



Original Article - Year 2013 - Volume 28 -
Anatomical reconstruction of the umbilicus
Reconstrução anatômica da cicatriz umbilical
ABSTRACT
BACKGROUND: The absence of the umbilicus causes significant changes in the appearance of the abdomen, thus making it an essential part of anatomy. The reconstruction procedures should account of the anatomical position to ensure a natural appearance after treatment. The new umbilicus should have a good shape and appropriate position, but should not have an unaesthetic appearance, stenosis, or enlargement.
METHODS: This study included 162 patients who previously underwent open gastroplasty for the treatment of morbid obesity and 2 patients who underwent laparoscopic surgery. We used 2 parallel rectangular flaps measuring 2 × 1.5 cm that were sutured together and fixed to the aponeurosis of the rectus abdominis muscles. The flaps exhibited a curvilinear-shaped skin transition. The attachment flaps were created with 2 parallel points that reached the dermis on both sides of the flap and aponeurosis. Thus, the union of 2 flaps was obtained, which were slightly compressed at their distal portion. Thereafter, the fat tissue around the new umbilicus was approximated.
RESULTS: The technique described produced all anatomical units including a base, groove, and impeller as well as adequate depth of the umbilical scar in all cases. There were no cases of umbilical stenosis, hypertrophic scars, or keloid scars in the new umbilici.
CONCLUSIONS: This technique for the reconstruction of the umbilicus takes into account the anatomical units and provides a very natural appearance, eventually resulting in a slight excess of skin in the upper portion, thus giving a graceful appearance.
Keywords: Umbilicus/surgery. Abdomen/surgery. Bariatric surgery. Surgery, plastic/methods.
RESUMO
INTRODUÇÃO: A ausência da cicatriz umbilical causa alteração importante na forma do abdome, tornando-se, desse modo, imprescindível na anatomia do mesmo. Sua reconstrução deve seguir seus aspectos anatômicos, conferindo aspecto natural ao final do tratamento. A nova cicatriz umbilical deve ter boa forma, bom posicionamento, não apresentar cicatriz estigmatizante, estenose ou alargamentos, e ter aspecto natural.
MÉTODO: Foram operados 162 pacientes submetidos previamente a gastroplastia aberta para tratamento de obesidade mórbida e 2 pacientes submetidos a cirurgia videolaparoscópica. Foram utilizados 2 retalhos retangulares paralelos, medindo 2 cm x 1,5 cm, que foram suturados entre si e fixados à aponeurose dos músculos reto abdominais. Os retalhos apresentavam a transição com a pele em forma curvilínea. A fixação dos retalhos foi realizada com 2 pontos paralelos, que atingiam a derme do retalho de um lado, a derme do retalho do lado oposto e a aponeurose. Desse modo, foi obtida a união dos 2 retalhos, comprimindo-se levemente a porção distal dos mesmos. Em seguida, foi realizada aproximação do tecido gorduroso ao redor da nova cicatriz umbilical.
RESULTADOS: Com a técnica apresentada, obteve-se a formação de todas as unidades anatômicas (mamelão, sulco e rodete), além de profundidade adequada em todas as cicatrizes umbilicais reconstruídas. Não foi observado nenhum caso de estenose umbilical, cicatriz hipertrófica ou queloide nas novas cicatrizes umbilicais.
CONCLUSÕES: A técnica apresentada para reconstrução da cicatriz umbilical, respeitando as unidades anatômicas, proporciona forma bem natural e, com o passar do tempo, ocorre uma sobra de pele em sua porção superior, conferindo graciosidade à mesma.
Palavras-chave: Umbigo/cirurgia.Abdome/cirurgia.Cirurgiabariátrica.Cirurgiaplástica/métodos.
In the last decade, bariatric surgery has become a routine procedure, and requires plastic surgery for the reconstruction of defects resulting from the resultant excess skin. The reconstruction of the umbilicus is a procedure that refines the outcomes of abdominal surgery.
Although the umbilicus is depressed and adheres to deep planes, it is the only scar in the human body that is acceptable to individuals. Its absence significantly affects the aesthetics of the abdomen, making it an essential part of the anatomy.
The aesthetic appeal of the abdomen is directly related to good umbilical conformation. Reconstruction of the umbilicus either after its loss or for aesthetic reasons must follow the anatomical features to provide a natural appearance after treatment. The new umbilicus should have a good shape and appropriate position; should not have an unaesthetic appearance, stenosis, or enlargement; and should have a natural appearance.
The umbilicus is a depressed scar surrounded by a natural fold of skin approximately 1.5 to 2.5 cm in diameter1,2. Its natural position is at the height of the line joining the highest point of the 2 anterior superior iliac crests; this point is located between the third and fourth lumbar discs3-5. The position in the vertical plane is known to vary, and in cases where it is located more anteriorly, the umbilicus provides a more graceful-looking abdomen 3. Regarding the sagittal plane, the umbilicus exhibits laterality up to 8% of the width of the abdomen in 98.3% of subjects 4. It is formed by a base, which corresponds to the corrugated part surrounded by a groove or ring. Its upper portion, which surrounds the depressed portion, is called the impeller. The umbilicus should be small, have a T-shaped depression, be round or oval, and have a slight fold of skin on its upper portion1,5.
This article reports a technique for the reconstruction of the umbilicus employed in the surgical treatment of 164 patients.
METHODS
Between March 2011 and September 2012, 164 patients who had previously undergone gastroplasty for the treatment of morbid obesity underwent reconstruction of the umbilicus. Of these patients, 162 had a median supraumbilical scar, which was the access for open gastroplasty. Two patients had no median scar since they had undergone laparoscopic surgery. Twenty-nine patients were men, and 135 were women.
All umbilical scars were eliminated along with the surgical specimen. To reconstruct the umbilicus either because of its absence or for aesthetic reasons, we used 2 parallel rectangular flaps as previously described by Franco et al.6; the flaps were sutured together and fixed to the aponeurosis of the rectus abdominis muscles. These flaps were 1.5 × 2.0 cm wide but somewhat larger flaps may be used in certain cases. The flaps exhibited a curvilinear-shaped skin transition rather than right angles. We also noted the curvilinear shape in the distal portion of the flap (Figure 1).

Figure 1 - Marking of the flaps, with a curvilinear-shaped skin transition (arrows).
The flaps were attached at 2 parallel points that reached the dermis of the flap on both sides and the aponeurosis in its median line. Thus, we obtained the union of 2 flaps, which were slightly compressed in the distal portion (Figures 2 to 4).
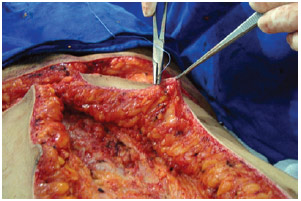
Figure 2 - Fixation of the flaps, with the stitch reaching the dermis of the flap.
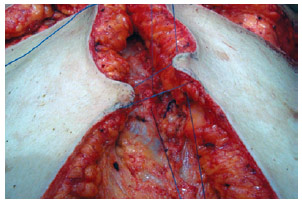
Figure 3 - Fixation of the flaps, with the stitch reaching the lateral flaps and aponeurosis.
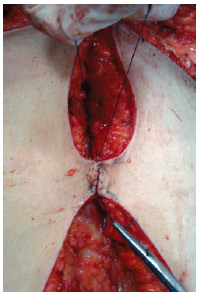
Figure 4 - Flaps fixed at the aponeurosis, forming the base and groove.
Next, the fat tissue around the umbilicus was approximated with new points using 1 Vicryl (polyglactin) and a 4-cm needle. The needle must be sufficiently large to include the maximum possible amount of fat tissue (Figure 5). Care must be taken when crossing points to avoid making the sutures too tight, which can cause liponecrosis. The procedure was completed with skin suturing (Figure 6).
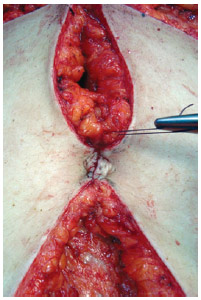
Figure 5 - Nearing the adipose tissue surrounding the new umbilicus.

Figure 6 - Immediate postoperative appearance.
RESULTS
A total of 164 patients underwent reconstruction of the umbilicus, while considering the anatomical units. The formation of all anatomical units was noted, including the base, groove, and impeller, and adequate depth was achieved in all reconstructed umbilical scars.
There were no cases of umbilical stenosis. Similarly, no hypertrophic or keloid scars were observed on the new umbilici, although pathological scarring occurred in the vertical scar above or below the umbilicus.
We observed ptosis in the supraumbilical skin, leading to a slight excess of skin in the upper portion of the new umbilicus in the postoperative period.
The reconstructed umbilical scars had good size and excellent shape, as is observed in Figures 7 to 11.
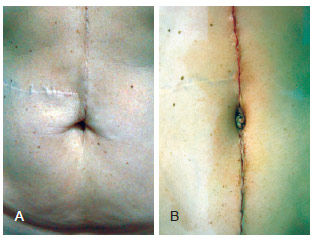
Figure 7 - In A, preoperative appearance. In B, immediate postoperative appearance.

Figure 8 - Late postoperative appearance.
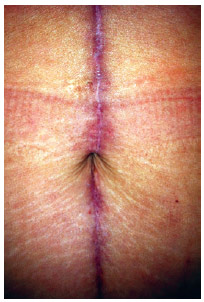
Figure 9 - Late postoperative appearance.
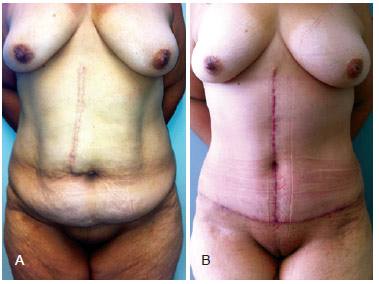
Figure 10 - In A, preoperative appearance. In B, postoperative appearance.
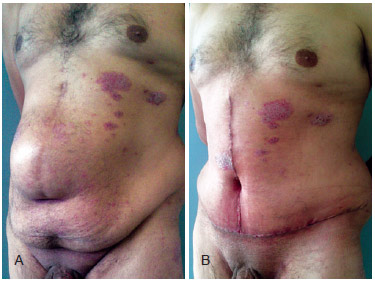
Figure 11 - In A, preoperative appearance. In B, postoperative appearance.
DISCUSSION
The reconstruction of the umbilicus remains challenging for plastic surgeons. Various techniques are described in the literature, including the use of local flaps4,5,7-14, skin grafts and cartilage5,15,16, and sutures alone17-19. Although these techniques provide some reasonably aesthetic results, they remain unable to yield a natural-looking new umbilicus. In order for the reconstruction to be as close to ideal as possible, the anatomical units of the element to be treated must be suitably reconstructed.
This paper presents a modification of the technique proposed by Franco et al.6 that involves rebuilding the anatomical units (i.e., base, groove, and impeller) in a stepwise manner. The base is formed at the aponeurosis by 2 fixing flaps, compressed at the distal edge. Because the dermal layer is included in the suture of the flap, the flaps fold, which gives the appearance of a groove. The proximity of the adjacent fat tissue to the new umbilicus raises the edges around it, thus providing the required depth. The sutures should not be too tight at those points in order to avoid necrosis of the adjacent tissue and liponecrosis. Because the flaps are short, there is a bend in the skin around the new umbilicus, which forms the impeller. Therefore, all anatomical structures are rebuilt, giving a natural final appearance. Some ptosis is expected to occur on the skin located in the upper portion of the umbilicus over time, forming a discreet fold that gives a more natural look to the final reconstruction. Using flap sizes of 1.5 to 2.0 cm ensures that a small and smooth umbilicus is obtained. Since there is a circular scar, neither stenosis nor "umbilical operation-associated stigma" occurs.
The technique of Silva & Oliveira20 can be used when performing a tuck in anchor reconstruction to determine the height of the umbilicus in the abdomen, in which a larger skin flap is left to further define a flap from 1.5 to 2.0 cm. The major difficulty of the reconstruction of the umbilicus is making the new umbilicus sufficiently deep, particularly when the patient presents a scarce adipose panniculus. By ensuring the adjacent fatty tissue is included, the present technique resolves this issue. Maintaining a curve in the base of the flap rather than a right angle to the approach avoids the formation of edges, thereby achieving a more rounded umbilicus and avoiding one that is elongated and closed.
CONCLUSIONS
The technique for reconstruction of the umbilicus presented here accounts for the anatomical units, provides a very natural look, and generates slight excess of skin on the upper part over time, giving a more graceful appearance. The resultant umbilicus exhibits appropriate features of depth and size. This technique avoids the appearance of scarring and secondary stenosis by hiding the circular scar incision and maintaining its position in the middle of the new navel.
REFERENCES
1. Craig SB, Faller MS, Puckett CL. In search of the ideal female umbilicus. Plast Recontr Surg. 2000;105(1):389-92.
2. Marconi F. Reconstruction of the umbilicus: a simple technique. Plast Recontr Surg. 1995;95(6):1115-7.
3. Coetzee T. Clinical anatomy ofthe umbilicus. S Afr Med J. 1980;57(12):463-6.
4. Rohrich RJ, Sorokin ES, Brown SA, Gibby DL. Is the umbilicus truly midline? Clinical and medicolegal implications. Plast Reconstr Surg. 2003;112(1):259-63.
5. Southwell-Keely JP, Berry MG. Umbilical reconstruction: a review of techniques. J Plast Reconstr Aesthet Surg. 2011;64(6):803-8.
6. Franco D, Medeiros J, Farias C, Franco T. Umbilical reconstruction for pacients with a midline scar. Aesthetic Plast Surg. 2006;30(5):595-8.
7. Arai K, Yamashita K, Suda T, Ikeda K, Yamauchi M, Yotsuyanagi T. Primary reconstruction of the umbilicus, using two rectangular subcutaneous pedicle flaps. J Plast Reconstr Aesthet Surg. 2012;65(1):132-4.
8. Baack BR, Anson G, Nachbar JM, White DJ. Umbilicoplasty: the construction of a new umbilicus and correction of umbilical stenosis without external scars. Plast Reconstr Surg. 1996;97(1):227-32.
9. Breuninger H. Navel reconstruction after umbilical melanoma excision. Eur J Plast Surg. 1997;20:325-7.
10. Iida N, Ohsumi N. Reconstruction of umbilical hypogenesis accompanied by a longitudinal scar. Plast Reconstr Surg. 2003;111(1):322-5.
11. Masuda R, TakedaA, Sugimoto T, Ishiguro M, Uchinuma E. Reconstruction of the umbilicus using a reverse fan-shaped flap. Aesthetic Plast Surg. 2003;27(5):349-53.
12. Ozbek S, Ozcan M. Umbilicus reconstruction with modified 'unfolded cylinder' technique. Br J Plast Surg. 2005;58(4):500-3.
13. Pfulg M, Van de Sijpe K, Blondeel P. A simple new technique for neo-umbilicoplasty. Br J Plast Surg. 2005;58(5):688-91.
14. Sawada Y. An umbilical reconstruction using subcutaneous pedicle flap. Eur J Plast Surg. 1995;18:185-7.
15. Abenavoli FM, Cusano V, Cucchiara V, D'Amico C, Corvelli L. An idea for umbilicus reconstruction. Ann Plast Surg. 2001;46(2):194.
16. SchoellerT, Rainer C, Wechselberger G, Piza-Katzer H. Immediate navel reconstruction after total excision: a simple three-suture technique. Surgery. 2002;131(1):105-7.
17. Bartsich SA, Schwartz MH. Purse-string method for immediate umbilical reconstruction. Plast Reconstr Surg. 2003;112(6):1652-5.
18. Park S, Hata Y, Ito O, Tokioka K, Kagawa K. Umbilical reconstruction after repair of omphalocele and gastroschisis. Plast Reconstr Surg. 1999;104(1):204-7.
19. SchoellerT, Rainer C, Wechselberger G, Piza-Katzer H. Immediate navel reconstruction after total excision: a simple three-suture technique. Surgery. 2002;131(1):105-7.
20. Silva FN, Oliveira EA. Neo-onfaloplastia na abdominoplastia vertical. Rev Bras Cir Plást. 2010;25(2):330-6.
Plastic surgeon, full member of the Sociedade Brasileira de Cirurgia Plástica/Brazilian Society of Plastic Surgery, chief resident of the Plastic Surgery Service of Hospital Felicio Rocho, Belo Horizonte, MG, Brazil
Correspondence to:
Alfredo Donnabella
Rua Timbiras, 3.642 - conj. 504 - Barro Preto
Belo Horizonte, MG, Brazil - CEP 30140-062
E-mail: adonnabella@uol.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: December 5, 2012
Article accepted: February 7, 2013
This study was performed at the Plastic Surgery Hospital Felicio Rocho, Belo Horizonte, MG, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket