



Original Article - Year 2012 - Volume 27 -
Use of dermal matrix and negative pressure dressings for the treatment of contractures in burn patients
Uso de matriz dérmica associado com o curativo por pressão negativa na abordagem da contratura em pacientes queimados
ABSTRACT
BACKGROUND: Burn patients are initially treated with volume replacement and, importantly, subsequent excision and early grafting of their injuries. These first aid measures improve the progress and survival rates of burned individuals. However, this treatment creates a new challenge in reparative surgery with regard to the management of burn sequelae, which mainly include contractures. In this study, we aimed to assess the effect of artificial dermal matrix application and negative pressure therapy on the treatment of burn sequelae.
METHODS: Ten patients with burn contractures were selected for this study and underwent scar contracture release, wound coverage with an artificial dermal matrix (Integra®), and negative pressure dressing according to the standard procedures. Dressing changes were performed every 5 days for 3-4 weeks. A skin graft was then laid on the wound bed. In the pre- and postoperative period, the patients were asked to rate their satisfaction with the aesthetic and functional aspects of the treated region.
RESULTS: In the areas in which the contractures were resected, integration of almost 98% of the dermal regeneration matrix was observed. Also integration was observed in 85% of the grafts used. All the patients reported a significant aesthetic and, in particular, functional improvement of the treated region.
CONCLUSIONS: The use of dermal regeneration matrix and negative pressure therapy for the treatment of scar contractures improves the success rate and the aesthetic and functional outcomes of patients with severe burn sequelae.
Keywords: Contracture. Burns. Reconstructive surgical procedures/methods.
RESUMO
INTRODUÇÃO: O aperfeiçoamento no tratamento inicial do paciente queimado, por meio da reposição volêmica e, principalmente, com excisão e enxertia precoce das lesões, resultou em profundo impacto na evolução dos indivíduos queimados, ocorrendo aumento da taxa de sobrevida. Com a maior sobrevida desses pacientes surgiu um novo desafio para a cirurgia reparadora, o tratamento das sequelas de queimaduras, principalmente compostas pelas contraturas. O objetivo deste estudo é demonstrar o uso da matriz dérmica artificial associado a terapia por pressão negativa no tratamento de sequelas de queimaduras.
MÉTODO: Foram selecionados 10 pacientes com contratura por queimadura. Os pacientes selecionados foram submetidos a liberação da contratura cicatricial e colocação de matriz dérmica artificial (Integra®), conforme técnica padrão, e curativo por pressão negativa para cobertura. A cada 5 dias, foram realizadas trocas do curativo até completar período de 3 semanas a 4 semanas. Após esse período, o leito foi submetido a enxertia de pele. Os pacientes foram questionados, no pré e pós-operatório, quanto a sua satisfação com os aspectos estético e funcional da região abordada.
RESULTADOS: Houve integração de cerca de 98% da matriz de regeneração dérmica na área em que a contratura foi ressecada. Também ocorreu integração de aproximadamente 85% dos enxertos utilizados. Todos os pacientes abordados referiram significativa melhora estética e, principalmente, funcional da região abordada.
CONCLUSÕES: O uso da matriz de regeneração dérmica associado a terapia por pressão negativa promove maior taxa de sucesso na abordagem da contratura cicatricial, proporcionando melhor resultado tanto funcional como estético nos pacientes com sequelas graves de queimadura.
Palavras-chave: Contratura. Queimaduras. Procedimentos cirúrgicos reconstrutivos/métodos.
Before the 1970s, patients with burns over more than one-third of their bodies often died due to burnshock or sepsis1. Burn patients are initially treated with volume replacement and, importantly, subsequent excision and early injury grafting. These first aid measures improved the progress and survival rates of burned individuals1,2.
The treatment of burn patients has improved, but it has also created a new challenge in reparative surgery with regard to the management of burn sequelae. Burn sequelae can be localized without causing extensive damage to the patient. However, contractures frequently result in the development of limiting and disfiguring scars in patients (Figure 1). Although several attempts have been made to prevent contracture formation, sequelae still occur in specific areas such as the neck, hands, wrists, and armpits3. Contractures can cause severe functional impairment, limit daily activities, and result in social isolation. Moreover, skeletal deformities may occur in children and lead to permanent and irreversible sequelae3,4.

Figure 1 - Child with a scar contracture in the cervical region caused by a prior burn that limited extension of the head.
To restore impaired function and prevent further deformities, contractures are treated by resection of the affected area and subsequent coverage of the region. Several approaches have been used to treat areas affected by scar contractures, such as primary closure; skin grafting; and Z-plasty-based local, distant, or microsurgical flaps. At present, skin grafts are commonly used after contracture resection5. However, patients with scar-induced contractures normally have extensive burns and scarce donor areas that might have already been used several times. Moreover, the small dermis of the graft placed in the recipient area influences the poor quality and resistance of the grafted region, which might result in the formation of new scar contractures3.
In this study, we aimed to assess the improvement of functional and aesthetic aspects of contracted regions induced by dermal regeneration matrix application and negative pressure therapy in the treatment of burn sequelae.
METHODS
This study was performed at the outpatient clinic of the Department of Plastic Surgery, Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (São Paulo, SP, Brazil).
Ten patients with post-burn scar contractures were selected for inclusion in this study. These patients underwent contracture resection until fibrotic regions were no longer observed. After resection and adequate hemostasis were achieved, a layer of dermal regeneration matrix (Integra®) was placed in the target area using a standard procedure. The matrix was fixed on the edge of the lesion with 5-0 monofilament nylon thread and a negative pressure dressing was applied (continuously and with a pressure of 125 mmHg) above the matrix. Negative pressure therapy was maintained for 2-3 weeks, whereas dressing changes were performed in a sterile environment every 5 days.
After 2-3 weeks, a thin skin graft made with the matrix was placed above the wound bed. This led to another negative pressure dressing (applied continuously and with a pressure of 125 mmHg) that was maintained for 5 more days. Once the dressing was removed, graft integration was assessed (Figures 2 and 3).

Figure 2 - In A, patient with scar contracture in the cervical region. In B, release of scar contracture and repositioning of the neck. Notice the widespread bloody area within the contracture region. In C, dermal regeneration matrix fixed to the bloody area in the cervical region. In D, negative pressure dressing placed above the dermal regeneration matrix. In E, appearance of the dermal regeneration matrix 3 weeks after the use of the negative pressure dressing. In F, appearance of the grafted area after removal of the negative pressure dressing. In G, 4 months postoperative aspect.
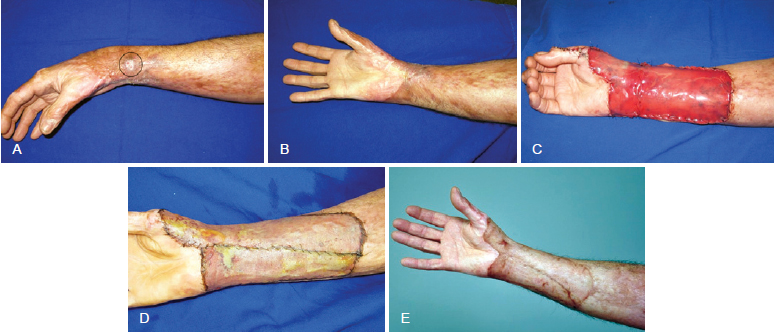
Figure 3 - In A, burn scar contracture in the upper limb. Notice the recurrent ulceration in the delimited area. In B, scar contracture in the upper limb hampering movement of the thumb. In C, defect in the upper limb after contracture resection. Notice the presence of the dermal regeneration matrix. In D, appearance of the grafted area after removal of the negative pressure dressing. In E, 12 months postoperative aspect.
In the pre-and postoperative periods, patients were asked to rate their satisfaction with the aesthetic as well as the functional aspects of the treated region.
RESULTS
In the areas in which the contractures were resected, integration of almost 98% of the dermal regeneration matrix was observed. Also integration was observed in 85% of the grafts used.
All the patients reported a significant aesthetic and, in particular, functional improvement of the treated region.
No further contractures or sequelae in the donor area were detected.
DISCUSSION
Resection followed by total or partial skin graft is the therapeutic approach that is more commonly used for the treatment of contractures. As a total skin graft involves the entire dermis, the advantages of this procedure include the following: less graft contraction, more resistant coverage of the receiving area, lower incidence of new contractures, and superior aesthetic outcomes. However, increased damage to the donor area as well as reduced graft integration has been observed3. A partial skin graft causes less damage to the donor area, thus increasing graft integration rate. However, small amounts of dermis increase graft contraction, grafted area sensitivity, and the incidence of new contractures in the treated regions. Moreover, the aesthetic outcome is worse than that obtained using total skin grafts3.
A small amount or even lack of dermis is observed in scar contracture areas in patients with burn sequelae, particularly those with major burns. Moreover, potential donor sites were previously used several times or affected by prior burns6. Ideally, grafts with the largest possible amount of dermis should be used for the treatment of scar contractures in these patients. However, as mentioned above, thin skin grafting is the more commonly used procedure.
The introduction of the dermal regeneration matrix enabled the option of providing a dermis to these patients, which is usually absent in the area to be treated. One dermal regeneration matrix, Integra®, consists of 2 layers. The upper layer, a silicone template, temporarily functions as an epidermis and prevents fluid loss and microbial invasion. The second layer is porous. Moreover, it is formed by cross-linked bovine collagen and chondroitin-6-sulfate, which constitute a template for dermal regeneration. Infiltrated fibroblasts migrate into this structure, which is quite similar to human tissue, and begin to synthesize the new dermis7,8.
Revascularization of this matrix begins after a minimum of 3 or 4 weeks, thus enabling the skin graft to be appropriately received7,8. Since this structure serves as a human dermis, a thin skin graft may then be used to treat burn patients. Thus, use of dermal matrix regeneration for the treatment of contractures combines the advantages afforded by the presence of the dermis in the contracture area with the beneficial effect of a thin skin graft when donor areas are scarce. Several studies in the literature have demonstrated that the use of a dermal regeneration matrix improves functional and aesthetic outcomes. In this study, we observed that the quality of the covered area significantly improved without the occurrence of complications in the donor area or the appearance of additional scar contractures.
The use of negative pressure therapy and its beneficial effects have been described in the literature for several years. It is known that when negative pressure is exerted on the wound bed, excess fluid is removed, area vascularization increases, bacterial concentration is inhibited, and granulation tissue is more rapidly formed9,10.
One of the advantages of using negative pressure therapy for the treatment of scar contractures is that patients do not require immobilization after surgery. This measure is usually taken out of fear of moving the matrix or the graft out the recipient wound bed; however, the negative pressure actually confers stability to the structures below the dressing. Thus, patients have high comfort levels after surgery, which improves the graft acceptance and matrix adhesion11.
Several studies report that the use of negative pressure therapy with dermal regeneration matrix application improved matrix vascularization and adhesion to the recipient bed. This effect reduces the interval required between matrix placement and skin graft surgery. Although no histological studies have demonstrated faster neovascularization, several authors report a reduction of 4-11 days in the interval required between matrix placement and skin grafting11.
In this study, we maintained a period of approximately 3 weeks between Integra® placement and skin grafting since a reduction of this period has not been proven to be effective with the use of negative pressure. However, negative pressure was used to confer a certain level of patient comfort, graft and matrix stability, and particularly, improve recipient wound bed and matrix quality. This procedure improved the integration rates of both the dermal regeneration matrix and the skin graft. The obtained values were similar to those found in the current literature11.
Thus, this new approach for the treatment of scar contracture presents several advantages over traditional procedures. However, a learning curve is required to obtain satisfactory results with dermal matrix regeneration and negative pressure therapy. Moreover, another disadvantage lies in the cost of this treatment, which is a limiting factor for many institutes. Aside from these disadvantages, this treatment for scar contractures should be included among the current procedures, based on the demonstrated satisfactory aesthetic and functional outcomes.
CONCLUSIONS
The use of dermal regeneration matrix and negative pressure therapy increase the scar contracture treatment success rate and improve the functional and aesthetic outcomes of patients with severe burn sequelae.
REFERENCES
1. Sheridan RL, Hinson MI, Liang MH, Nackel AF, Schoenfeld DA, Ryan CM, et al. Long-term outcome of children surviving massive burns.JAMA. 2000;283(1):69-73.
2. Donelan MB. Principles of burn reconstruction. In: Thorne C, ed. Grabb & Smith's plastic surgery. Philadelphia: Lippincott Williams & Wilkins; 2007. p.150-61.
3. Frame JD, Still J, Lakhel-LeCoadou A, Carstens MH, Lorenz C, Orlet H, et al. Use of dermal regeneration template in contracture release procedures: a multicenter evaluation. Plast Reconstr Surg. 2004;113(5):1330-8.
4. Alison WE Jr, Moore ML, Reilly DA, Phillips LG, McCauley RL, Robson MC. Reconstruction of foot burn contractures in children. J Burn Care Rehabil. 1993;14(1):34-8.
5. Dantzer E, Braye FM. Reconstructive surgery using an artificial dermis (Integra): results with 39 grafts. Br J Plast Surg. 2001;54(8):659-64.
6. Stiefel D, Schiestl C, Meuli M. Integra artificial skin for burn scar revision in adolescents and children. Burns. 2010;36(1):114-20.
7. Jeschke MG, Rose C, Angele P, Füchtmeier B, Nerlich MN, Bolder U. Development of new reconstructive techniques: use of Integra in combination with fibrin glue and negative-pressure therapy for reconstruction of acute and chronic wounds. Plast Reconstr Surg. 2004;113(2):525-30.
8. Dantzer E, Queruel P, Salinier L, Palmier B, Quinot JF. Dermal regeneration template for deep hand burns: clinical utility for both early grafting and reconstructive surgery. Br J Plast Surg. 2003;56(8):764-74.
9. Borgquist O, Ingemansson R, Malmsjö M. The influence of low and high pressure levels during negative-pressure wound therapy on wound contraction and fluid evacuation. Plast Reconstr Surg. 2011;127(2):551-9.
10. Orgill DP, Bayer LR. Update on negative-pressure wound therapy. Plast Reconstr Surg. 2011;127(Suppl 1):105S-15S.
11. Moiemen NS, Vlachou E, Staiano JJ, Thawy Y, Frame JD. Reconstructive surgery with Integra dermal regeneration template: histologic study, clinical evaluation, and current practice. Plast Reconstr Surg. 2006;117(7 Suppl):160S-74S.
1. Resident physician, Department of Plastic Surgery, Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (HCFMUSP), São Paulo, SP, Brazil.
2. Assistant physician, Department of Plastic Surgery, HCFMUSP, São Paulo, SP, Brazil.
3. Full professor, Department of Plastic Surgery, HCFMUSP, São Paulo, SP, Brazil.
Correspondence to:
Johnny Leandro Conduta Borda Aldunate
Rua Dr. Ovídio Pires de Campos, 171 - ap. 213 - Cerqueira César
São Paulo, SP, Brazil - CEP 05403-001
E-mail: johncond88@yahoo.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: March 3rd, 2012
Article accepted: August 7, 2012
This study was performed at Department of Plastic Surgery, Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, São Paulo, SP, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket