



Case Report - Year 2013 - Volume 28 -
Histopathology of Keith's lip scar
Histopatologia da forma labial cicatricial de Keith
ABSTRACT
Examinations of the etiology of congenital cicatricial presentations, which include congenital constriction bands and cicatricial presentations of cleft lip, have provided several theories that explain their development; however, they do not explain all the aspects involved in these malformations. In the present article, we present the cases of 4 patients with Keith's lip scar who underwent cheiloplasty using the spina technique. These cases were compared with 1 case of a patient with a traumatic scar. Tissue samples were obtained from all the patients for histopathological examination using hematoxylin-eosin staining. The cases under study exhibited similarities in embryonic skin and common scar tissue.
Keywords: Cleft lip. Lip diseases. Mouth abnormalities. Amniotic band syndrome.
RESUMO
O estudo da etiologia das formas congênitas ditas cicatriciais, que incluem bandas cicatriciais congênitas e formas cicatriciais das fissuras labiais, apresenta diversas teorias, que fundamentam seu aparecimento, porém não justificam todos os aspectos envolvidos nessas malformações. Neste artigo são apresentados 4 casos de pacientes portadores da forma cicatricial de Keith, submetidos à realização de queiloplastia pela técnica de Spina, comparados a 1 caso de paciente portador de cicatriz traumática. Todos os pacientes tiveram amostra de tecido enviada para estudo histopatológico, com coloração com hematoxilina-eosina. Os casos estudados apresentaram semelhanças entre a pele embrionária e a cicatriz comum.
Palavras-chave: Fenda labial. Doenças labiais. Anormalidades da boca. Síndrome de bandas amnióticas.
Despite the fast pace of the research in this field, the knowledge on the pathogenicity of congenital malformations has not increased by a great extent.
In 1976, we assessed congenital malformations known as cicatricial malformations1 in the cleft lip and palate, which include congenital constriction bands of the limbs and Keith's lip scars2. Since then, no significant scientific advances in this field have been made. Several theories address distinct aspects of the malformations; however, they do not offer a comprehensive explanation that could provide a solution to the problem.
Some authors such as Brindeau et al.3 argue that congenital constriction bands of the limbs are caused by amniotic anomalies. However, other researchers state that the amniotic anomalies are a result and not the cause of congenital constriction bands of the limbs. Streeter4 postulated that focal deficiency develops in fetal tissues as a result of failure of these structures, which prevents their full development. According to Inglis5, focal deficiency of fetal tissues is caused by intrinsic and extrinsic factors during an early stage of development.
Patterson6 claimed that the congenital constriction bands of the limbs are mainly the result of errors in the development of subcutaneous tissue, and he was the first researcher to compare them to Keith's lip scars.
Although many theories have been put forward regarding the etiology of these "cicatricial" presentations, and some authors such as Swanson et al.7 have compared them to a bridge-shaped scar of a third-degree burn, other researchers are more cautious and state that these congenital malformations only resemble a scar4.
Given the contradictory opinions found in the literature, the aim of the present work was to conduct a histopathological study of cicatricial lip presentations.
CASE REPORTS
This article presents the cases of 4 patients with Keith's lip scar who underwent cheiloplasty using the spina technique. These cases were compared to 1 case of a patient with a traumatic scar.
Tissue samples were obtained from all the patients for histopathological examination using hematoxylin-eosin staining.
Case 1
A 17-year-old female patient presented with Keith's lip scar, cleft nose, and congenital fistulas of the lower lip (Figure 1). The result of the histological examination of the tissue sample obtained during cheiloplasty showed a thin epidermis with melanin pigment in the basal layer and few dermal papillae (Figure 2). The dermis exhibited dense connective tissue. Skin adnexa, normal blood vessels, and nerve fascicles were present, in addition to a mildly basophilic amorphous substance.

Figure 1 - Case 1. Patient with Keith's lip scar, cleft nose, and congenital fistulas of the lower lip.

Figure 2 - Case 1. Result of the histological examination of a sample obtained during cheiloplasty, showing a thin epidermis with the presence of melanin pigment in the basal layer and few dermal papillae.
Case 2
A 46-year-old male patient presented with Keith's lip scar and cleft nose (Figure 3). The result of the histological examination of the sample obtained during cheiloplasty showed a thin epidermis with melanin pigment in the basal layer and the absence of dermal papillae and dense connective tissue in the dermis (Figure 4). In addition, skin adnexa, normal blood vessels, and nerve fascicles were present.

Figure 3 - Case 2. Patient with Keith's lip scar and cleft nose.
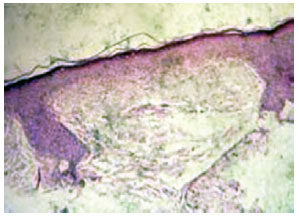
Figure 4 - Case 2. Result of the histological examination of a sample obtained during cheiloplasty, showing a thin epidermis with the presence of melanin pigment in the basal layer and absence of dermal papillae and dense connective tissue in the dermis.
Case 3
A 12-year-old male patient presented with Keith's lip scar and cleft nose (Figure 5). The result of the histological examination of the sample obtained during cheiloplasty showed a thin epidermis with melanin pigment in the basal layer and dermal papillae (Figure 6). The dermis exhibited dense connective tissue. Skin adnexa were present in large quantities; moreover, only few blood vessels were present, and nerve fascicles were absent.

Figure 5 - Case 3. Patient with Keith's lip scar and cleft nose.

Figure 6 - Case 3. Result of the histological examination of a sample obtained during cheiloplasty, showing a thin epidermis with the presence of melanin pigment in the basal layer and dermal papillae.
Case 4
A 43-year-old male patient presented with Keith's lip scar and cleft nose (Figure 7). The result of the histological examination of the sample obtained during cheiloplasty showed thick epidermis and few, though differentiated, dermal papillae (Figure 8). The dermis exhibited dense connective tissue. Skin adnexa and few blood vessels were absent.

Figure 7 - Case 4. Patient with Keith's lip scar and cleft nose.

Figure 8 - Case 4. Result of the histological examination of a sample obtained during cheiloplasty, showing a thick epidermis and fewer but differentiated dermal papillae.
Case 5
A 21-year-old male patient presented with an 18-year-old traumatic scar (Figure 9). The result of the histological examination revealed a thin epidermis and absence of dermal papillae (Figure 10). The dermis was composed of dense connective tissue. Skin adnexa was absent.
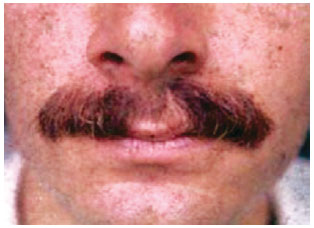
Figure 9 - Case 5. Patient with a traumatic scar.
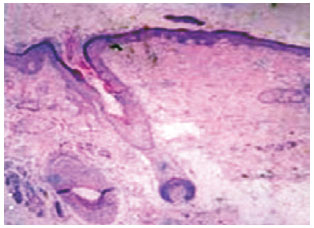
Figure 10 - Case 5. Result of the histological examination result showing a thin epidermis and the absence of dermal papillae.
DISCUSSION
Structural and/or metabolic congenital anomalies occur in 3-4% of the population aged <1 year. Thus, growth and fusion of embryonic buds (when referring solely to the face) occur in an environment favorable to small structural "errors" and, as Keith2 clarified, this is an "in utero" scarring that does not leave marks or sequelae.
In the present study, we observed that the congenital scar exhibits histological features similar to those of a common scar, which is formed "extra utero," and other features similar to those of embryonic skin. In addition, the presence of the melanin pigment and the absence or scarcity of dermal papillae were noted. The dermis was either normal or exhibited an amorphous substance similar to that observed during hyalinization, which resembles scarring. In some aspects, such as in case 2, it is very similar to an embryonic stage of skin development.
Therefore, the congenital scar is a mosaic that reveals a natural error, which many researchers have tried to explain through a variety of theories that may explain some but not all cases. We agree with Keith2 when he referred to an "in utero" scar; in fact, if we were able to understand and study in greater detail all the phenomena regarding the fusion of embryonic buds, and if we could simulate the same parameters and intrauterine conditions when performing surgery, we would be able to operate without leaving noticeable scars in most cases.
REFERENCES
1. Gonella HA. Histopatologia das formas congênitas ditas cicatriciais. In: XIII Congresso Brasileiro de Cirurgia Plástica, I Congresso Brasileiro de Cirurgia Estética; 1976; Porto Alegre. p. 303-4.
2. Keith A. Evolutionary wounds. Br Med J. 1921;2:137-9.
3. Brindeau A, Latuejoul P, Chappaz G. Des malformations d'origine amniotique arrest de developpement ou maladies de la membrane amniotique. Sem Hop Paris. 1952;71:2269.
4. Streeter GL. Focal deficiencies in fetal tissues and their relation to intrauterine amputations. Cont Embryol. 1930;22:1.
5. Inglis K. The nature of agenesis and deficiency of parts: the influence of intrinsic factors in disease when development of the body is abnormal, as illustrated by agenesis of the digits, facial hemiatrophy, and cerebral agyria and microgyria. Am J Pathol. 1952;28(3):449-75.
6. Patterson TJ. Congenital ring-constrictions. Br J Plast Surg. 1961;14:1-31.
7. Swanson AB, Barsky AJ, Entin MA. Classification of limb malformations of the basis of embryological failures. Surg Clin North Am. 1968;48(5):1169-79.
1. Plastic surgeon, full member of the Sociedade Brasileira de Cirurgia Plástica (Brazilian Society of Plastic Surgery - SBCP), full professor at the Department of Surgery of the Faculdade de Ciências Médicas e da Saúde de Sorocaba da Pontifícia Universidade Católica de São Paulo (Faculty of Medical and Health Sciences of Sorocaba, Pontifical Catholic University of São Paulo - PUC-SP), Sorocaba, SP, Brazil
2. Plastic surgeon, associate member of the SBCP, former resident at the Department of Surgery of the Faculdade de Ciências Médicas e da Saúde de Sorocaba da Pontifícia Universidade Católica de São Paulo (Faculty of Medical and Health Sciences of Sorocaba, Pontifical Catholic University of São Paulo - PUC-SP), Sorocaba, SP, Brazil
Correspondence to:
Hamilton Aleardo Gonella
Rua Afonso Cavalline, 142 - Santa Rosália
Sorocaba, SP, Brazil - CEP 18090-160
E-mail: hagonella@hotmail.com
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: September 16, 2010
Article accepted: November 5, 2010
This study was performed at the Faculty of Medical and Health Sciences of Sorocaba, Pontifical Catholic University of São Paulo (PUC-SP), Sorocaba, São Paulo, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket