



Case Report - Year 2012 - Volume 27 -
Breakage of the tip of the cannula in the adipose tissue during liposuction
Quebra de ponta de cânula, no plano gorduroso, durante lipoaspiração
ABSTRACT
During liposuction, 3 cm of the distal segment of the cannula broke within the patient's adipose tissue. We used an image intensifier to easily and quickly address this complication without the development of any sequelae for the patient.
Keywords: Lipectomy/adverse effects. Equipment failure.
RESUMO
Durante procedimento de lipoaspiração, uma cânula teve seu segmento distal de 3 cm quebrado no plano adiposo. Os autores apresentam, neste trabalho, a conduta adotada para solução do caso, de maneira simples e rápida, com emprego de um intensificador de imagens, sem grandes dificuldades.
Palavras-chave: Lipectomia/efeitos adversos. Falha de equipamento.
Described in 1979, liposuction was an important breakthrough in plastic surgery and has become the most commonly performed surgical procedure of this specialty1.
Despite the high demand for liposuction and the popular acceptance of the procedure, its associated complications - which may be severe - have been targeted by the media.
It is worth noting that, even in the hands of an experienced plastic surgeon, this surgery presents risks. Some of these are rare, such as the breakage of the tip of the cannula within the adipose tissue that is described in this article. We report the solution that we adopted during the procedure to solve this complication; that is, the use of an image intensifier.
CASE REPORT
A 35-year-old female student (Caucasian) underwent wet liposuction of the flanks, thighs, and back under epidural anesthesia. She was maintained in the ventral decubitus position.
During liposuction of the back and upon cannula removal, the surgeon realized that its tip was missing. After ensuring that the broken tip had not fallen on the floor or on the surgical table, the possibility of breakage of the tip within the patient's adipose tissue was considered.
Palpation of the broken tip of the cannula in the adipose tissue was hampered by the fact that the surgery had already taken half the time originally predicted, in addition to the inconvenience caused by the infiltration of a solution containing epinephrine.
It was first decided to perform radiography, which indicated the tip in the adipose tissue. However, the two-dimensional image was not useful for assessing the precise location of the tip of the cannula, because it was impossible to evaluate the depth of the image.
Subsequently, the use of an image intensifier was considered (Figure 1). The device installed in the surgical unit is used by several specialties including urology, neurology, and, in particular, trauma surgery. This instrument provides live radiography, thus facilitating the monitoring of the procedure performed in the area examined, via a video screen and in real time. By using this equipment and with the aid of an Allis forceps inserted into the original liposuction incision, the tip of the cannula was "retrieved and removed from the adipose tissue (Figures 2 and 3).

Figure 1 - Image intensifier.
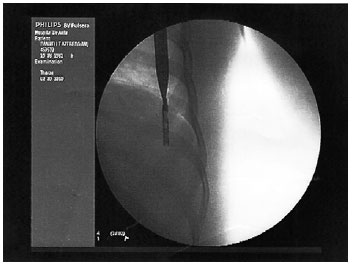
Figure 2 - A straight hemostatic forceps reaches the broken segment of the cannula.

Figure 3 - Profile view of the broken segment of the cannula against the ribs.
The surgery proceeded normally and according to the preoperative plan, without any further complications. The patient was discharged the following day and recovered completely after the surgery.
DISCUSSION
Cannulae for aspirating subcutaneous adipose tissue are available in several materials, diameters, and lengths, and with different types of tips and orifices. The instrument used in this procedure was a steel cannula, 25 cm long, with a diameter of 4 mm and 5 orifices of 1.5 mm × 2 mm each (Figures 4 and 5). Cannulae similar to that used in this study have been employed by the surgical team for more than 5 years without any inconvenience. This particular cannula had been used for only 3 months and had not shown any sign of deterioration.

Figure 4 - Steel cannula, 25 cm × 4 mm.

Figure 5 - Broken tip of the cannula, 3 cm in length.
The entire operation was performed within the norms required by the 1711/2003 Resolution of the Brazilian Federal Council of Medicine, which establishes safety criteria that should be observed during liposuction. These criteria ensure that the patient has the right to make an informed decision and the physicians are aware of the limits and indications for the procedure.
It is believed that it is not necessary to use cannulae with a diameter larger than 4 mm, as at least 1 study showed a similar rate of aspiration by using 4 or 5 mm cannulae. However, the possibility of complications is higher with larger-diameter cannulae2.
The cannula described in this study probably had defects, as narrow openings in the form of "slots", in the region of the lumen that, because they were in the interior of the cannula, were not detected by either the manufacturer's quality control evaluation or the medical team. This case demonstrates that, even with experienced surgeons using materials in perfect condition, unexpected situations might occur. Many professionals rely more on their personal experiences in troubleshooting than on scientific articles, often because of the lack of studies discussing these complications. No case reports similar to this study were found in the literature.
Liposuction is a safe procedure when performed by a well-trained surgeon with good medical and surgical judgment in a well-equipped operating room, depending on the extent of surgery required3. However, this does not imply that this procedure is free of complications, either major or minor, as in the case of any other operation4. This case demonstrates the necessity of performing surgical procedures in well-equipped hospitals to ensure the safety of the patient and the medical team. Without an image intensifier available during the operation, the "retrieval" of the broken tip of the cannula would have been quite difficult.
REFERENCES
1. Gomes RS. Critérios de segurança em lipoaspiração. Arq Catarin Med. 2003;32(4):35-46.
2. Viterbo F, Ochoa JS. Vibroliposuction: a study of rate of aspiration. Aesthetic Plast Surg. 2002;26(2):118-22.
3. Hughes CE 3rd. Reduction of lipoplasty risks and mortality: an ASAPS survey. Aesthet Surg J. 2001;21(2):120-7.
4. Karmo FR, Milan MF, Silbergleit A. Blood loss in major liposuction procedures: a comparison study using suction-assisted versus ultrasonically assisted lipoplasty. Plast Reconstr Surg. 2001;108(1):241-7.
1. Plastic surgeon, full member of the Sociedade Brasileira de Cirurgia Plástica/Brazilian Society of Plastic Surgery (SBCP), Director of the Clínica Multiplástica do Recife, Recife, PE, Brazil.
2. Plastic surgeon, full member of the SBCP, Master in Plastic Surgery, Recife, PE, Brazil.
3. Student at the Faculty of Medical Sciences of the Universidade de Pernambuco, Recife, PE, Brazil.
Correspondence to:
Moisés Wolfenson
Av. João de Barros, 791 - Boa Vista
Recife, PE, Brazil - CEP 50100-020
E-mail: moiseswolfenson@hotmail.com
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: December 22, 2010
Article accepted: August 14, 2011
This study was performed at the Clínica Multiplástica do Recife, Recife, PE, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket