



Original Article - Year 2012 - Volume 27 -
Subtotal glossectomy by modified keyhole lingual resection technique for the treatment of true macroglossia
Glossectomia subtotal pela técnica de ressecção lingual em orifício de fechadura modificada como tratamento de macroglossia verdadeira
ABSTRACT
We describe a case of true macroglossia in a 6-year-old child that was surgically treated with a midline elliptical excision and anterior wedge resection along a Gothic-shaped arch. The postoperative result was considered satisfactory with regard to both the volume of the tongue, which now remains entirely within the mouth, and the aesthetic appearance; the ability to taste has been maintained.
Keywords: Macroglossia/congenital. Macroglossia/surgery, Glossectomy. Tongue/surgery.
RESUMO
Neste artigo é apresentado o caso de macroglossia verdadeira em criança de 6 anos de idade, tratada cirurgicamente, com excisão elíptica na linha média da língua e ressecção ampla na ponta da língua em arco gótico. O resultado pós-operatório foi considerado satisfatório, tanto sob o aspecto de volume da língua, que passou a se manter totalmente dentro da boca, como sob o aspecto estético, mantendo a capacidade de gustação normal.
Palavras-chave: Macroglossia/congênito. Macroglossia/cirurgia, Glossectomia. Língua/cirurgia.
Macroglossia is an unusual pediatric condition with a variety of etiologies1,2. It is classified as true macroglossia when the tongue size is larger than normal, and as relative macroglossia when the oral cavity is not large enough to accommodate the tongue.
Macroglossia may be congenital or acquired2. The diagnosis is based on the presence of tongue protrusion with reference to the teeth, open lips, and maintenance of open-mouth posture3.
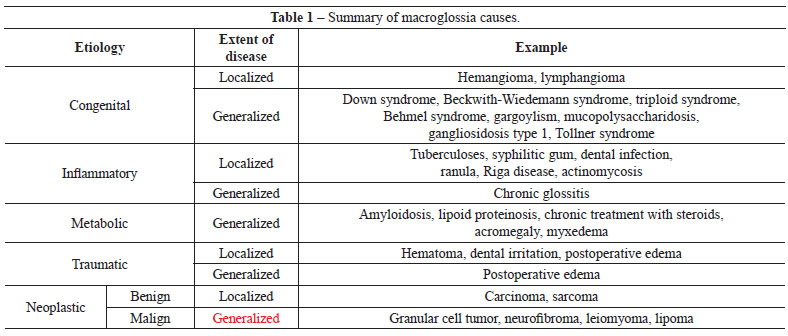
Myer et al.4 classified the etiologies of macroglossia - congenital, inflammatory, traumatic and neoplastic - as either generalized or localized (Table 1), according to the extent of the disease process5-24.
The tongue is involved in many functions, including swallowing, phonation, breathing, and normal development of the alveolar process and facial bone structure. Because of this, macroglossia may cause a number of problems, including difficulty in speaking, chewing, and swallowing as well as airway obstruction. In addition, tongue protrusion predisposes to tongue trauma, dry mouth, and repeated infections of the upper airways25.
The evaluation of macroglossia begins with a careful consideration of the patient's history and physical examination, with particular attention to changes in breathing, swallowing, phonation, and alteration of dental occlusion. Effort should also be made to try to identify any undiagnosed syndrome.
The therapeutic approach should include follow-up observations, treatment of any underlying systemic condition that may be causing tongue enlargement, orofacial therapy, and proper surgical intervention that preserves the vascularization and innervation of the tongue.
Surgical resection is considered the most appropriate treatment in the pediatric age group. Keyhole subtotal glossectomy is an optimal technique for these patients because it allows normal body development and prevents dentoalveolar complications. This technique was originally described by Morgan et al.26 and differs as to the reduction of muscle size in the 3 planes.
Surgical success should be evaluated by many factors, such as the disappearance of teeth marks on the edges of the tongue; proper positioning of the tongue within the oral cavity; improvement in or resolution of respiratory disorders; improvement in swallowing and phonation; preservation of taste, heat pain, epicritic and protopathic sensitivity; and improvement in tongue mobility.
Currently, priority is given to multidisciplinary treatment, including orthodontic, surgical, and phonoaudiological evaluation.
CASE REPORT
The patient, a 6-year-old girl, presented with a tongue with increased length and width. The tongue was resting and was interposed between the teeth, interfering with phonation and causing difficulty in chewing. Assessment of the skeletal profile showed absence of any alterations related to dentofacial deformities. A diagnosis of true macroglossia was made (Figure 1).
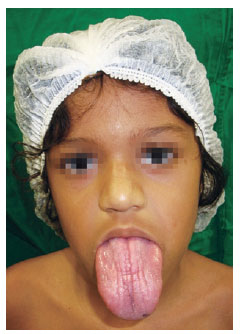
Figure 1 - Preoperative condition.
Glossoplasty was performed under general anesthesia, according to the technique of modified keyhole subtotal glossectomy with Gothic arch-shaped extensive resection of the tongue ends (Figures 2 and 3).
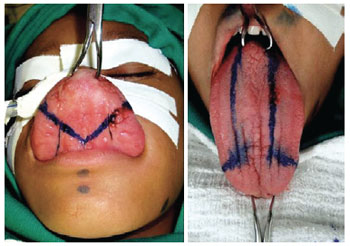
Figure 2 - Glossoplasty planning.
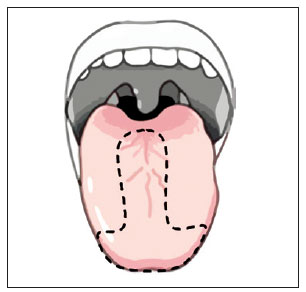
Figure 3 - Keyhole subtotal glossectomy, with gothic arch-shaped extensive resection of the tongue ends.
The incision was carried out using a surgical scalpel; the diaeresis was completed with electrocautery, for better hemostasis. In this manner, the excess tongue muscle tissue was removed (Figures 4 and 5). The tongue was closed using absorbable Vicryl sutures (Figure 6).
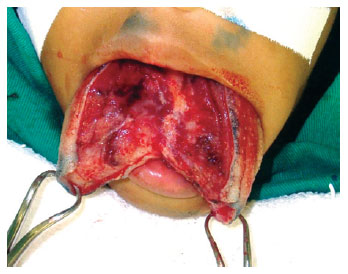
Figure 4 - Excess tongue tissue removal.
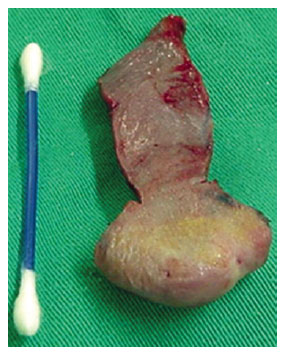
Figure 5 - Large rhomboid resection of the anterior third of the tongue.

Figure 6 - Approximation of planes and sutures.
DISCUSSION
Subtotal glossectomy is the appropriate surgical treatment in most cases in patients with airway obstruction, difficulty in speaking, dysphagia, and aesthetic damage.
Several surgical techniques are described for the correction of true macroglossia; these are subdivided into median line and peripheral glossectomies27.
In 1950, Edgerton28 described a technique consisting of excision along the center of the tongue with preservation of blood vessels, nerves, and taste buds, obtaining as result getting the strengthening of the tongue without changing the length (Figure 7). In 1965, Kole29 proposed a triangular incision at the end of the tongue, reducing the length and thickness of the anterior third of the tongue (Figure 8).
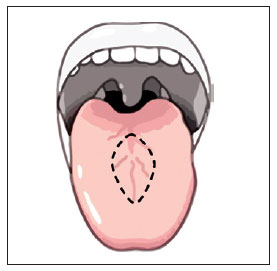
Figure 7 - Elliptical excision in the center of the tongue, as proposed by Edgerton28.
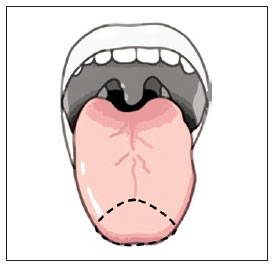
Figure 8 - Triangular incision at the end of the tongue, as proposed by Kole29.
The surgical technique presented in this article is a variant of keyhole glossectomy, originally described by Morgan et al.26, and involves a large excision of the distal end of the tongue, thus further reducing its length.
The realization of this technique has shown good results in the case shown (Figure 9), as in others described in the literature27-30.

Figure 9 - Anatomical presentation of the tongue at 9 months postoperatively.
In cases of macroglossia with idiopathic muscle hypertrophy, such as the reported in this paper, there is risk of relapse, thus, the surgical indication must be individualized, taking into consideration the risks and possible benefits for the patient31,32.
REFERENCES
1. Horn C, Thaker HM, Tampakopoulou DA, De Serres LM, Keller JL, Haddad J Jr. Tongue lesions in the pediatric population. Otolaryngol Head Neck Surg. 2001;124(2):164-9.
2. Vogel JE, Mulliken JB, Kaban LB. Macroglossia: a review of the condition and a new classification. Plast Reconstr Surg. 1986;78(6):715-23.
3. Dolan EA, Riski JE, Mason RM. Macroglossia: clinical considerations. Int J Orofacial Myology. 1989;15(2):4-7.
4. Myer CM 3rd, Hotaling AJ, Reilly JS. The diagnosis and treatment of macroglossia in children. Ear Nose Throat J. 1986;65(10):444-8.
5. Jian XC. Surgical excision of lymphangiomatous macroglossia: a case report. J Oral Maxillofac Surg. 1997;55(3):306-9.
6. Dios PD, Posse JL, Sanromán JF, Garcia EV. Treatment of macroglossia in a child with Beckwith-Wiedemann syndrome. J Oral Maxillofac Surg. 2000;58(9):1058-61.
7. Murphy JP. Comment on macroglossia and reduction glossectomy. Am J Orthod Dentofacial Orthop. 1997;111(4):29A-30A.
8. Moura CG, Moura TG, Durães AR, Souza SP. Exuberant macroglossia in a patient with primary systemic amyloidosis. Clin Exp Rheumatol. 2005;23(3):428.
9. Kempton JJ, Latto C. Neurofibromatosis presenting as macroglossia. Arch Dis Child. 1951;26(125):76-7.
10. Wittmann AL. Macroglossia in acromegaly and hypothyroidism. Virchows Arch A Pathol Anat Histol. 1977;373(4):353-60.
11. Bamelis M, Boyden B, Sente F, Madoe V. Sweet's syndrome and acute myelogenous leukemia in a patient who presented with a sudden massive swelling of the tongue. Dermatology. 1995;190(4):335-7.
12. García de Guilarte RF, Frönher BB, Urcelay PR, Nájera RC, Meli BG, Enríquez de Salamanca Celada J. An idiopathic case of macroglossia. J Plast Reconstr Aesthet Surg. 2009;62(2):e41-3.
13. Meares N, Braude S, Burgess K. Massive macroglossia as a presenting feature of hypothyroid-associated pericardial effusion. Chest. 1993;104(5):1632-3.
14. Linder N, Kuint J, German B, Lubin D, Loewenthal R. Hypertrophy of the tongue associated with inhaled corticosteroid therapy in premature infants. J Pediatr. 1995;127(4):651-3.
15. Ramesh V. Tuberculoma of the tongue presenting as macroglossia. Cutis. 1997;60(4):201-2.
16. Rizer FM, Schechter GL, Richardson MA. Macroglossia: etiologic considerations and management techniques. Int J Pediatr Otorhinolaryngol. 1985;8(3):225-36.
17. Loeffler JR, Duray PH, Sasaki CT. Macroglossal lymphangioendotheliomatosis. Report of a case in a pregnant woman. Arch Otolaryngol. 1984;110(9):600-3.
18. Donnelly LF, Jones BV, Strife JL. Imaging of pediatric tongue abnormalities. AJR Am J Roentgenol. 2000;175(2):489-93.
19. Gupta OP. Congenital macroglossia. Arch Otolaryngol. 1971;93(4):378-83.
20. Luna Ortiz K, Carmona Luna T, Herrera Gómez A, Cano Valdez AM. Macroglossia caused by adenoid cystic carcinoma. Case report. Med Oral Patol Oral Cir Bucal. 2008;13(6):E395-7.
21. Zúñiga S, Benveniste S, Egger E, Salgado C, Artigas R, Carter R, et al. Tumors of the tongue in children. Rev Chil Pediatr. 1982;53(4):338-44.
22. Abbott FC, Shattock SG. I. Neurofibromatosis of the nerves of the tongue (macroglossia neurofibromatosa) and of certain other nerves of the head and neck. Ann Surg. 1903;37(3):321-35.
23. Roles DM. Lipoma of the tongue. Br J Oral Maxillofac Surg. 1995;33(3):196-7.
24. Guelmann M, Katz J. Macroglossia combined with lymphangioma: a case report. J Clin Pediatr Dent. 2003;27(2):167-9.
25. Wolford LM, Cottrell DA. Diagnosis of macroglossia and indications for reduction glossectomy. Am J Orthod Dentofacial Orthop. 1996;110(2):170-7.
26. Morgan WE, Friedman EM, Duncan NO, Sulek M. Surgical management of macroglossia in children. Arch Otolaryngol Head Neck Surg. 1996;122(3):326-9.
27. Gasparini G, Saltarel A, Carboni A, Maggiulli F, Becelli R. Surgical management of macroglossia: discussion of 7 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94(5):566-71.
28. Edgerton M. The management of macroglossia when associated with prognathism. Br J Plast Surg. 1950;3(2):117-22.
29. Kole H. Results, experience, and problems in the operative treatment of anomalies with reverse over bite (mandibular protrusion). Int J Oral Surg. 1965;19:427-50.
30. Kaufman Y, Cole P, McKnight A, Hatef DA, Hollier L, Edmonds J. A modified keyhole technique for correction of macroglossia. Plast Reconstr Surg. 2008;122(6):1867-9.
31. Davalbhakta A, Lamberty BG. Technique for uniform reduction of macroglossia. Br J Plast Surg. 2000;53(4):294-7.
32. Malagola C, Barbato E, Fordellone P. Sindrome di Beckwith-Wiedemann: un caso raro. Dent Cadmos. 1990;58(1):74-8.
1. Plastic surgeon, Associate Professor at the Universidade Estadual do Ceará (State University of Ceará), Fortaleza, CE, Brazil.
2. Specialist member of the Sociedade Brasileira de Cirurgia Plástica (Brazilian Society of Plastic Surgery), Surgery Assistant at the Clínica de Cirurgia Crânio-Facial do Hospital Infantil Albert Sabin (Facial-Skull Clinic at Albert Sabin Children's Hospital), Fortaleza, CE, Brazil.
3. Medical student at the Universidade Estadual do Ceará (State University of Ceará), Fortaleza, CE, Brazil.
Moacir Cymrot
Rua Bonfim Sobrinho, 316 - ap. 901 - Fátima
Fortaleza, CE, Brazil - CEP 60040-500
E-mail: moacymrot@uol.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: February 22, 2010
Article accepted: June 4, 2011
Study conducted at the Universidade Estadual do Ceará (State University of Ceará), Fortaleza, CE, Brazil.
* In memoriam.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket