you interested in sex? |
| Were you sexually active? |
| Did you feel please during intercourse? |
| DURING THE PAST WEEK: |
| Did you experience shoulder pain? |
| Did you experience upper limb swelling? |
| Did you experience pain in the affected breast area? |
| Did you have trouble raising your arms? |
| Was the breast area sore? |
| Were your breasts swollen? |
| Did you experience any skin problems on your breasts? |
| Did you sweat excessively? |
| Did you have mood swings? |
| Did you feel dizzy? |
| Did you have a sore throat? |
| Did you experience redness in your mouth? |
| Did you experience pain in your feet or hands? |
| Did you experience redness in your feet or hands? |
| Did you experience tingling in your feet or hands? |
| Did you experience numbness in your feet or hands? |
| Did you experience joint issues (pain)? |
| Did you gain weight? |
| Has weight gain been a problem? |
| DURING THE PAST MONTH |
| Did you experience vaginal dryness? |
| Did you experience any vaginal discomfort? |
| Did you experience pain during intercourse? |
| Did you experience vaginal dryness during intercourse? |
| DURING THE PAST WEEK |
| Were you satisfied with the esthetic outcome? |
| Were you satisfied with the quality of the reconstructed skin? |

| 1 - Very dissatisfied/uncomfortable/unimportant |
|---|
| 2 - Somewhat dissatisfied |
| 3 - Neither satisfied nor dissatisfied |
| 4 - Somewhat satisfied |
| 5 - Very satisfied |
| WHAT IS YOUR SATISFACTION LEVEL WITH: |
| Size during sex? |
| Size during leisure activities? |
| Size during work? |
| Shape during sex? |
| Shape during leisure activities? |
| Shape during work? |
| Firmness during sex? |
| Firmness during leisure time? |
| Firmness during work? |
| WHAT IS YOUR DISCOMFORT LEVEL WITH: |
| General appearance when dressed and alone? |
| General appearance when dressed and with your partner? |
| General appearance when dressed and with men in general? |
| General appearance when dressed and with women you know? |
| General appearance when dressed and with women you do not know well? |
| General appearance when dressed and with healthcare professionals? |
| HOW DO YOU FEEL ABOUT YOUR GENERAL APPEARANCE WEARING BIKINI/BEACHWEAR WHEN: |
| Alone? |
| With your partner? |
| With men in general? |
| With women you know? |
| With women you do not know well? |
| With healthcare professionals? |
| HOW DO YOU FEEL ABOUT YOUR GENERAL APPEARANCE WHEN NAKED AND: |
| Alone? |
| With your partner? |
| With men in general? |
| With women you know? |
| With women you do not know well? |
| With healthcare professionals? |
| HOW DO YOU FEEL ABOUT THE APPEARANCE OF THE BREAST WITH CLOTHES ON WHEN: |
| Alone? |
| With your partner? |
| With men in general? |
| With women you know? |
| With women you do not know well? |
| With healthcare professionals? |
| HOW DO YOU FEEL ABOUT THE APPEARANCE OF YOUR BREASTS IN A BIKINI WHEN: |
| Alone? |
| With your partner? |
| With men in general? |
| With women you know? |
| With women you do not know well? |
| With healthcare professionals? |
| HOW DO YOU FEEL ABOUT THE APPEARANCE OF YOUR NAKED BREASTS WHEN |
| Alone? |
| With your partner? |
| With men in general? |
| With women you know? |
| With women you do not know well? |
| With healthcare professionals? |
| WHAT IS YOUR LEVEL OF SATISFACTION, AND THAT OF OTHERS, WITH THE APPEARANCE OF YOUR BREASTS? |
| You |
| Partner |
| Mother or father (most important opinion to you) |
| Brother or sister |
| Friend |
| IS SIZE IMPORTANT TO YOU OR OTHER PEOPLE? |
| You |
| Partner |
| Mother or father |
| Brother or sister |
| Friend |

| BREAST-Q |
|---|
| With your breasts in mind, in the past week, how often have you felt: |
| 1 - None of the time |
| 2 - A little of the time |
| 3 - Some of the time |
| 4 - Most of the time |
| 5 - All of the time |
| a) Con?dent in a social setting? |
| b) Emotionally capable of doing the things you want to do? |
| c) Emotionally healthy? |
| d) Of equal worth to other women? |
| e) Self-assured? |
| f) Feminine in your clothes? |
| g) Accepting your body? |
| h) Normal? |
| i) Like other women? |
| j) Attractive? |
| Thinking of your sexuality, since your breast reduction, how often do you generally feel: |
| a) Sexually attractive in your clothes? |
| b) Comfortable/at ease during sexual activity? |
| c) Con?dent sexually? |
| d) Satis?ed with your sex life? |
| e) Con?dent sexually about your breast area appearance when undressed? |
| f) Sexy when undressed? |
| With your breasts in mind, in the past week, how satis?ed or dissatis?ed have you been with: |
| 1 - Very dissatis?ed |
| 2 - Somewhat dissatis?ed |
| 3 - Somewhat satis?ed |
| 4 - Very satis?ed |
| a) How you look in the mirror? |
| b) How comfortably does your bras ?t? |
| c) Being able to use more ?tted clothes? |
| d) How do you look in the mirror undressed? |
| During the past week, how satis?ed or dissatis?ed have you been with: |
| a) Your appearance in the mirror while dressed? |
| b) The shape of your reconstructed breast when wearing a bra? |
| c) How normal you feel in your clothes? |
| d) The size of your reconstructed breasts? |
| e) Your ability to wear more ?tted clothing? |
| f) How well your breasts are aligned with each other? |
| g) How comfortably your bra ?ts? |
| h) The softness of your reconstructed breast? |
| i) How similar in size your breasts are to each other? |
| j) How natural your reconstructed breast looks? |
| k) How naturally your reconstructed breasts sit/position themselves? |
| l) How your reconstructed breasts feel when touched? |
| m) How much your reconstructed breast feels like a natural part of your body? |
| n) How similar your breasts are to each other? |
| o) Your appearance in the mirror while undressed? |
| If you have implants in both breasts, answer thinking about the breast you are least satis?ed with. During the past week, how satis?ed or dissatis?ed have you been with: |
| a) The amount of rippling or wrinkling in your implant that you can see? |
| b) The amount of rippling or wrinkling in your implant that you can feel? |
| During the past week, how often have you experienced: |
| 1 - None of the time |
| 2- Some of the time |
| 3 - All of the time |
| a) Chest muscle pain? |
| b) Dif?culty lifting or moving your arms? |
| c) Dif?culty sleeping because of discomfort in the breast area? |
| d) Regions of hardness in the breast area? |
| e) Tightness in the breast area? |
| f) Dscomfort in the breast area? |
| g) Tenderness in the breast area? |
| h) Sharp pain in the breast area? |
| i) Aching pain in the breast area? |
| j) Tingling in the breast area? |
| k) Swelling in the arm (lymphedema) on the side where you had your mastectomy? |
| During the past week, thinking about your abdomen, how often have you experienced: |
| 1 - None of the time |
| 2 - A little of the time |
| 3 - Some of the time |
| 4 - Most of the time |
| 5 - All of the time |
| a) Dif?culty sitting up because of abdominal muscle weakness (e.g., getting out of bed)? |
| b) Difficulty performing daily activities because of abdominal weakness (e.g., making the bed)? |
| c) Abdominal discomfort? |
| d) Abdominal swelling? |
| Nipple reconstruction: How satisfied or dissatisfied are you with: |
| a) How natural your reconstructed nipples and areolae look? |
| Latissimus dorsi: During the past week, thinking about your back, how often have you been bothered by: |
| 1 - None of the time |
| 2 - A little of the time |
| 3 - Some of the time |
| 4 - Most of the time |
| 5 - All of the time |
| a) The location of the scar on your back? |
| b) The length of the scar on your back? |
| c) How visible the scar on your back is to others? |
| d) Your back not looking symmetrical? |
| e) The appearance of your back? |
| f) The shape of your back? |
| g) The appearance of the scar on your back? |
| h) Having to wear certain clothes to hide your back scars? |
| Latissimus dorsi: During the past week, thinking about your shoulder and back, how often have you experienced: |
| a) Shoulder stiffness? |
| b) Shoulder pain? |
| c) Back pain? |
| d) Difficulty performing activities with your arms above your head? |
| e) Difficulty performing activities with your arms extended? |
| f) Arm weakness? |
| g) Difficulty performing activities that repeatedly use your shoulder and back muscles? |
| h) Stiffness when extending your arm? |
| i) A pulling or twinging sensation in your back? |
| j) Difficulty reaching for objects? |
| k) Difficulty carrying heavy objects? |
| If you have received radiation in both breasts, answer thinking about the breast you are least satisfied with. During the past week, how concerned have you been about: |
| 1 - Not at all |
| 2 - A little |
| 3 - Very much |
| a) The skin of your breast looking different (e.g., much lighter or darker)? |
| b) Marks on the skin of your breast caused by radiation therapy (e.g., small blood vessels)? |
| c) The skin of your breast feeling dry due to radiation therapy? |
| d) The skin of your breast being sore or sensitive to touch due to radiation (e.g., with temperature changes or bathing)? |
| e) The skin of your breast feeling thick, rough, or dry when touched? |
| f) Skin irritation from clothing due to radiation therapy? |
| How satisfied or dissatisfied were you with the information you have received from your plastic surgeon about: |
| 1 - Very dissatisfied |
| 2 - Somewhat dissatisfied |
| 3 - Somewhat satisfied |
| 4 - Very satisfied |
| a) How reconstructive surgery was to be done? |
| b) Healing and recovery time? |
| c) Possible complications? |
| d) The options you were given regarding the timing of your breast reconstruction (i.e., at the same time as the mastectomy or later)? |
| e) The options were given regarding the type of surgery? |
| f) The pros and cons of the timing of your breast reconstruction? |
| g) How long would the breast reconstruction process take from start to finish? |
| h) What size you could expect your breasts to have after surgery? |
| i) How much pain could you expect during recovery? |
| j) What could you expect your breasts to look like after surgery? |
| k) How long after reconstructive surgery would it take for you to feel normal again? |
| l) How the surgery could affect future breast cancer screening (e.g., ultrasound, mammogram, self-examinations)? |
| m) The lack of sensitivity in your reconstructed breasts and nipples? |
| n) The experience of other women with their breast reconstruction surgeries? |
| o) What the scars would look like? |
| These questions are about your plastic surgeon. Did you feel that he/she: |
| 1 - Definitely disagree |
| 2 - Somewhat disagree |
| 3 - Somewhat agree |
| 4 - Definitely agree |
| a) Was competent? |
| b) Gave you confidence? |
| c) Involved you in the decision-making process? |
| d) Was reassuring? |
| e) Answered all your questions? |
| f) Made you feel comfortable? |
| g) Was thorough? |
| h) Was easy to talk to? |
| i) Understood what you wanted? |
| j) Was sensitive? |
| k) Listened to your concerns? |
| l) Was available when you had concerns? |
| These questions are about members of the medical team other than the surgeon (e.g. nurses and other doctors who looked after you on the day you had your surgery). Did you feel that they: |
| a) Were professional? |
| b) Treated you with respect? |
| c) Were knowledgeable? |
| d) Were friendly and kind? |
| e) Made you feel comfortable? |
| f) Were thorough? |
| g) Listened to your concerns? |
| These questions are about members of the office staff (e.g. secretaries, office or clinic nurses). Did you feel that they: |
| a) Were professional? |
| b) Treated you with respect? |
| c) Were knowledgeable? |
| d) Were friendly and kind? |
| e) Made you feel comfortable? |
| f) Were thorough? |
| g) Listened to your concerns? |

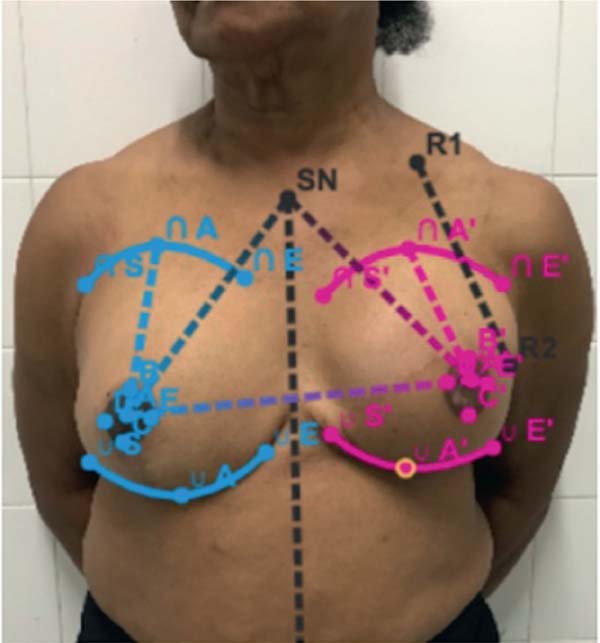
| Parameter | Mean |
|---|---|
| Difference in distance between the sternal notch and the nipple between the breasts:
[(SN-A) - (SN-A’)], if SN-A > SN-A’ or [(SN-A’) - (SN-A)], if SN-A’ > SN-A |
7.8 mm |
| Difference between the level of the right and left nipple | 6.6 mm |
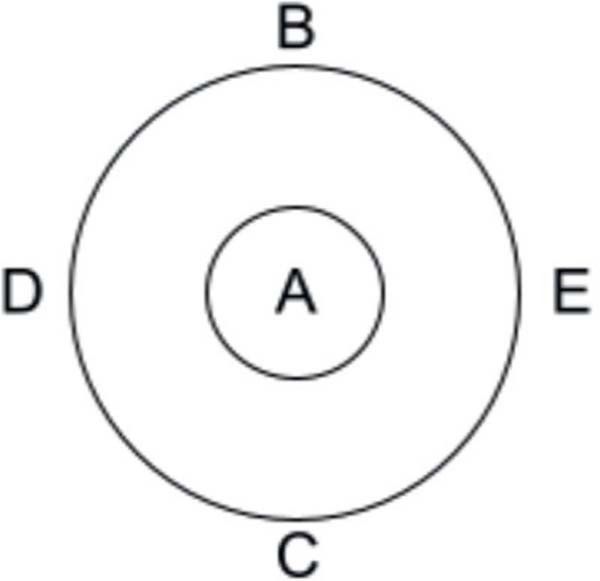
| Difference in distance from points B to C between the breasts: [(B-C) - (B’-C’)], if B-C > B’-C’ or [(B’-C’) - (B-C)], if B’-C’ > B-C |
2.5 mm |
| Difference in distance from points D to E between the breasts: [(D-E) - (D’-E’)], if D-E > D’-E’ or [(D’-E’) - (D-E)], if D’-E’ > D-E |
3 mm |
Abbreviations: A, apex of the upper pole of the right breast; A’, apex of the upper pole of the left breast; SN, sternal notch; SN-A, distance between the sternal notch and the right nipple; SN-A’, distance between the sternal notch and the left nipple.

Results
The mean age of the patients was of approximately 59 years. The sample adopted as representative for discussion in this study had a higher mean age, of 71 years. The group undergoing reconstruction with type-I Liacyr pedicle includ-ed 8 patients with a mean age of 59.62 years, 5 of whom underwent initial reconstruction with a latissimus dorsi flap, and 3, with a tissue expander. In the sample involving type-III pedicles, the patients had a mean age of 59.29 years, and 3 out of the 5 patients underwent reconstruction with a latissimus dorsi flap, while the remaining 2 received tissue expanders.
In the BREAST-Q assessment, the median simplified breast satisfaction score was of 71 (range: 0-100). In the group with type-III pedicles, the median score was of 82 (range: 0-100), with a total score ranging from 15 to 16, indicating excellent satisfaction. The median score of the complete breast satisfaction questionnaire was of 67, with minimal differences between the groups.
The median score regarding psychosocial well-being was of 87 (range: 0-100), with no significant differences between the groups. Sexual well-being showed the lowest median score: 62 (range: 0-100).
During the physical evaluation, the latissimus dorsi re-construction questionnaire was applied exclusively to patients who underwent this technique, as it considers variables and complications specific to this approach. The median score was of 83 (range: 0-100), with consistent satisfaction across most items, except for “appearance of the back scar” and “having to wear specific clothing to conceal back scars.”
The questionnaire assessing satisfaction with the infor-mation provided by the medical team yielded highly-positive results, with a median of 85 (range: 0-100) and a mode of 100 (range: 0-100). One of the items showing greater variability concerned guidance on “how surgery could affect future cancer screening (such as self-examination).”
Questionnaires evaluating satisfaction with the medical team (excluding the surgeon) and satisfaction with the surgeon demonstrated the highest median scores: 91 and 100 respectively. The mode for satisfaction with the surgeon was of 100 (range: 0-100), and the mean value was similarly high, with very few patients selecting responses equivalent to “somewhat satisfied” for any item about professional performance.
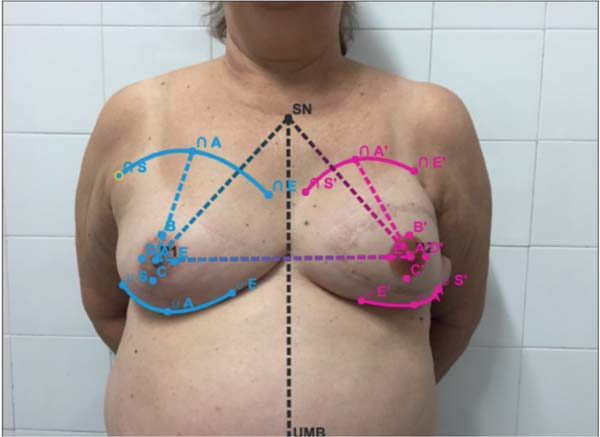
Table 7 presents the mean values regarding symmetry. The greatest difference occurred in the distances between the sternal notch and the nipples, with a mean of 7.8 (range: 2-9) mm. The difference between the levels of the left and right nipples also showed considerable variability, ranging from 2 to 8 (mean: 6.6) mm. In contrast, the difference in the distance between points B and C, as defined by the applica-tion, showed less variation, ranging from 2 to 3.5 (mean: 2.5) mm. Similarly, the difference in the distance between points D and E ranged from 2 to 5 (mean: 3) mm (►Fig. 2).
Discussion
Breast reconstruction is an essential component of patient care and a legally-guaranteed right. It is provided by the Brazilian Unified Health System (Sistema Único de Saúde, in Portuguese) and financed by insurance companies in Argentina. Breast cancer is the most common malignancy among women in many countries, affecting approximately one in seven women. Fortunately, survival after diagnosis has increased in recent years.
With advances in breast cancer treatment, more patients respond well to therapy and remain disease-free. Therefore, current discussions are no longer limited to curative approaches, but also include measures aimed at promoting a better quality of life for women.
The BREAST-Q is a valuable tool to assess the quality of life of patients undergoing breast reconstruction, addressing aspects such as satisfaction with breasts and psychosocial, sexual, and physical well-being. Recent studies, such as those by Sadok (2023) and Miseré (2021), have demonstrated that patients undergoing autologous reconstruction tend to re-port greater satisfaction with esthetic outcomes and quality of life compared with those who opt for alloplastic reconstruction.
The Liacyr flap used in the current study aligns with breast reconstruction goals, including achieving contralateral breast symmetry, ensuring patient safety, and maintaining quality of life. The different pedicle types enable better adaptation to each patient’s individual needs, with type-I being suitable for women with moderate breast volume (►Figs. 3-4) and type-III, for patients with low breast volume (►Figs. 5-6).










The use of Liacyr type-I and -III flaps in implant-based mammaplasty yields satisfactory esthetic outcomes and lower reoperation rates compared with reconstruction using implants alone. Furthermore, the two-step reconstruction process enhances breast symmetry, resulting in improved esthetic outcomes.
The analysis of reconstructed breast symmetry is funda-mental. It can use various parameters, such as size, position, projection, and ptosis (►Fig. 7). The surgical technique employed in the present study, combined with symmetry-assessment measures described in the literature, resulted in imperceptible asymmetries or only minor asymmetries in all evaluated patients.
In summary, autologous breast reconstruction using the Liacyr flap proved to be a safe and effective option, providing satisfactory esthetic results and improved quality of life. The use of validated questionnaires, such as the BREAST-Q, and careful analysis of breast symmetry are crucial tools to evaluate and optimize breast reconstruction outcomes.
Conclusion
Breast reconstruction using autologous tissue is highly-available and -reproducible, and it is associated with high patient satisfaction rates. As a result, the functional and esthetic outcomes of this reconstruction validate its status as a viable reconstructive option. It is important to note that the current study, which involved patients operated on by the same surgeons, has a relatively small sample size. Further research, especially matched clinical trials, is needed to determine the best outcomes for each group.
References
1. Nahabedian MY, Patel K. Autologous flap breast reconstruction: surgical algorithm and patient selection. J Surg Oncol 2016;113 (08):865-874. Doi: 10.1002/jso.24208
2. Homsy A, Rüegg E, Montandon D, Vlastos G, Modarressi A, Pittet B. Breast reconstruction: a century of controversies and progress. Ann Plast Surg 2018;80(04):457-463. Doi: 10.1097/SAP.0000000000001312
3. Colwell AS, Taylor EM. Recent Advances in Implant-Based Breast Reconstruction. Plast Reconstr Surg 2020;145(02):421-432. Doi: 10.1097/PRS.0000000000006510
4. Castro M, Pessoa M, Accorsi AJ Jr., Ribeiro L, Moreira LF. Mastopexy combined with augmentation: systematic use of Ribeiro’s inferi-orly-based flaps. Rev Bras Cir Plást 2013;28(03):333-342. Avail-able from: https://www.rbcp.org.br/Content/imagebank/pdf/en_v28n3a03.pdf
1. Surgery Division, Hospital Alcides Carneiro, Petrópolis, RJ, Brazil
Address for correspondence Ivan Demolinari de-Miranda, MD, Hospital Alcides Carneiro, Serviço de Cirurgia, Petrópolis, RJ, Brazil (e-mail: idemolinari@hotmail.com abgomesdealmeida@gmail.com).
Artigo submetido: 03/04/2024.
Artigo aceito: 14/12/2025.
Editor-in-chief: Dov Charles Goldenberg.
Conflict of Interests
The authors have no conflict of interests to declare.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket