



Original Article - Year 2013 - Volume 28 -
Nipple-areola reconstruction using the double opposing flap technique
Reconstrução do complexo areolopapilar com double opposing flap
ABSTRACT
BACKGROUND: Reconstruction of the nipple-areola complex (NAC) is the fundamental step in breast reconstruction in cases involving amputation of the nipple complex during mastectomy. The double opposing flap technique enables efficient reconstruction of the NAC, providing an adequate diameter, good projection, and symmetry with respect to the contralateral NAC. In addition, the donor area can be closed, and all scars can be contained within the topography of the reconstructed areola. This study presents the results obtained in NAC reconstruction using the double opposing flap technique in breast reconstruction.
METHODS: This retrospective study involved 24 patients in whom 31 NACs (17 unilateral and 7 bilateral) were reconstructed using the abovementioned technique between July 2008 and June 2010. The results were evaluated objectively and subjectively.
RESULTS: In the subjective analysis, the patients' satisfaction level regarding the final surgery results was high. In the objective analysis, the areolar horizontal diameter and nipple projection of the reconstructed NACs were quantitatively similar (P > 0.05).
CONCLUSIONS: The double opposing flap is an excellent strategy for NAC reconstruction. The method has a short learning curve and guarantees centralized symmetrical nipples with long-term results.
Keywords: Mammaplasty. Breast/surgery. Nipples/surgery. Breast neoplasms. Surgical flaps.
RESUMO
INTRODUÇÃO: A reconstrução do complexo areolopapilar (CAP) é etapa fundamental na reconstituição mamária nos casos em que há amputação desse complexo durante a mastectomia. Uma técnica muito eficiente é a do double opposing flap, que possibilita reconstruir o CAP, propiciando diâmetro adequado, boa projeção e simetria em relação ao CAP contralateral, com a possibilidade de fechar a área doadora e com todas as cicatrizes contidas na topografia da nova aréola reconstruída. O objetivo deste estudo é demonstrar os resultados obtidos nas reconstruções do CAP com o double opposing flap nas reconstituições mamárias.
MÉTODO: Estudo retrospectivo de 24 pacientes, nas quais foram reconstruídos 31 CAPs (17 unilaterais e 7 bilaterais) utilizando a técnica referida, entre julho de 2008 e junho de 2010. Os resultados foram avaliados objetiva e subjetivamente.
RESULTADOS: Na análise subjetiva, o grau de satisfação das pacientes foi elevado no que concerne ao resultado cirúrgico final. Na análise objetiva, o diâmetro horizontal areolar e a projeção mamilar dos CAPs reconstruídos demonstraram-se matematicamente semelhantes, com valores de P apresentando significância estatística (P > 0,05).
CONCLUSÕES: O double opposing flap é, na atualidade, uma excelente estratégia para reconstrução do CAP, com metodização que propicia curta curva de aprendizado, garantindo mamilos centralizados, simétricos e com resultados duradouros.
Palavras-chave: Mamoplastia. Mama/cirurgia. Mamilos/cirurgia. Neoplasias da mama. Retalhos cirúrgicos.
Reconstruction of the nipple-areola complex (NAC) is a fundamental step of breast reconstruction in cases in which the nipple complex is amputated during mastectomy. Various techniques for NAC reconstruction have been reported, but the results are controversial; some results are considered very good, whereas others are considered unsatisfactory.
In 1949, Adams1 pioneered the use of skin grafts from the labia minora as a donor area for NAC reconstruction. Other techniques that use the labia majora have also been described. However, the results have been disappointing because of inadequate coloration of the graft as well as the residual deformity of the donor area2-4. Brent & Bostwick5 used a graft from the retroauricular region in patients with fair skin; the results were good because of the pink coloration obtained in patients with low pigmentation of the NAC. The skin of the inguinoperineal region is better for reconstructions when a darker NAC is desired3,4,6.
The "nipple-banking" technique was described by Millard et al.7, in 1971. This technique originally involves removing the NAC and transferring it to the buttocks, groin, or abdomen as a total skin graft during mastectomy. After breast reconstruction, the grafts are collected and used for NAC reconstruction. However, questions regarding the safety of this method emerged after cases of patients with compromised lymph nodes with mammary cells in the inguinal region were reported when using the groin in this technique.
In the last 20 years, the major milestone of NAC reconstruction has been the use of local flaps. The first technique was reported by Berson8 in 1946; it involved use of 3 triangular skin flaps that were sutured to form the nipple projection. In 1984, Little9 developed the skate flap technique, which became the most popular technique for NAC reconstruction (Figure 1); the skate flap is a vertical dermo-fat flap that is elevated with both wings curled around a fat central nucleus to assure an adequate nipple projection. Meanwhile, dermapigmentation is used to restore the color of the NAC. Multiple modifications of this technique have emerged since then. Shestak & Nguyen10 described one very efficient technique called the "double-opposing flap," which enables NAC reconstruction with an adequate diameter, good projection, and symmetry with the contralateral side. In addition, the donor area can be closed, and all scars can be contained within the topography of the reconstructed areola.
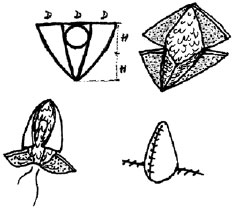
Figure 1 - Schematic of the skate flap.
This study presents the results of NAC reconstruction with the double opposing flap technique in breast reconstruction performed using various techniques, both immediate and late. Modifications of the original technique are also described.
METHODS
This retrospective study involved 24 patients in whom 31 NACs were reconstructed (17 unilateral and 7 bilateral) using the abovementioned technique between July 2008 and June 2010. Because of its versatility, this technique was used after reconstructions using myocutaneous flaps from the rectal abdominal muscle (TRAM) as well as flaps from the large muscle of the back (RGD) with prosthesis and expansion techniques. Variations in the thickness of the skin and fat pad in the region where the NAC was to be reconstructed as well as a history of radiotherapy did not preclude use of the double opposing flap technique.
In most patients, the NAC was reconstructed in the third surgery as described previously. However, in 8 cases, NAC reconstruction was conducted during symmetrization. In 2 patients who underwent reconstruction with RGD and prostheses, NAC reconstruction was performed during the first surgery, as described by Hammond et al.11.
The results were evaluated both objectively and subjectively. The subjective evaluation consisted of questionnaires administered in the doctor's office by a nurse technician. The patients classified their satisfaction level with the final results as "regular", "good", or "excellent".
In the objective evaluation, the reconstructed NACs and remaining areolas were measured once by the same nurse technician, who was properly oriented and trained. In particular, the horizontal diameter of the areola (HD) and nipple projection (NP) were measured. These data were analyzed by calculating means, standard deviations, medians, and maximum and minimum values. In addition, the Wilcoxon statistical test was used to test the hypothesis of similarity between the breasts; the level of significance was set at 5%. In particular, the similarities between the reconstructed and original NACs as well as 2 reconstructed NACs in cases of bilateral reconstruction were tested. The results are presented as line graphs and box plots.
Surgical Technique
Similar to most local flaps, double opposing flaps should be created after the projection of the new breast is stabilized during the second or third breast reconstruction.
In unilateral breast reconstructions, the position of the contralateral nipple, including its base diameter and projection as well as the horizontal and vertical measures of the areola, should be determined in order to ensure the symmetry of the reconstructed NAC.
The flap is designed with the nipple localized at the peak of the new breast while considering the contralateral areola in cases of unilateral reconstruction. The width of the base of the opposite nipple and its projection determine the size of the flap to be constructed. In cases of bilateral reconstruction, this measure should be determined on a case-by-case basis. However, in most cases, its dimensions should be between 10 mm and 12 mm (Figure 2). The width of the lateral extension determines the nipple projection. The length of the lateral extension should be between 20 mm and 22 mm but may reach 30 mm.
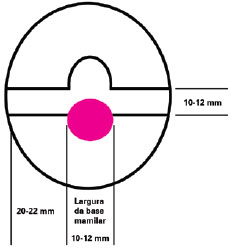
Figure 2 - Schematic of the double opposing flap including dimensions.
The areola of the opposite side should be carefully analyzed and measured. The NAC to be constructed should be planned to be 20% to 25% higher relative to the opposite side in order to obtain symmetry with respect to the contralateral side. A round block suture should be placed to equalize the dimensions and promote an over-projection of the reconstructed NAC with respect to the skin of the new breast. After 3 or 4 months, the diameter of the reconstructed NAC should be similar to that of the opposite side such that the dermapigmentation does not exceed the scar borders.
In bilateral reconstructions, the areolar measures should be approximately 50 mm. Moreover, the positioning should vary, aiming to provide a better blood supply to the elevated flap and the best available skin.
A modification adopted by our team is the oval form, which differs from the circular form proposed by Shestak & Nguyen10 (Figure 3).
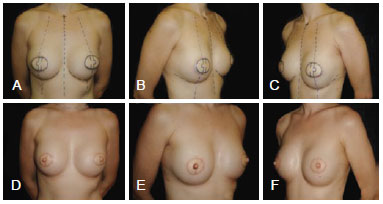
Figure 3 - Preoperative planning of bilateral nipple-areola complex reconstruction with double opposing flap in a patient submitted to bilateral mammary reconstruction using the latissimus dorsi muscle.
During the surgery, the flap is gently dissected just enough to allow it to be elevated 90º without compromising the blood supply; subsequently, it is sutured with nylon 5.0 or 6.0. After assembling the nipple, the suture described by Benneli12 (i.e., a round block suture) is placed using nylon 3.0 or 2.0 in the deep dermis to avoid extrusion and the risk of flattening the NAC in case the suture is subsequently removed. This suture should be firm and secure to promote close similarity between the diameters of the NACs. Conventional areola cutters are used to determine an adequate diameter for tying up the round block (Figure 4).
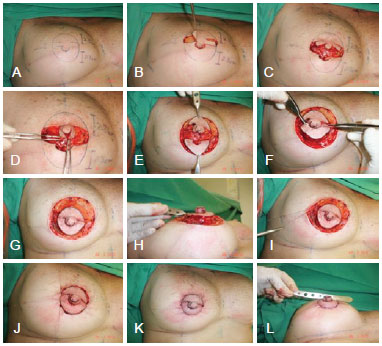
Figure 4 - Surgical steps illustrating the creation of the double opposing flap.
When NAC reconstruction is performed during the third surgery, local infiltration with 2% lidocaine is performed without use of vasoconstrictors and with support from an anesthesiologist for sedation and monitoring.
RESULTS
The sample included only women with an average age of 53 years and average follow-up of 18 months.
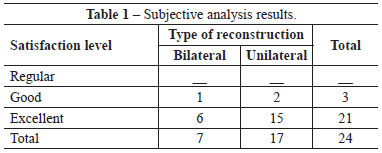
In the subjective analysis, the patient's satisfaction level with the final result was high in both unilateral and bilateral reconstructions (Table 1).
HD and NP were evaluated for the objective evaluation. In the analysis, P-values greater than 0.05 (i.e., 5%) were considered to indicate similarity.
The average difference between the measures of the reconstructed and contralateral NACs was evaluated in the unilateral reconstructions. The average values of HD and NP were 1.12 mm (P = 0.0817) and -0.18 mm (P = 0.4685), respectively (Table 2, Figures 5 and 6).
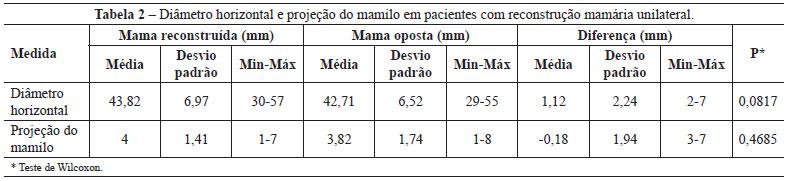
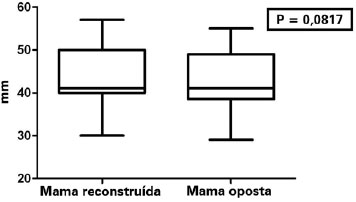
Figure 5 - Horizontal diameter of the areola in the unilateral mammary reconstructions.
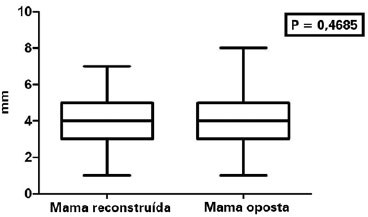
Figure 6 - Projection of the nipple in unilateral mammary reconstructions.
The analysis of HD and NP in the unilateral breast reconstructions did not reveal statistically significant differences (P > 0.05); therefore, both parameters were considered quantitatively similar between the reconstructed and contralateral breasts. Figures 7 and 8 show the curves between the reconstructed and contralateral breasts with respect to HD and NP, demonstrating the similarity of these analyzed parameters.
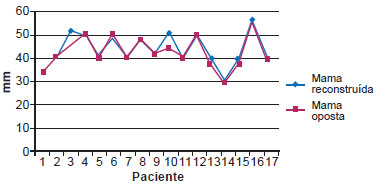
Figure 7 - Horizontal diameter of the areola in unilateral mammary reconstructions.
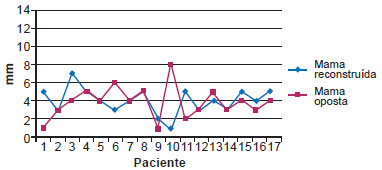
Figure 8 - Projection of the nipple in unilateral mammary reconstructions.
In bilateral breast reconstructions, the average differences were (right-left) −0.13 (P = 0.8302) and 0 (P = 1.000).
Table 3 and Figures 9 and 10 illustrate the results regarding HD and NP in bilateral breast reconstructions.
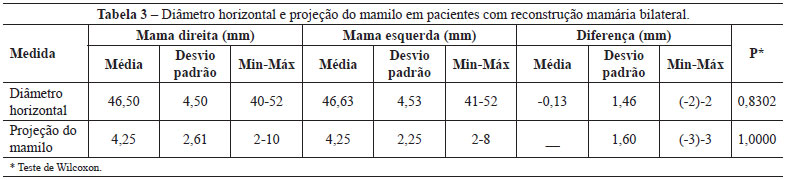
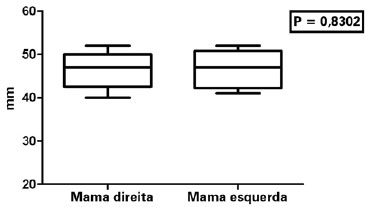
Figure 9 - Horizontal diameter of the areola in bilateral mammary reconstructions.
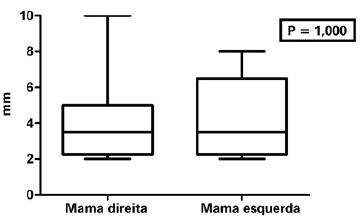
Figure 10 - Projection of the nipple in bilateral mammary reconstructions.
HD and NP in bilateral breast reconstructions were even more similar (Figures 9 and 10) than those in unilateral reconstructions (Figures 5 and 6). The curves in the graphs of bilateral reconstructions almost overlap, demonstrating high similarity between the right and left breasts with respect to HD and NP (Figures 11 and 12).
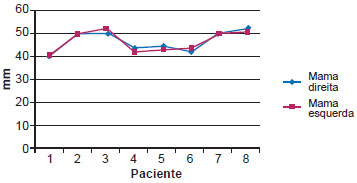
Figure 11 - Horizontal diameter of the areola in bilateral mammary reconstructions.
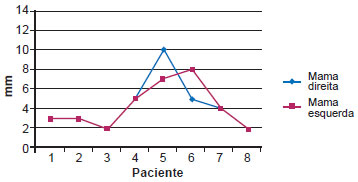
Figure 12 - Projection of the nipple in bilateral mammary reconstructions.
Among all reconstructions, only 3 patients developed partial necrosis of the flaps; this was treated with successive and curative mechanical debridement without compromising the final result.
DISCUSSION
Excellent results regarding NAC reconstruction are obtained when the positions, format, size, and texture are symmetrical in addition to permanent projection of the reconstructed nipple. In order to optimize the results, some standard rules should be followed regardless of the technique used.
According to Farhadi et al.13, NAC reconstruction should be delayed until a stable configuration of the new breast is obtained; this usually occurs from 4 months onwards after mammary reconstruction. In unilateral mammary reconstructions, the contralateral NAC should be used as a model. Nonetheless, the position must be adapted to the asymmetries of the remaining breast. Meanwhile, in bilateral mammary reconstructions, the localization of the NAC should be planned according to the anatomic references and esthetic preferences of the patient. A loss of projection of the reconstructed nipple should be expected in all cases as a result of scar retraction. Accordingly, during the planning of the new NAC, a hypercorrection of 25% to 50% of the desired result should be performed10.
The use of local flaps in NAC reconstructions has become popular since the first report by Berson et al.8. Since then, significant changes have been made by simplifying the flap design, mainly aiming to improve the blood supply and minimize the retraction forces. The vascularization was optimized by enlarging the subdermal plexus present in the base of the flap pedicle in addition to the increasing use of doubled pediculated flaps as well as an S-shaped flap, as first described by Cronin et al.14.
The ideal NAC reconstruction technique should be applicable to any type of tissue, regardless of previous scars and radiotherapy. In addition, the technique should ensure that the boundaries of the new NAC do not overcome the margins of the flaps used in the mammary reconstructions. Similarly, the ideal technique should not require the use of other areas of the body for source tissues. Furthermore, it should be possible to reconstruct a structure that simulates the areola as well as the papilla. Losken et al.15 (C-V flap), Anton et al.16 (star flap), Eskenazi17 (wrap flap), and Little9 (skate flap) reported results corroborating these ideas.
The double opposing flap guarantee these principles and also complies with previous markings, which determine all surgical steps and guidelines with respect to the form and perimeter of the new NAC10.
In the originally described technique, the round format proposed by Shestak & Nguyen10 does not guarantee precise positioning of the nipple in the center of the complex. The present work proposes an improvement of this technique because the flap is planned by drawing an oval format, which guarantees a centralized nipple in the boundaries of the reconstructed NAC (Figure 13).

Figure 13 - In A, representation of the "oval" format of the double opposing flap in a patient submitted to bilateral mammary reconstruction using a flap of the large muscle from the back. In B, 5th postoperative day demonstrating the centralized positioning of the nipple in the complex. In C, late postoperative period showing adequate nipple projection and positioning.
In cases involving irradiated flaps after reconstruction with expanders, RGD, or TRAM, this technique may be used without compromising local blood delivery10. Nevertheless, the flap may be autonomized as a result of serious distortions due to radiotherapy; this occurred in 2 patients in the present series, but the final result was satisfactory. A round block suture was placed, elevating the lateral flaps and the central portion of the flap. However, all sutures were not placed on the same day; after 15 days, the final sutures were placed in the doctor's office.
The round block suture is an important surgical step. This suture reduces the tension of the suture lines, thus allowing the NAC to circulate and migrate upwards or medially if necessary. Nevertheless, previous scars of mastectomies and transposed flaps can be used to create pexia and allow the new NAC to migrate in the desired direction. Thus, good positioning of the new NAC can be achieved without approaching areas with no scars, complying with the principle of not causing damage beyond the pre-defined limits of the double opposing flap.
Figure 14 illustrates a case in which it was necessary to mobilize the prosthesis downward during the reconstruction using the temporary expander as the NAC was being constructed, resulting in an adequate position.
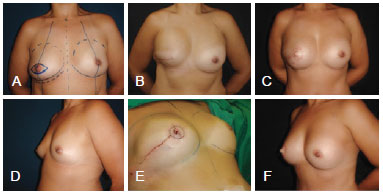
Figure 14 - A patient in which the repositioning of the prosthesis and NAC reconstruction were performed at the same surgical time. To avoid excess skin and allow the double opposing flap to migrate, centering it in the new breast and symmetrization its position with the opposite NAC, the yet unopened scar was used.
The technical refinements used in mammary reconstructions include liposuction and fat grafting, which play important roles in the correction of scar depressions or scars associated with radiation. These techniques allow regularization of flap thickness as well as symmetrization of the flaps and breasts, providing favorable aesthetic results18. In mammary reconstructions using expanders, there is often a shortage of tissues for adequate coverage, which hinders the subsequent utilization of local flaps for NAC reconstruction. With the aim of increasing the thickness of the flaps, which will be elevated to construct the new NAC, fat grafting is frequently used before the creation of the double opposing flap.
After accommodation and adequate healing of the reconstructed NAC, areolar dermapigmentation should be performed. Spear et al.19 state that this procedure helps maximize the natural appearance of the mammary reconstruction by providing areolar reconstructions compatible with the tonality of the skin of each patient.
While areolar reconstructions are simple to execute and difficulties are rarely encountered, the creation of a three-dimensional natural nipple with long-lasting projection remains a challenge. Bezerra et al.20 and Tostes et al.21 demonstrated long-term satisfactory results using autologous tissues and synthetic materials for the filling, respectively.
The variability of a nipple's presentation in its relaxed or erect form remains technically impossible to create. Because of the existing diversity of modalities for nipple reconstruction, each case should be approached individually, taking into consideration the local conditions of the tissues as well as the preferences of the surgeon and patient22.
The future of NAC reconstruction is directed towards the creation of more dynamic and functional structures obtained with the aid of genetic engineering23.
CONCLUSIONS
The double opposing flap is effective for NAC reconstruction with low rates of complications and a methodization that promotes a short learning curve.
The lack of invasiveness into distant areas is one of the major advantages of this technique. In this study, we slightly modified the original technique to reconstruct NACs with centralized nipples that are symmetrical to the contralateral side, providing long-term results.
REFERENCES
1. Adams WM. Labial transplant for correction of loss of the nipple. Plast Reconstr Surg. 1949;4(3):295-8.
2. Cronin TD, Upton J, McDonough JM. Reconstruction of the breast after mastectomy. Plast Reconstr Surg. 1977;59(1):1-14.
3. Schwartz AW. Reconstruction of the nipple and areola. Br J Plast Surg. 1976;29(3):230-3.
4. Broadbent TR, Woolf RM, Metz PS. Restoring the mammary areola by a skin graft from the upper inner thigh. Br J Plast Surg. 1977;30(3):220-2.
5. Brent B, Bostwick J. Nipple-areola reconstruction with auricular tissues. Plast Reconstr Surg. 1977;60(3):353-61.
6. Gruber RP. Nipple-areola reconstruction: a review of techniques. Clin Plast Surg. 1979;6(1):71-83.
7. Millard DR Jr, Devine J Jr, Warren WD. Breast reconstruction: a plea for saving the uninvolved nipple. Am J Surg. 1971;122(6):763-4.
8. Berson MI. Construction of pseudoareola. Surgery. 1946;20(6):808.
9. Little JW 3rd. Nipple-areola reconstruction. Clin Plast Surg. 1984;11(2):351-64.
10. Shestak KC, Nguyen TD. The double opposing periareola flap: a novel concept for nipple-areola reconstruction. Plast Reconstr Surg. 2007;119(2):473-80.
11. Hammond DC, Khuthaila D, Kim J. The skate flap purse-string technique for nipple-areola complex reconstruction. Plast Reconstr Surg. 2007;120(2):399-406.
12. Azzawi K, Humzah MD. Mammaplasty: the 'Modified Benelli' technique with de-epithelialisation and a double round-block suture. J Plast Reconstr Aesthet Surg. 2006;59(10):1068-72.
13. Farhadi J, Maksvytyte GK, Schaefer DJ, Pierer G, Scheufler O. Reconstruction of the nipple-areola complex: an update. J Plast Reconstr Aesthet Surg. 2006;59(1):40-53.
14. Cronin ED, Humphreys DH, Ruiz-Razura A. Nipple reconstruction: the S flap. Plast Reconstr Surg. 1988;81(5):783-7.
15. Losken A, Mackay GJ, Bostwick J 3rd. Nipple reconstruction using the C-V flap technique: a long-term evaluation. Plast Reconstr Surg. 2001;108(2):361-9.
16. Anton M, Eskenazi LB, Hartrampf CR Jr. Nipple reconstruction with local flaps: star and wrap flaps. Perspect Plast Surg. 1991;5(1):67-78.
17. Eskenazi L. A one-stage nipple reconstruction with the "modified star" flap and immediate tattoo: a review of 100 cases. Plast Reconstr Surg. 92(4):671-80.
18. Erdim M, Tezel E, Numanoglu A, Sav A. The effects of the size of liposuction cannula on adipocyte survival and the optimum temperature for fat graft storage: an experimental study. J Plast Reconstr Aesthet Surg. 2009;62(9):1210-4.
19. Spear SL, Convit R, Little JW 3rd. Intradermal tattoo as an adjunct to nipple-areola reconstruction. Plast Reconstr Surg. 1989;83(5):907-11.
20. Bezerra FJF, Moura RMG, Costa VRS. Reconstrução papilar: preenchimento com tecido autólogo ou heterólogo. Rev Bras Cir Plást. 2010;25(1):200-4.
21. Tostes ROG, Silva KDA, Andrade Júnior JCCG, Ribeiro GVC, Rodrigues RBM. Reconstrução do mamilo por meio da técnica do retalho C-V: contribuição à técnica. Rev Bras Cir Plást. 2005;20(1):36-9.
22. Banducci DR, Le TK, Hughes KC. Long-term follow-up of a modified Anton-Hartrampf nipple reconstruction. Ann Plast Surg. 1999;43(5):467-70.
23. Cao YL, Lach E, Kim TH, Rodríguez A, Arévalo CA, Vacanti CA. Tissue-engineered nipple reconstruction. Plast Reconstr Surg. 1998;102(7):2293-8.
1. Plastic surgeon, full member of Sociedade Brasileira de Cirurgia Plástica (Brazilian Society of Plastic Surgery - SBCP), preceptor of the Plastic Surgery Service at the Daher Hospital in Lago Sul, Brasília, DF, Brazil
2. Aspiring member in training of SBCP, resident doctor in Plastic Surgery Service at the Daher Hospital in Lago Sul, Brasília, DF, Brazil
3. Plastic surgeon, full member of SBCP, head of the Plastic Surgery Service at the Daher Hospital in Lago Sul, Brasília, DF, Brazil
4. Plastic surgeon, specialist member of SBCP, staff of Plastic Surgery Service at the Daher Hospital in Lago Sul, Brasília, DF, Brazil
5. Academic in Medicine at the Universidade Católica de Brasília (Catholic University of Brasília), Brasília, DF, Brazil
Correspondence to:
Jefferson Di Lamartine SCN Quadra 2 - Torre A - Salas 1121/1123 - 11º andar - Shopping Liberty Mall
Brasília, DF, Brazil - CEP 70712-900
E-mail: jefferson@dilamartine.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: February 7, 2012
Article accepted: November 15, 2012
This study was performed at the Daher Hospital in Lago Sul, Brasília, DF, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket