



Original Article - Year 2012 - Volume 27 - Issue 1
Changes in nipple-areola complex sensitivity after mammaplasty using the cross flap technique
Estudo de alterações de sensibilidade do complexo areolopapilar após mamoplastias com a técnica de retalhos cruzados
ABSTRACT
BACKGROUND: Although several types of reduction mammaplasty have been described in the literature, there are few studies addressing the post-operative changes in nipple-areola complex (NAC) sensitivity. The present study analyzed the changes in NAC sensitivity after mammaplasties performed using the cross flap technique (Sperli's technique).
METHODS: A descriptive, analytical, and retrospective study was conducted including 14 women between 20 and 60 years of age who underwent reduction mammaplasty with the cross flap technique. The patients had grades I, II, and III breast ptosis without hypertrophy or with small to medium hypertrophies.
RESULTS: In a subjective sensitivity and nipple contraction analysis, 12 (85.7%) patients reported a total return of NAC sensitivity 6 months after surgery. One year after surgery, all patients reported the return of sensitivity and nipple contraction with various degrees of intensity.
CONCLUSIONS: The cross flap technique is a viable option for reduction mammaplasty as it provides good aesthetic and functional results and the restoration of sensitivity to the breast in 100% of the cases.
Keywords: Mammaplasty. Breast/surgery. Surgical flaps. Perception.
RESUMO
INTRODUÇÃO: Vários tipos de mamoplastia redutora têm sido descritos na literatura, porém há poucas referências ao retorno da sensibilidade do complexo areolopapilar (CAP) após a cirurgia. Nesse contexto, o presente estudo objetiva analisar as alterações de sensibilidade do CAP após mamoplastias com a técnica de retalhos cruzados (técnica de Sperli).
MÉTODO: Foi realizado um estudo descritivo, analítico e retrospectivo, incluindo 14 mulheres com idade entre 20 anos e 60 anos, submetidas a mamoplastia redutora com a técnica de retalhos cruzados. As pacientes apresentavam ptoses mamárias graus I, II e III, sem hipertrofia ou com pequenas a médias hipertrofias.
RESULTADOS: A análise subjetiva da sensibilidade e da contração mamilar demonstra que, 6 meses após a operação, 12 (85,7%) pacientes reportaram que houve retorno total da sensibilidade do CAP. Um ano após a operação, todas as pacientes relataram volta da sensibilidade e da contração mamilar, em graus variados de intensidade.
CONCLUSÕES: A mamoplastia com a técnica de retalhos cruzados é uma ótima opção no arsenal técnico do cirurgião plástico, uma vez que, além de resultado estético harmonioso, proporciona excelente resultado funcional, com restituição da mama, ao longo do tempo, como órgão erógeno na mulher em 100% dos casos.
Palavras-chave: Mamoplastia. Mama/cirurgia. Retalhos cirúrgicos. Percepção.
Reduction mammaplasty is performed to correct functional alterations and/or the unsightly appearance of voluminous breasts or those presenting with ptosis. The purpose of surgery is to reduce breast size while maintaining symmetry and preventing complications1. Some of the main complications of reduction mammaplasty are the reduction in nipple-areola complex (NAC) sensitivity, unsightly scars, and postoperative mastodynia2,3. One of the main difficulties associated with reduction mammaplasties for large breasts is the maintenance of the vascularization of the NAC.
Current surgical techniques result in scars that can be "L" shaped, inverted "T" shaped, vertical, and periareolar. Vascular pedicles can be upper, superomedial, superolateral, lower, central, a combination of these, or none of these during the NAC grafting procedure2,4.
The cross flap technique described by Sperli5-8 in 1972 is aimed at reestablishing the relationship between the content and continent of the breast, and providing harmony to the mammary cones. The complications associated with the cross flap technique are similar to those observed with other surgical techniques for breast reduction and ptosis correction.
In the present study, the changes in NAC sensitivity caused by mammaplasties performed using the cross flap technique are assessed.
METHODS
The present descriptive, analytical, and retrospective study was conducted at the Integrated Plastic Surgery Services of Hospital Ipiranga, in São Paulo, SP, Brazil.
A total of 14 women between 20 and 60 years of age who underwent reduction mammaplasty with the cross flap technique in 2010 were included in the study.
The patients had grades I, II, and III breast ptosis without hypertrophy or with small to medium hypertrophies.
NAC sensitivity assessment
Tactile sensitivity tests were performed 6 months and 1 year after reduction mammaplasty. In addition, self reported information on NAC sensitivity in response to a stimulus was also considered in the analysis
The subjective analysis of NAC sensitivity and contractility was followed by two tests. In the first test, protopathic tactile sensitivity was assessed by sliding gauze over the NAC, while specific sensitivity was examined in the second test, which was based on stimulation with insulin needles.
RESULTS
The results of the subjective analysis of sensitivity and nipple contraction in patients who underwent cross flap mammaplasty obtained 6 months and 1 year after surgery are shown in Tables 1 and 2.
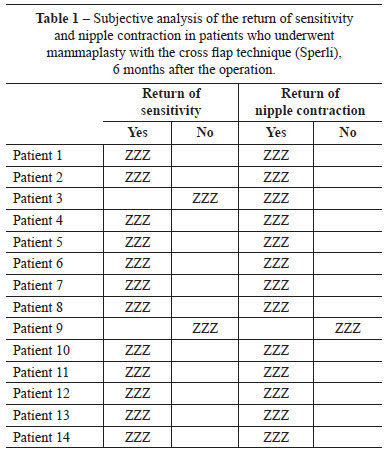
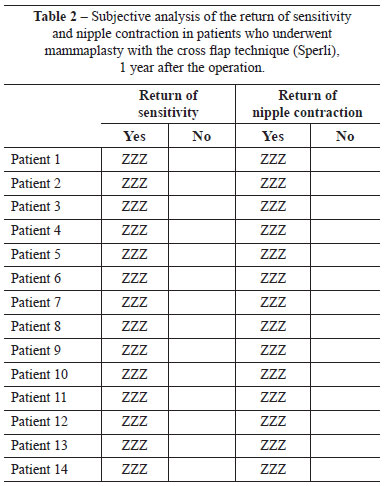
Six months after the surgery, 12 (85.7%) patients reported a complete recovery of NAC sensitivity. One year after surgery, all patients reported a recovery of nipple sensitivity and contractility, although with different degrees of intensity.
All patients reported a positive response to NAC stimulation with gauze 6 months and 1 year after surgery. The results of the assessment of specific sensitivity differed among patients, although the responses were similar on both sides: 8 (57.1%) patients reported the return of sensitivity first in the left NAC, and 6 (42.9%) in the right. With respect to breast quadrants, 9 (64.3%) patients felt the stimulus equally in the 4 quadrants, 3 (21.4%) reported reduced sensation in the left upper quadrant, which was present on the right side in 2 (14.3%) patients 6 months after surgery. All patients reported a recovery of specific sensitivity in the 4 quadrants 1 year after surgery.
DISCUSSION
Reduction mammaplasty is one of the most commonly performed procedures in plastic surgery2,3,7. In the selection of a surgical procedure, the safety of the method is an important consideration1.
There are several reduction mammaplasty techniques currently available that are mainly focused on the preservation of NAC vascularization. Certain techniques consider the two transverse pedicles, such as the technique described by Pitanguy et al.9, or the vertical pedicle, as in the technique of McKissoc. Techniques based on the lateral pedicle include the technique of Skoog, whereas techniques based on the lateral pedicle have been described by several authors. Notably, the decortication of the pedicle for the preservation of the subdermal plexus is important in all surgical mammaplasty techniques.
The NAC is innervated by sensory branches that originate from intercostal nerves. The areola is laterally innervated by the lateral cutaneous branches of the III, IV, V, and VI intercostal nerves10. The anterior lateral branch of the cutaneous branch of the IV intercostal nerve passes through the mammary tissue extending from the base of the breast directly to the NAC10. The erogenous sensitivity is provided by the sympathetic nerve fibers originating from the second to the sixth thoracic paravertebral ganglia that innervate the smooth muscle under the nipple11.
Schwartzman10 first reported the importance of the dermal vascular network for NAC nourishment. Since then, several authors have developed upper, lateral, and lower dermal pedicles for the NAC in reduction mammaplasties. A well nourished NAC is less likely to undergo necrosis and total loss of sensitivity.
NAC necrosis is described in the literature with a frequency of 85% to 90% in cases of gigantomastia, and grafting is often required for reconstruction1.
In protopathic sensitivity, which is the most primitive and diffuse type of sensory response, patients respond to painful cutaneous stimuli, heat, and cold, although the specific localization or type of stimulus cannot be determined with accuracy. It is the first type of sensitivity that appears after regeneration of a sectioned sensory-cutaneous nerve.
Specific sensitivity, which is associated with the accurate localization and discrimination of stimuli, appears later in cases of nerve regeneration and covers tactile and thermal sensitivities.
In the present study, the recovery of protopathic sensitivity was observed 6 months after reduction mammaplasty, while recovery of specific sensitivity was only partly observed at 6 months and was complete 1 year after surgery in all patients.
It is important to highlight that, in some patients, the return of sensitivity in the upper quadrants was not observed until 6 months after surgery.
CONCLUSIONS
Mammaplasty using the cross flap technique is a good treatment option for the plastic surgeon as it provides excellent aesthetic and functional results with complete recovery of NAC sensitivity.
REFERENCES
1. Pacheco LMS, Pacheco AT, Batista KT. Mamoplastia redutora com pedículo medial: modificação na técnica de Skoog. Rev Bras Cir Plást. 2011;24(3):321-7.
2. Bostwick J. Plastic and reconstructive breast surgery. St Louis: Quality Medical Publishing; 1990.
3. Arie G. Una nueva técnica de mastoplastia. Rev Latinoam Cir Plast. 1957;3:23-31.
4. Skoog T. Atlas de cirurgia plástica. Barcelona: Salvat; 1976. p. 332-80.
5. Sperli A E. Reduction mammaplasty under cross-flaps. In: I International Congress of the Aesthetic Surgery - 1972. Rio de Janeiro, Brasil.
6. Sperli AE. Mastoplastias redutoras pela técnica de retalhos cruzados. In: IV Congresso Argentino de Cirurgia Estética - 1975. Buenos Aires, Argentina.
7. Sperli AE. Mastoplastias estéticas en las ptosis: el limite entre el uso de las siliconas y las mastopexias. Rev Arg C Estética. 1977;2(2):93-8.
8. Sperli AE. Mammaplasty utilizing the crossed flap technique: a critical analysis of 23 years experience. Rev Soc Bras Cir Plást. 1994; 9(2):34-44.
9. Pitanguy I, Salgado F, Radwansky HN. Reduções mamárias: técnicas pessoais sem descolamento cutâneo. In: Mélega JM, ed. Cirurgia plástica: fundamentos e arte. Vol. III. Cirurgia estética. Rio de Janeiro: Médica e Científica; 2003. p. 477-84.
10. Schwartzman E. Die technik der mammaplastick. Chirurgie. 1930;2:932-43.
11. Strömbeck JO. Mammaplasty. In: Grabb W, Smith JW, eds. Plastic surgery. 5th ed. Washington: Library of Congress; 1997. p. 726-8.
1. Specialist in General Surgery, Specialist in Plastic Surgery of the Sociedade Brasileira de Cirurgia Plástica (Brazilian Society of Plastic Surgery) - SBCP, São Paulo, SP, Brazil.
2. Member of SBCP, Head of the Serviços Integrados de Cirurgia Plástica do Hospital Ipiranga (Integrated Plastic Surgery Services of Hospital Ipiranga), São Paulo, SP, Brazil.
3. Member of SBCP, Regent of the Serviços Integrados de Cirurgia Plástica do Hospital Ipiranga (Integrated Plastic Surgery Services of Hospital Ipiranga), São Paulo, SP, Brazil.
Thaís Helena A. Fernandes
Rua Cajaíba, 535 - Vila Pompeia
São Paulo, SP, Brazil - CEP 05025-000
E-mail: thais.antoniete@hotmail.com
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: November 28, 2011
Article accepted: February 2, 2012
Study conducted at the Serviços Integrados de Cirurgia Plástica do Hospital Ipiranga (Integrated Plastic Surgery Services of Hospital Ipiranga), São Paulo, SP, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket