



Original Article - Year 2012 - Volume 27 -
Pulp exchange: a simple solution for a complex problem
Troca pulpar: uma solução simples para um problema complexo
ABSTRACT
BACKGROUND: The fingertip is essential to the quality of the bi-digital pinch. Trauma to the fingertip is common and is difficult to resolve. In pulp exchange, a homodigital neurovascular island flap reconstructs the dominant pulp using pulp from the nondominant pulp, providing good skin coverage and sensitivity.
METHODS: From January 2000 to December 2008, 16 patients lost their dominant digital pulp. The surgical technique used for repair consisted of a homodigital neurovascular island flap, vascularized by the palmar digital artery of the nondominant pulp transposed to the dominant side. Flap viability, its sensitivity, and deficits in proximal and distal interphalangeal articulations were analyzed.
RESULTS: In the two-point discrimination test, an average of 8 mm was measured for all digits except the ring finger. In the Semmes-Weinstein monofilament test, D1 and D3 scored 3.61, while the other fingers scored 4.31. The same contralateral digits scored 2.83, except D5, which scored 3.61.
CONCLUSIONS: The technique of pulp exchange presented satisfactory functional results with regard to viability, sensitivity, and digital mobility, particularly with respect to the pinch. This local neurovascular flap also provides acceptable aesthetic results and is performed as a single surgical procedure.
Keywords: Reconstructive surgical procedures. Finger injuries/surgery. Surgical flaps. Sensation.
RESUMO
INTRODUÇÃO: A ponta do dedo tem papel importante na qualidade do movimento de pinça bidigital, e seu trauma é comum e difícil de resolver. Na troca pulpar, um retalho neurovascular homodigital em ilha reconstrói a polpa dominante, proporcionando boa cobertura de pele e sensibilidade, usando a polpa não-dominante.
MÉTODO: De janeiro de 2000 a dezembro de 2008, 16 pacientes perderam a polpa digital dominante. A técnica cirúrgica consistiu de um retalho neurovascular homodigital em ilha, vascularizado pela artéria digital palmar da polpa não-dominante transposto para o lado dominante. A viabilidade do retalho, sua sensibilidade e o déficit das articulações interfalangeanas proximal e distal foram analisados.
RESULTADOS: Houve média de 8 mm no teste de discriminação entre dois pontos estáticos para todos os dígitos, exceto no dedo anelar. No teste monofilamentar de Semmes-Weinstein, obteve-se escore de 3,61 para D1 e D3, e de 4,31 para os outros dedos. Comparado ao mesmo dígito contralateral, obteve-se escore de 2,83 para todos os dígitos, exceto para D5, que apresentou maior escore (3,61).
CONCLUSÕES: A técnica de troca pulpar apresentou resultados funcionais satisfatórios quanto a viabilidade, sensibilidade e mobilidade digital, priorizando o movimento da pinça. Esse retalho neurovascular local também proporciona resultados estéticos aceitáveis, em um único procedimento cirúrgico.
Palavras-chave: Procedimentos cirúrgicos reconstrutivos. Traumatismos dos dedos/cirurgia. Retalhos cirúrgicos. Sensação.
Trauma of the fingertips, followed by loss of substance, is commonly encountered in the daily practice of a hand surgeon. When this loss of substance occurs on the volar face of a fingertip, there are several reconstruction options. It is well known, however, that in this zone, the so-called digital pulp, good sensitivity, and fine perception are essential to preservation of one of the major movements of the hand, the pinch.
Uninnervated cutaneous grafts and flaps are considered poor alternatives because they do not ensure sensitivity and perception. Most practitioners in the field consider innervated flaps, such as those in homodigital "islands," to be the best option.
In this study, we present a technique of pulp exchange, where the flap is produced from the fingertip pulp on the side that is functionally less important, and is transferred to the defect, with highest priority given to maintaining opposition to the thumb.
This study aims to assess the results of digital pulp reconstruction by means of pulp exchange, a homodigital neurovascular island flap that uses the nondominant pulp as the donor area.
METHODS
We assessed 16 patients with traumatic lesions of the digital pulp who were treated by the Hand Surgery staff of Hospital São Lucas of Pontifícia Universidade Católica do Rio Grande do Sul (Porto Alegre, RS, Brazil), from January 2000 to December 2008. All procedures were performed by the same surgeon.
Patient age ranged from 22 to 25 (mean = 29); 10 were male (62.5%).
The extent of the pulp loss in all cases was determined immediately after appropriate debridement and was measured in square centimeters with the aid of a sterile ruler.
Patients were assessed with regard to fine sensitivity in the areas of the flap and of the total skin graft and, comparatively, in the contralateral finger. The two-point discrimination test (Weber test) and Semmes-Weinstein monofilament test were used to assess this sensitivity.
Finally, we also assessed the amount of leave time that patients took from work and their ability to return to work.
The average postoperative follow-up was 11 months.
Surgical technique
The surgical technique consisted of replacing the digital pulp on the more functionally important side of the fingertip by means of an island homodigital flap with neurovascular pedicle, based on the palmar digital artery (Figure 1).
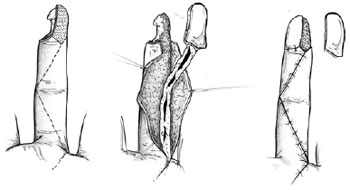
Figure 1 - Scheme of flap preparation.
An island flap gets its name from the fact that it is totally free in its cutaneous circumference except deeply at its neurovascular pedicle; this allows for great mobility.
When the digital pulp loss occurs in the 2nd, 3rd, 4th, or 5th fingers (Figure 2), the ulnar face of the fingertip is used to obtain the skin island (new digital pulp). In the thumb, the radial face is used for this purpose. This is justified by the greater importance of the radial faces of the 2nd, 3rd, 4th, and 5th fingers of the hand, which are in contact with the ulnar face of the thumb when the pinch is performed (Figure 3). Therefore, the skin used in the flap is from the less important, in functional terms, lateral face of the distal phalanx of the finger.

Figure 2 - Patient with significant loss of the dominant pulp of the index finger.

Figure 3 - Bi-digital pinch with the thumb, indicating the region to be reconstructed.
Several forms of flap design can be used, depending on the size of the digital pulp loss.
Initially, the flap is separated from the sheath of the flexor tendons, from the distal to proximal direction, in the central part of the finger. Next, the neurovascular pedicle is dissected to include the greatest quantity possible of fibroadipose tissue, in order to increase venous drainage. The collateral nerve and the palmar digital artery of the digit face are included. The flap is then laterally transposed and attached to the margins of the recipient area. The skin overlying the neurovascular pedicle (longitudinal incision) is sutured. The secondary defect in the donor area is covered with a total-thickness skin graft, removed from the hypothenar region (Figure 4).

Figure 4 - Flap of the pulp exchange, with skin grafting at the donor area.
RESULTS
Of the 16 patients who underwent pulp exchange, 12 (75%) had digital trauma in the dominant hand. Moreover, 14 (87.5%) of these patients relied on their hands for their professional activities.
With regard to the distribution of injuries, the most affected digit was the thumb in 5 (31.3%) patients; 4 (25%) patients had lesions in D2, 2 (12.5%) in D3, 2 (12.5%) in D4, and 3 (18.7%) in D5.
The thumb was the digit that had the greatest average extent of pulp loss (2.85 ± 0.85 cm2), followed by D2, D4, D5, and D3 (2.67 ± 0.26 cm2, 2.23 ± 0.12 cm2, 2.21 ± 0.23 cm2, and 2.18 ± 0.45 cm2, respectively).
The average result of the two-point discrimination test was 8 mm for all digits except D4, where the average was 10 mm. In the contralateral healthy digits, the average result was 6 mm, except in D2, where it was 8 mm. When the same test was performed on the areas of skin grafting, the average was 10 mm for D1 and D4 and 12 mm for D2, D3, and D5.
For D1 and D3, the area reconstructed by the flap received a score of 3.61 on the Semmes-Weinstein test; D2, D4, and D5 scored 4.31. The same digits on the contralateral side scored 2.83 on this test, with the exception of D5, which scored 3.61. When the same test was performed in the skin-grafted area, results ranged between 4.56 and 6.65, indicating the worst functional result as compared to the area of the neurovascularized flap.
The deficit of extension in the distal interphalangeal articulation was -15 degrees, always found in D5.
Partial or total necrosis did not occur in any of the surgical flaps.
The average time of sick leave was 45 days (range: 31-62 days). All patients returned to the same professional activities.
DISCUSSION
Digital pulp loss is a very common situation in hand trauma, as is demonstrated by the great number of surgical alternatives that are available for its reconstruction1-14. This type of trauma poses a surgical challenge with respect to the restitution of cutaneous coverage.
Skin grafts or uninnervated flaps give a poor surgical result in functional terms, with little restoration of local sensitivity. Good digital function requires not only good cutaneous coverage, but also the restoration of fingertip sensitivity. The quality of the fine sensitivity depends on the presence of a sufficient number of skin receptors. In the fingers, this population occurs only in the pulp, and decreases in the proximal direction. Therefore, several authors have reported their experiences with and without the use of local flaps for the aesthetic and functional treatment of this condition.
Only in cases of complete amputations of the digital pulp, where the use of local or distant flaps is impossible or inappropriate, is the free transference of the pulp of a toe used3,4,7,8.
The use of local advancement flaps is not always possible, when there is great tissue loss of the pulp obliquely. Palmar (thenar) flaps or cross-finger flaps proved to be insensitive, as are skin grafts. Moreover, according to Foucher et al.3, the dorsal digital skin, used in the cross-finger flap, is of inferior quality compared to the palmar skin for digital pulp reconstruction. This flap also requires the surgical violation of a healthy finger and its prolonged immobilization, which should be avoided whenever possible.
According to statistical data in the literature, the average result of the two-point discrimination test is 6 mm for innervated flaps and 9 mm for uninnervated flaps14. In the present study, the average result of this test, for all digits, was 8 mm, with the exception of D4, for which the average was 10 mm.
Several studies have already proven that, of the different techniques that exist for digital pulp reconstruction, neurovascular flaps constitute the best option, as they present the best functional results in the long term, allowing for appropriate sensitivity with good discrimination between two points and a low incidence of hyperesthesia. These two characteristics ensure one of the most important functions of the hand, perhaps the most essential, the pinch. Moreover, out of the several existing neurovascular flaps, it is possible to conclude that pulp exchange should be considered as the first option for reconstruction in cases of oblique traumatic lesions, in which the pulp is affected predominantly on the digital dominant face (radial in the fingers and ulnar in the thumb).
CONCLUSIONS
The technique of pulp exchange presented satisfactory functional results with regard to viability, sensitivity, and digital mobility, with the highest priority given to the pinch. This local neurovascular flap also provides acceptable aesthetic results and is performed as a single surgical procedure.
REFERENCES
1. Adani R, Busa R, Castagnetti C, Bathia A, Caroli A. Homodigital neurovascular island flaps with "direct flow" vascularization. Ann Plast Surg. 1997;38(1):36-40.
2. Borman H, Maral T, Tancer M. Fingertip reconstruction using two variations of direct-flow homodigital neurovascular island flaps. Ann Plast Surg. 2000;45(1):24-30.
3. Foucher G, Smith D, Pempinello C, Braun FM, Citron N. Homodigital neurovascular island flaps for digital pulp loss. J Hand Surg Br. 1989;14(2):204-8.
4. Joshi BB. A local dorsolateral island flap for restoration of sensation after avulsion injury of fingertip pulp. Plast Reconstr Surg. 1974;54(2):175-82.
5. Venkataswami R, Subramanian N. Oblique triangular flap: a new method of repair for oblique amputations of the fingertip and thumb. Plast Reconstr Surg. 1980;66(2):296-300.
6. Snow JW. The use of a volar flap for repair of fingertip amputations: a preliminary report. Plast Reconstr Surg. 1967;40(2):163-8.
7. Lanzetta M, Mastropasqua B, Chollet A, Brisebois N. Versatility of the homodigital triangular neurovascular island flap in fingertip reconstruction. J Hand Surg Br. 1995;20(6):824-9.
8. Henry M, Stutz C. Homodigital antegrade-flow neurovascular pedicle flaps for sensate reconstruction of fingertip amputation injuries. J Hand Surg. 2006;31(7):1220-5.
9. Kim KS, Yoo SI, Kim DY, Lee SY, Cho BH. Fingertip reconstruction using a volar flap on the transverse palmar branch of the digital artery. Ann Plast Surg. 2001;47(3):263-8.
10. Huang YC, Liu Y, Chen TH. Use of homodigital reverse island flaps for distal digital reconstruction. J Trauma. 2010;68(2):429-33.
11. Wilson AD, Stone C. Reverse digital artery island flap in the elderly. Injury. 2004;35(5):507-10.
12. Yildirim S, Avci G, Akan M, Aköz T. Complications of the reverse homodigital island flap in fingertip reconstruction. Ann Plast Surg. 2002;48(6):586-92.
13. Braga-Silva J, Jaeger M. Repositioning and flap placement in fingertip injuries. Ann Plast Surg. 2001;47(1):60-3.
14. Braga-Silva J, Gehlen D, Bervian F, Cunha GL, Padoin AV. Randomized prospective study comparing reverse and direct flow island flaps in digital pulp reconstruction of the fingers. Plast Reconstr Surg. 2009;124(6):2012-8.
1. Resident physician in the Plastic Surgery Department of Hospital São Lucas of Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS), Porto Alegre, RS, Brazil.
2. Full member of the Sociedade Brasileira de Cirurgia Plástica (Brazilian Society of Plastic Surgery) - SBCP, Head of the Plastic Surgery Department of Hospital São Lucas of PUCRS, Porto Alegre, RS, Brazil.
3. Full professor at Universidade Federal de São Paulo (Federal University of São Paulo) - Unifesp, São Paulo, SP, Brazil; full professor of Surgery at PUCRS, Porto Alegre, RS, Brazil.
Felipe Kunrath Simões Pires
Rua Padre Chagas, 370 - ap. 701 - Moinhos de Vento
Porto Alegre, RS, Brazil - CEP 90570-080
E-mail: fkspires@gmail.com
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: July 19, 2011
Article accepted: January 18, 2012
Study conducted at Hospital São Lucas of Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS), Porto Alegre, RS, Brazil.
Study presented at the 48th Brazilian Conference of Plastic Surgery, held in Goiânia, GO, Brazil, between November 11 and 15, 2011.
Prize-winning work, Victor Spina Award 2011.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket