



Original Article - Year 2026 - Volume 41Issue 1
Analysis of the Outcomes and Postoperative Complications of Patients Undergoing Body Contouring Plastic Surgery after Weight Loss
Análise dos resultados e das complicações pós-operatórias de pacientes submetidos à cirurgia plástica do contorno corporal após perda ponderal
Ana Carolina Vasconcellos Guedes Otsuka1,
ABSTRACT
Introduction Today, obesity is a global epidemic, leading to reduced life expectancy, increased mortality rates, and poorer quality of life. Patients experiencing weight loss may undergo body contouring surgeries to improve their mobility, personal hygiene, appearance, and psychological wellbeing. These procedures may have complications, suggesting an association between obesity and a higher incidence of postoperative complications.
Materials and Methods The present retrospective case review study analyzed medical records of patients undergoing reconstructive body contouring plastic surgery after bariatric surgery. The Plastic Surgery team at Hospital Estadual de Sapopemba performed these body contouring procedures from January to December 2022.
Results The sample consisted of 242 patients with a mean age of 44 years. Most patients were female (95.8%). The most frequently performed procedures were abdominal dermolipectomy (52%), mammaplasty (15%), and cruroplasty (14%). Seventy-five (30%) patients presented with complications, of which 94.6% were minor, and 5.3% were major. The main complications were seroma (33%), partial wound dehiscence (28%), and hematoma (9%).
Conclusion Complications are inevitable consequences of surgical procedures; however, appropriate management and knowledge of how to prevent and treat them in these patients are fundamental. Maintaining a good physician-patient relationship, frequent follow-up visits, and effective communication are essential during this period.
Keywords: obesity; plastic surgery; body contouring; bariatric surgery; postoperative complications
RESUMO
Resumo A obesidade é considerada, atualmente, uma epidemia global, sendo responsável pela redução da expectativa de vida, aumento da taxa de mortalidade e piora da qualidade de vida. Visando facilitar a mobilidade e a higiene pessoal, melhorar a aparência e o perfil psicológico, estes pacientes emagrecidos são submetidos a cirurgias do contorno corporal. Estes procedimentos podem ser acompanhados por complicações, sugerindo haver associação entre obesidade e aumento da incidência de complicações.
Materiais e Métodos Este estudo retrospectivo de revisão de casos, realizado por meio da análise dos prontuários dos pacientes submetidos a cirurgia plástica reparadora do contorno corporal após cirurgia bariátrica, pela equipe da cirurgia plástica do hospital estadual de Sapopemba, no período de janeiro a dezembro do ano de 2022. Resultados A amostra foi de 242 pacientes com idade média de 44 anos. O sexo predominante foi o feminino (95,8%). As cirurgias mais realizadas foram a dermolipectomia abdominal (52%), a mamoplastia (15%) e a cruroplastia (14%). As complicações estiveram presentes em 75 pacientes (30%), sendo 94,6% complicações menores e 5,3% complicações maiores. As principais complicações foram o seroma (33%), deiscência parcial da ferida (28%) e hematoma (9%).
Conclusão As complicações são consequências inevitáveis dos procedimentos cirúrgicos; no entanto, o manejo adequado e o conhecimento sobre como prevenir e tratar essas complicações nesses pacientes são fundamentais. Manter um bom relacionamento médico-paciente, consultas de acompanhamento frequentes e uma comunicação eficaz são essenciais durante esse período.
Palavras-chave: obesidade; cirurgia plástica; contorno corporal; cirurgia bariátrica; complicações pós-operatórias
Introduction
According to the Brazilian Association for the Study of Obesity and Metabolic Syndrome (Associação Brasileira para Estudo da Obesidade e Síndrome Metabólica, ABESO, in Portuguese), the World Health Organization states that obesity is one of the most severe health problems currently faced worldwide. By 2025, ABESO estimates that 2.3 billion adults around the world will be overweight, with approximately 700 million subjects classified as obese, that is, with a body mass index (BMI) over 30.1 In Brazil, the rate of this chronic condition increased by 72% over the past 13 years, rising from 11.8% in 2006 to 20.3% in 2019. The prevalence of obesity is similar among men and women; however, among women, obesity decreases with increasing educational level. Current data indicate an overall obesity prevalence of 19.8% in Brazil, affecting 18.7% of men and 20.7% of women.1,2
Obesity is currently considered a global epidemic and results in reduced life expectancy, increased mortality rates, poorer quality of life, and high public healthcare costs.3 The treatment of obesity may use clinical and surgical methods. Clinical treatment is effective for most obese patients; however, in cases of severe obesity, surgical treatment through bariatric surgery represents the most effective approach. Consequently, an increasing number of patients undergo this surgical procedure, which promotes fast and significant weight loss but leads to functional and esthetic bodily sequelae.4
After weight loss, excess skin folds may cause dermatitis, functional limitations, difficulties with personal hygiene, and impairment of sexual activity, reducing the quality of life for formerly obese patients. As a result, clinical evaluation by the plastic surgeon in collaboration with the patient is key. Patients who underwent weight loss may experience several conflicts and may have difficulty accepting their body image.5,6
Formerly obese patients may undergo body contouring surgeries to improve their mobility, personal hygiene, appearance, and psychological wellbeing. However, these procedures may have complications, suggesting an association between obesity and an increased incidence of postoperative complications.7 It is also necessary to provide proper counseling regarding the numerous and extensive scars resulting from multiple procedures, as this approach is fundamental to avoid unrealistic expectations concerning surgical outcomes.8,9
A surgical complication refers to any deviation that interferes with the expected recovery process. In general, patients’ overall health conditions, the magnitude of the procedure, or suboptimal surgical techniques influence such complications.10–12 Complications can be major or minor. Major complications require surgical reintervention or increased hospital stays. In contrast, management of minor complications may occur in outpatient settings using less complex procedures, such as aspiration, drainage, or dressings.13
Objective
The present study aims to analyze complications in post-bariatric body contouring surgery and to describe their postoperative management.
Materials and Methods
The current retrospective case review study analyzed medical records of patients undergoing reconstructive body contouring plastic surgery after bariatric surgery. The Plastic Surgery team at Hospital Estadual de Sapopemba (HESAP) performed these body contouring procedures from January to December 2022.
A surgical center census reported that the reconstructive plastic surgery team performed 292 surgical procedures in 2022. All patients underwent treatment of only one surgical area at a time, with intervals of at least six months, and no combined procedures. The surgical census excluded duplicate records, as some patients underwent more than one surgical intervention within a six-month interval and, as a result, could have had two surgeries in the same year. After these exclusions, the final sample consisted of 242 patients.
All surgeries were performed by the same professional team at HESAP. The local Research Ethics Committee approved this study under number CAAE 67111822.5.0000.008. The inclusion criteria were patients of both genders who had undergone bariatric surgery at least 2 years prior and experienced weight loss, as well as complaints of excess skin. These patients were referred to the Plastic Surgery outpatient clinic at HESAP in 2022. Weight stability for at least 6 months after achieving the target weight loss was required in all cases. All patients underwent clinical and laboratory evaluations confirming their suitability for the surgical procedure.
The exclusion criteria were patients with unstable weight loss, high surgical risk who were not cleared for surgery by the anesthesiology team, and patients who had not under-gone bariatric surgery. All participants signed informed consent forms and authorized the photographic documentation.
All patients received prophylactic antibiotic therapy with a first-generation cephalosporin (cefazolin). It is worth noting that all patients used compression stockings, intermittent lower-limb compression devices, and thermal blankets during the surgical procedure.
Data from the analysis of medical records were entered into a Microsoft Excel spreadsheet (Microsoft Corp.), version 2013. Demographic and sample characterization data were collected, including age, gender, weight, height, BMI, type of surgery performed, comorbidities, weight of the resected surgical specimen, surgical complications, and their management. Complications were classified as major or minor.
Major complications included those requiring additional surgical procedures (such as hematomas, significant suture dehiscence, and marginal skin necrosis) or rehospitalization (such as subjects with postoperative infections with systemic involvement). Minor complications included seromas, small suture dehiscence, hypertrophic scars, localized infections at the surgical wound site, and foreign-body granulomas in subcutaneous tissue.
All patients underwent preoperative and postoperative follow-up at the Plastic Surgery Outpatient Clinic of HESAP. The procedures performed included abdominal, crural, and brachial dermolipectomies, mammaplasty with no implant placement, torsoplasty, blepharoplasty, and scar revision.
Results
The sample consisted of 242 patients with a mean age of 44 years, ranging from 23 to 66 years. Most patients were female (95.8%).
► Table 1 shows the most frequently performed procedures, that is, abdominal dermolipectomy (52%), mamma-plasty (15%), and crural dermolipectomy (14%).
| Surgeries | N | % |
|---|---|---|
| Abdominal dermolipectomy | 127 | 52% |
| Mammaplasty | 36 | 15% |
| Crural dermolipectomy | 33 | 14% |
| Brachial dermolipectomy | 25 | 10% |
| Scar correction | 8 | 3% |
| Torsoplasty | 6 | 2% |
| Lateral chest wall dermolipectomy | 3 | 1% |
| Cyst resection | 2 | 1% |
| Blepharoplasty | 2 | 1% |
| Total | 242 |
Abbreviations: N, number of surgeries.

Seventy-five patients had complications, corresponding to 30% of cases, of which 94.6% were minor, and 5.3% were major. The main complications were seroma (33%), partial wound dehiscence (28%), and hematoma (9%), as presented in ►Table 2.
| Types of complications | N | % |
|---|---|---|
| Seroma | 25 | 33% |
| Partial dehiscence of the surgical wound | 21 | 28% |
| Hematoma | 7 | 9% |
| Hypertrophic scar | 5 | 7% |
| Necrosis | 4 | 5% |
| Surgical wound infection | 3 | 4% |
| Cyst | 2 | 3% |
| Pulmonary thromboembolism | 2 | 3% |
| Mondor’s disease | 2 | 3% |
| Venous thromboembolism | 1 | 1% |
| Keloid scar | 1 | 1% |
| Acute pulmonary edema | 1 | 1% |
| Pyoderma gangrenosum | 1 | 1% |
| Total | 75 |
Abbreviations: number of complicantions.

The comorbidities observed among the patients in this study included systemic arterial hypertension (SAH), type 2 diabetes mellitus (DM), depression, anxiety, and hypothyroidism.
The association between complications and BMI values revealed that 58% of the complication cases occurred in patients with a BMI ≥ 30.
Discussion
The increased performance of bariatric surgeries and the higher rates of body contour deformities, known as dysmorphias, have led to a growing demand for plastic surgery among post-bariatric patients to restore physical and emotional balance.7,14
Our demographic data is consistent with the literature, including the study by Cintra Junior et al.,7 with a predomi-nance of female patients (95.8%), a mean age of 44 years, and abdominoplasty and mammaplasty as the most frequently performed procedures.
In the management of patients with massive weight loss, it is essential to understand the clinical particularities and the increased risk of complications in this population compared with non-formerly obese patients.15,16 Postbariatric patients differ from non-bariatric patients in several aspects, including the rate of weight reduction, nutritional status, and complication rates.17
Agha-Mohammadi and Hurwitz18 reported that patients undergoing bariatric surgery have nutritional deficiencies, with greater deficits in micro and macronutrients due to malabsorption, especially in subjects with a history of gastric bypass. These deficiencies negatively affect wound healing, as these patients have increased nutritional requirements. Earlier studies have also reported that changes in digestive physiology may lead to chronic anemia resulting from a reduced absorption of iron, nutrients, and vitamins, leading to impaired wound healing and immune dysfunction.19
In the present study, the overall complication rate was 30%, which is consistent with data reported in the literature. The minor and major complication rates in our study were 94.6% and 5.3%, respectively. A meta-analysis and systematic review by Marouf and Mortada20 reported an overall complication rate of 31.5% across all included studies, consistent with our findings. This same meta-analysis identified seroma as the most frequent complication, followed by wound dehiscence. These findings are consistent with our study, in which seroma and wound dehiscence accounted for 33% and 28% of complications, respectively.
The next sections discuss some complications observed in our study, their management, and strategies for risk mitigation.
Seroma
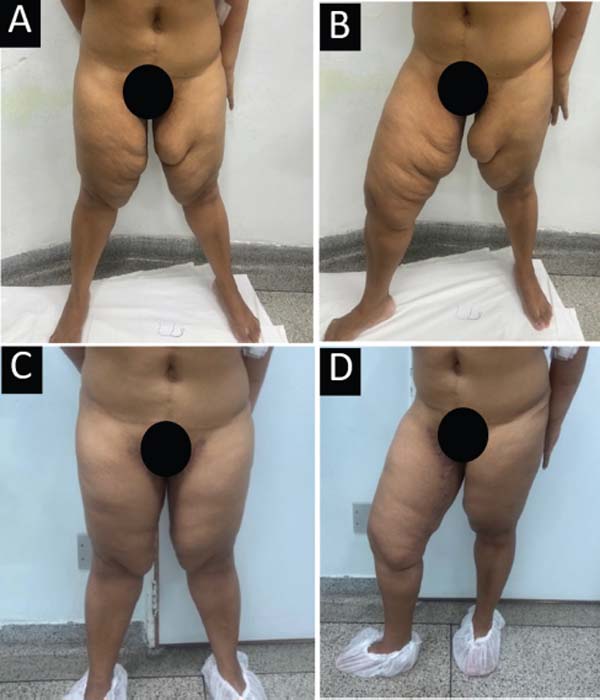
Seroma formation is one of the most common complications after body contouring procedures, with reported rates averaging around 15%.21 However, the seroma rate in our study was 33%. André22 reported that patients who underwent gastroplasty, when compared with non-bariatric patients, present a significantly higher incidence of seroma formation, particularly in the abdominal and thigh regions, to the point that it is virtually routine. This author also emphasized that the thickness of the adipose panniculus was a relevant factor in patients with recurrent seromas and large drainage volumes, as they had undergone hygienic surgical procedures. This finding is consistent with our results, as we identified a higher incidence of seroma in patients with greater adipose panniculus thickness (►Figs. 1–2).




We routinely place closed-suction drains in all major body contouring procedures and maintain them until daily fluid output is below 60 mL/day. If drainage remains above this threshold, the drain is kept in place, but for a maximum period of 2 weeks. Continuous compression garments are routinely prescribed. In cases of seroma formation, serial aspiration is combined with compression therapy. Patients requiring aspiration are evaluated weekly to monitor fluid reduction and to assess the potential risk of infection.
Surgical wound dehiscence
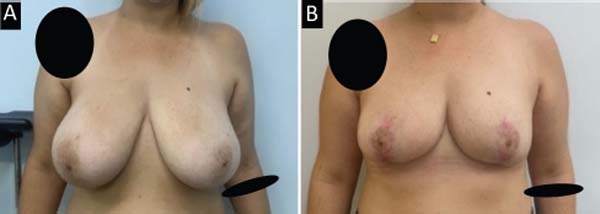
Wound dehiscence is one of the most common complications observed in post-bariatric body contouring procedures.16 Our study revealed a high incidence of wound dehiscence in cruroplasty scars, particularly at the junction of incisions in the inguinal region and the medial thigh. Albuquerque et al.23 described the triangular flap technique for medial thighplasty, in which a modification of the traditional “T-shaped” medial thighplasty involves preserving a triangular skin flap measuring approximately 4.5 × 4.0 cm, with a superior base, fixed to the deep planes, interrupting the horizontal incision near the inguinal fold. This flap is positioned greatest tension area to reduce the likelihood of wound dehiscence, consistent with our surgical experience. ►Fig. 3 illustrates a case of dehiscence following the use of the traditional “T” cruroplasty technique, which required a subsequent surgical revision to improve the scar appearance. The reoperation applied the triangular flap technique, resulting in reduced tension along the scar. The use of this technique resulted in a final scar with good aesthetic appearance and proper positioning (►Fig. 4).



Pyoderma Gangrenosum
Pyoderma gangrenosum is a rare, chronic autoimmune dermatosis first described by Brunsting and O’Leary in 1930, who emphasized its non-infectious nature. Histopath-ologically, it consists of a non-specific dermal neutrophilic infiltrate that is non-infectious, non-neoplastic, and does not present primary vasculitis.24
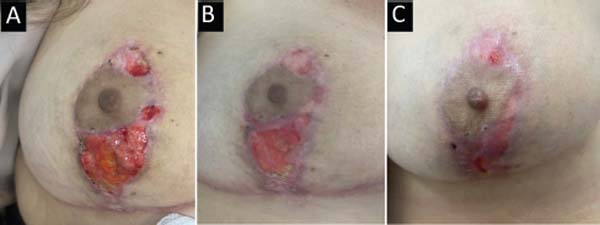
Our study had a single case of pyoderma gangrenosum following mammaplasty. The patient was a 39-year-old woman with a history of rheumatoid arthritis and no other comorbidities. On the twentieth postoperative day, she developed necrotic ulcers along the vertical and periareolar scars of both breasts, with moderate drainage of serous secretion. Oral pharmacological treatment followed a protocol consistent with the one described by Oliveira et al.,25 consisting of prednisone at a dose of 60 mg/day for seven days, followed by 40 mg/day for another seven days, then 20 mg/day for seven days, then 10 mg/day for four days, and concluding with 10 mg/day on alternate days, with a total treatment duration of 28 days. Topical treatment included laser therapy and wound dressings with collagenase ointment combined with chloramphenicol (►Figs. 5–6).


Conclusion
Seventy-five patients (30%) had postoperative complications in the current study. Minor complications were the most frequent, accounting for 94.6% of cases.
Although complications are inevitable in surgical practice, appropriate management and thorough knowledge of preventive and therapeutic strategies are essential, particularly in this patient population. Early identification of complications and transparent communication with patients are fundamental to achieving favorable outcomes. Maintaining a strong physician-patient relationship, ensuring regular follow-up visits, and promoting effective communication are crucial throughout the postoperative period.
REFERENCES
1. Associação Brasileira para o Estudo da Obesidade e Síndrome Metabólica. Mapa da Obesidade; 2022. Available from: <https://abeso.org.br/obesidade-e-sindrome-metabolica/mapa-da-obesi-dade/>
2. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Análise em Saúde e Vigilância de Doenças Não Transmissíveis. Vigitel Brasil 2019: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico: estimativas sobre frequência e distribuição sociodemográfica de fatores de risco e proteção para doenças crônicas nas capitais dos 26 estados brasileiros e no Distrito Federal em 2019. Brasília: Ministério da Saúde; 2020. Available from: https://bvsms.saude.gov.br/bvs/publicacoes/vigitel_brasil_2019_vigilancia_fatores_risco.pdf
3. World Health Organization (WHO). Obesity [Internet]. Available from: http://www.who.int/topics/obesity/en/
4. Cintra W Junior. Análise da qualidade de vida de pacientes submetidos à abdominoplastia circunferencial após tratamento cirúrgico da obesidade mórbida [Master’s Dissertation]. São Paulo: Faculdade de Medicina da Universidade de São Paulo; 2006
5. Adami GF, Meneghelli A, Bressani A, Scopinaro N. Body image in obese patients before and after stable weight reduction following bariatric surgery. J Psychosom Res 1999;46(03):275–281. Doi: 10.1016/s0022-3999(98)00094-4
6. Loli MSA. Obesidade como sintoma. São Paulo: Vetor; 2000
7. Cintra W Junior, Modolin MLA, Colferai DR, Rocha RI, Gemperli R. Post-bariatric body contouring surgery: analysis of complications in 180 consecutive patients. Rev Col Bras Cir 2021;48:e20202638. Doi: 10.1590/0100-6991e-20202638. [Internet]
8. Gerk PdO. Cirurgia do contorno corporal após grandes perdas ponderais. Rev Soc Bras Cir Plást 2007;22(03):143–152
9. Beidas OE, Gusenoff JA. Common Complications and Management After Massive Weight Loss Patient Safety in Plastic Surgery. Clin Plast Surg 2019;46(01):115–122. Doi: 10.1016/j.cps.2018.08.013
10. Cintra W Jr, Faintuch J. Aesthetic rehabilitation after bariatric surgery. In: Capodaglio P, Liuzzi A, Fainutch J, editors. Disabling Obesity: From Determinants to Health Care Models. Princeton: Springer; 2013:249–267
11. Moossa AR, Mayer AD, Lavelle-Jones M. Complicações cirúrgicas. In: Sabiston DC, editor. Tratado de cirurgia. A base biológica da prática cirúrgica moderna. 14th ed. Rio de Janeiro: Guanabara Koogan; 1993:282–299
12. Buck DW II, Mustoe TA. An evidence-based approach to abdom-inoplasty. Plast Reconstr Surg 2010;126(06):2189–2195. Doi: 10.1097/PRS.0b013e3181f83115
13. Neaman KC, Hansen JE. Analysis of complications from abdomi-noplasty: a review of 206 cases at a university hospital. Ann Plast Surg 2007;58(03):292–298. Doi: 10.1097/01.sap.0000239806. 43438.54
14. Cintra W, Modolin M, Rocha RI, Gemperli R. Abdominoplastia circunferencial simples e composta: evolução técnica, experiência de 10 anos e análise das complicações. Rev Bras Cir Plást 2021; 36(01):21–27. Doi: 10.5935/2177-1235.2021RBCP0005
15. Fraccalvieri M, Datta G, Bogetti P, et al. Abdominoplasty after weight loss in morbidly obese patients: a 4-year clinical experience. Obes Surg 2007;17(10):1319–1324. Doi: 10.1007/s11695-007-9235-7
16. Michaels J V, Coon D, Rubin JP. Complications in postbariatric body contouring: postoperative management and treatment. Plast Reconstr Surg 2011;127(04):1693–1700. Doi: 10.1097/PRS.0b013e31820a649f
17. García Botero A, García Wenninger M, Fernández Loaiza D. Complications After Body Contouring Surgery in Postbariatric Patients. Ann Plast Surg 2017;79(03):293–297. Doi: 10.1097/SAP.0000000000001109
18. Agha-Mohammadi S, Hurwitz DJ. Nutritional deficiency of post-bariatric surgery body contouring patients: what every plastic surgeon should know. Plast Reconstr Surg 2008;122(02): 604–613. Doi: 10.1097/PRS.0b013e31817d6023
19. Grace DM. Metabolic complications following gastric restrictive procedures. In: Deitel M, editor. Surgery for the Morbidly Obese Patient. Philadelphia: Lea & Febiger; 1989:339–50
20. Marouf A, Mortada H. Complications of Body Contouring Surgery in Postbariatric Patients: A Systematic Review and Meta-Analysis. Aesthetic Plast Surg 2021;45(06):2810–2820. Doi: 10.1007/s00266-021-02315-2. Erratum in: Aesthetic Plast Surg. 2021 Dec 6; PMID: 34018015
21. Coon D, Gusenoff JA, Kannan N, El Khoudary SR, Naghshineh N, Rubin JP. Body mass and surgical complications in the postbari-atric reconstructive patient: analysis of 511 cases. Ann Surg 2009; 249(03):397–401. Doi: 10.1097/SLA.0b013e318196d0c6
22. André FS. Cirurgia plástica após grande perda ponderal. Rev Bras Cir Plást 2010;25(03):532–539
23. Montenegro L, Albuquerque M, Tardelli HC, et al. Técnica do retalho triangular para cruroplastia medial pós grandes perdas ponderais em mulheres. Rev Bras Cir Plást 2010;25(04):700–704. Doi: 10.1590/S1983-51752010000400024
24. Binus AM, Qureshi AA, Li VW, Winterfield LS. Pyoderma gangrenosum: a retrospective review of patient characteristics, comorbidities and therapy in 103 patients. Br J Dermatol 2011;165(06):1244–1250. Doi: 10.1111/j.1365-2133.2011.10565.x
25. Oliveira FFGd, Fernandes M, Giacoia AMN, et al. Pioderma gangrenoso: um desafio para o cirurgião plástico. Rev Bras Cir Plást 2018;33(03):414–418. Doi: 10.5935/2177-1235.2018RBCP0156
1. Plastic Surgery Department, Hospital Estadual de Sapopemba, São Paulo, SP, Brazil
Address for correspondence Ana Carolina Vasconcellos Guedes Otsuka, MD, Departamento de Cirurgia Plástica, Hospital Estatual de Sapopemba, Avenida da Aclimação 314, São Paulo, SP, CEP: 01531– 000, Brazil (e-mail: ac.otsuka@gmail.com).
Article received: October 13, 2025.
Article accepted: January 13, 2026.
Conflict of Interests
The author has no conflict of interests to declare.
Editor-in-Chief: Dov Charles Goldenberg.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket