



Ideas and Innovation - Year 2012 - Volume 27 -
Closed circular suspension in the middle third of the face
Suspensão circular fechada do terço médio da face
ABSTRACT
The surgical treatment presented here involves technical innovations, making it a less-aggressive procedure. The goal is to demonstrate a different way of executing a suspension of the skin in the medial third of the face. The procedure is performed with semi-circular Stocchero needles with the passage of a 2-0 nylon thread through the subcutaneous plane at the anterior edge of the parotid gland and fixation to the temporal fascia. A total of 49 patients were operated on using this method with good aesthetic results. One patient required a preauricular incision to accommodate the skin. This method is safe, simple, does not require hospital inpatient admission, avoids a pre-auricular scar, and provides satisfactory results.
Keywords: Rejuvenation. Rhytidoplasty. Cosmetic techniques.
RESUMO
O tratamento cirúrgico apresentado neste artigo tem inovações táticas e torna o procedimento pouco agressivo. O objetivo é demonstrar uma maneira diferente de executar a suspensão do terço médio da face. O procedimento é realizado com agulhas semicirculares tipo Stocchero, com passagem de fio de náilon 2.0 no plano subcutâneo, na altura da borda anterior da glândula parótida, e fixação do fio na fáscia temporal. Foram operados com emprego desse método 49 pacientes, com obtenção de bons resultados estéticos. Em um paciente, houve necessidade de executar uma cicatriz pré-auricular, para acomodação da pele. O método é seguro, simples, não necessita de internação hospitalar, evita uma cicatriz pré-auricular e o resultado oferece boa satisfação aos pacientes.
Palavras-chave: Rejuvenescimento. Ritidoplastia. Técnicas cosméticas.
The growing concerns of patients with scars resulting from rhytidoplasty led to the search for non-stigmatizing methods, even if indications were restricted and the results were not excellent.
Roundblock is a treatment technique of the superficial muscular aponeurotic system (SMAS) developed by Stocchero1. A variant based on this technique was devised, in which the passage of the suspension thread through the SMAS lifts the medial third of the face without leaving scars. Other techniques described in the literature that involve suspensions of the face, leave pre- and/or retroauricular scars2,3.
Indications
The indications of the procedure are of great importance, because there are restrictions considering that this is a less-invasive method4. This surgery is indicated in patients aged between 35 and 45 years, with discrete skin flaccidity, mainly on the mandibular and submandibular regions5,6.
Pre-surgery photographs are taken by positioning the patient in front of a mirror and asking them to perform a digital traction of the skin towards the pinna so that an aesthetic improvement is observed in the submandibular and genian regions. This maneuver shows the redundant skin at the pre-auricular region (Figure 1). The photograph is taken in that position, representing the patient's desire and expectations of the results. In addition, the photograph is used as a protection against possible complaints7,8.

Figure 1 - Maneuver for preoperative photography. The patient shows how he/she wishes to appear; in that position, the skin redundancy at the pre-auricular region is indicated.
The patient's medical history is carefully recorded, and the procedure is precisely and thoroughly explained to the patients9. Patients are informed that the procedure does not require inpatient admission and that, in case of discomfort, it is possible to remove the suspension thread10.
METHODS
Anesthesia
The anesthetic solution is prepared with a bottle of lidocaine hydrochloride 2% (20 mL) with a vasoconstrictor diluted in 60 mL saline. In a 10-mL syringe with a Jelco no. 22 catheter, the solution is injected into the subcutaneous space between the previously marked lines (Figure 2).
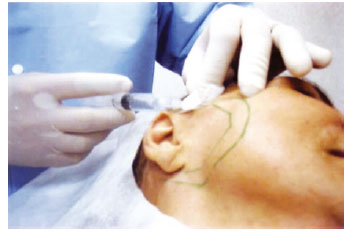
Figure 2 - Marking of the passage of the suspension thread and beginning of anesthetic infiltration.
Sedation must be performed in the presence of an anesthesiologist; however, this procedure may be performed without sedation in emotionally balanced patients who have a good relationship with the surgeon.
Technique
After anesthetic infiltration, a small incision is made on the scalp on the temporal region approximately 2 cm above the upper implantation line of the pinna. When the aponeurotic level is reached, the Stocchero curved needle is passed, following the 2 previously marked lines (Figure 3). This passage continues through the subcutaneous tissue and emerges on the skin approximately 2 or 3 cm below the ear lobe. Next, a 2-0 nylon thread, preferably transparent, is passed through the hole of the needle, and the needle is returned in the upper direction, exiting at the incision of the temporal region (Figure 4). The nylon thread may be passed around the pinna using Stocchero's curved needle or, in progressive maneuvers, using a Reverdin needle or a semi-circular needle (3/4 curved) with a false bottom, cutting edges, and 4 cm or more in length (Figure 5). When the passage around the pinna is completed, the 2 extremities of the nylon thread are at the upper incision. Thread traction is subsequently performed in order to assess the extent of skin suspension (Figure 6). After obtaining the ideal suspension, a triple knot is made with the nylon threads (Figure 7). The scalp is sutured with a 5-0 black nylon thread.

Figure 3 - Passage of the Stocchero needle through subcutaneous plane.

Figure 4 - Mounting of 2-0 transparent nylon thread onto the tip of the needle.
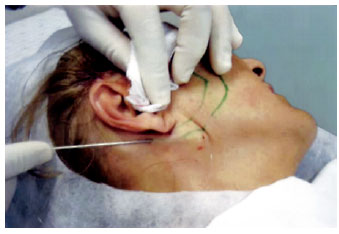
Figure 5 - Passage of the thread through the retroauricular region using a Reverdin needle or a false-bottom curved needle.

Figure 6 - Traction of the 2-0 thread showing suspension of the skin.

Figure 7 - Fixation of the passed thread to the temporal aponeurosis and tying of a triple knot.
DISCUSSION AND CONCLUSIONS
The technique described above is a less-aggressive procedure, easy to execute, and can be performed without hospital inpatient admission and without sedation in emotionally balanced patients.
The results are well accepted, and treatment can occasionally be repeated (Figures 8 and 9).

Figure 8 - In A, preoperative appearance, frontal view. In B, preoperative appearance, frontal view. In C, preoperative appearance, profile view. In D, postoperative appearance, showing accumulation of skin at the pre-auricular region, profile view. In E, postoperative appearance 1 month after the procedure, profile view. In F, postoperative appearance after 1 month, showing an absence of skin accumulation on the pre-auricular region, profile view.
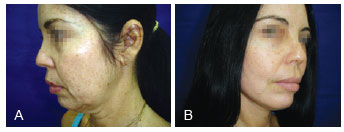
Figure 9 - In A, preoperative appearance. In B, postoperative appearance; the patient covers the volume of skin in the pre-auricular region with hair for 1 month.
Preoperative assessment must be thorough and very informative for the patient, considering the results are not as excellent as those with classical rhytidoplasty. The patient must be made aware that there will be an accumulation of skin in the pre-auricular region that must be hidden with hair. However, this accumulation practically disappears after approximately 1 month.
In conclusion, this procedure is effective when well indicated and well guided, and adds one more resource to the plastic surgeon's toolkit.
REFERENCES
1. Stocchero IN. The roundblock SMAS treatment. Plast Reconstr Surg. 2001;107(7):1921-3.
2. De Paola DQ, Varon EC. Mini-MACS lift: um minilift simplificado e de rápida recuperação. Rev Bras Cir Plást. 2011;26 Supl:30.
3. Stocchero I. Shortscar face-lift with the roundblock SMAS treatment: a younger face for all. Aesthetic Plast Surg. 2007;31(3):275-8.
4. Bafutto MG. Agulha para pontos internos de suspensão por fios. Rev Bras Cir Plást. 2008;23(4):310-2.
5. Baker TJ, Gordon H, Stuzin JM. Surgical rejuvenation of the aging face. 2nd ed. St. Louis: CV Mosby; 1996.
6. Converse JM. Personal communication, 1963, apud Johnson JB, Hartley R. The aging face. In: Converse JM, ed. Reconstructive Plastic Surgery. Philapelphia: WB Saunders; 1964. p. 1306-42.
7. Cardoso C. Ritidoplastia, arte e ciência. Rio de Janeiro: Di Livro; 2007.
8. Franco T, Rebello C. Cirurgia estética. Rio de Janeiro: Atheneu; 1977.
9. Farrapeira AB. Abordagem segmentar do terço médio da face. Triângulo da região geniana: ponto de sutura dermogorduroso. Rev Bras Cir Plást. 2009;24(4):497-503.
10. Souza AST, Andrade Júnior JCCG. Suspensão musculoaponeurótica com fixação periostal minimamente invasiva do terço médio da face: revisão de 50 casos. Rev Bras Cir Plást. 2011;26(3):439-45.
1. Head of the Plastic Surgery Department of the Hospital das Forças Armadas, plastic surgeon at private practice, President of the Distrito Federal Regional Office of the Sociedade Brasileira de Cirurgia Plástica/Brazilian Society of Plastic Surgery, Technical Director of the Instituto de Cirurgia Especializada (ICEL), Brasília, DF, Brazil.
Correspondence to:
Adilson Branco Farrapeira SHIS QI 26 - conj. 3 - casa 20 - Lago Sul
Brasília, DF, Brazil - CEP 71670-030
E-mail: abfarrapeira@ig.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: June 25, 2012
Article accepted: August 7, 2012
This study was performed at the Instituto de Cirurgia Especializada, Brasília, DF, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket