



Case Report - Year 2014 - Volume 29 -
Versatility of the anterolateral thigh flap in oncology reconstructions: Case reports of the reconstructive plastic surgery and microsurgery procedures in Erasto Gaertner Hospital
A versatilidade do retalho anterolateral da coxa em reconstruções oncológicas: série de casos do serviço de cirurgia plástica reconstrutora e microcirurgia do hospital Erasto Gaertnera
ABSTRACT
INTRODUCTION: The anterolateral thigh (ALT) flap first described in 1984 is based on perforator vessels of the lateral femoral circumflex artery. It is a cutaneous flap located in the middle third of the anterior thigh and lateral to the rectus femoris and vastus lateralis. The low morbidity related to the donor site and its usefulness for different dimensions make it a versatile flap.
OBJECTIVE: This study aimed to present the versatility of the ALT flap in plastic and reconstructive surgeries at the Erasto Gaertner Hospital through a report of three cases.
CASES: We describe three cases in which the ALT flap was used for the head and neck, and right hemithorax reconstructions.
Keywords: Anterolateral Thigh Flap; Microsurgery; Versatility of the Flap.
RESUMO
INTRODUÇÃO: Retalho anterolateral da coxa (ALT) foi descrito em 1984, baseado nos vasos perfurantes da artéria circunflexa femoral lateral. Trata-se de um retalho cutâneo, localizado no terço médio da coxa anterior, e lateral aos músculos reto femoral e vasto lateral. A baixa morbidade, relacionada à área doadora, e a possibilidade de utiliza-lo com diversas dimensões o tornam um retalho muito versátil.
OBJETIVO: Apresentar sua versatilidade no serviço de Cirurgia Plástica Reconstrutora e Microcirurgia, do Hospital Erasto Gaertner, através do relato de três casos.
CASOS: Foram descritos dois casos com utilização do retalho ALT para reconstrução de cabeça e pescoço, e um caso com reconstrução do hemitórax direito.
Palavras-chave: Retalho anterolateral da coxa; Microcirurgia; Versatilidade do retalho.
Plastic surgery has greatly advanced in terms of the use of the microsurgical flap, often in cases of defects and complex deformities for the covering of articular surfaces, vessels, tendons, and bones with the periosteum removed, with the objective of restoring function and shape1.
For this purpose, these flaps must be adapted in their dimension and composition. They can be simple or compound flaps, transferred at one time from one part of the body to another, and modified for a specific defect. It is important to highlight that the anterolateral thigh (ALT) flap became popular in the recent years for its advantages that include long and large pedicles, reduced thickness, cutaneous sensitivity, possibility of flow through or chimerical construction, three-dimensional covering and filling of the cavities (due to its malleability), and minimum morbidity of the donor area1.
The ALT flap, initially described by Song et al in1984, was based on the perforations of the lateral femoral circumflex artery. It consists of a fasciocutaneous flap located in the middle third of the anterior thigh and lateral to the rectus femoris and vastus lateralis. Its measures may reach 20 ' 40cm; however, traditionally, flaps with smaller dimensions, which are safer, are used2.
Considering the great importance of the use of ALT flaps, this study aimed to show their versatility by reporting three cases selected at the plastic and reconstructive surgery, and microsurgery departments of Erasto Gaertner Hospital (Curitiba, Paraná), which is the national reference center for the treatment of cancer.
CASES
Case 1
A 58-year-old female patient underwent mastectomy for adenocarcinoma. She presented with a recurrent tumor invading the thoracic wall. Metastatic tumor resection resulted in deformity of the thoracic wall. Reconstruction of the left hemithorax was performed using an ALT microsurgical flap. The flap showed good postoperative viability (Figure 1A and B; Figure 2A and B).

Figure 1(A)- Right thigh anterolateral flap lifted. (B)- Panoramic view of the donor area.

Figure 2(A)- Receptor area after tumor removal. (B)- Immediate postoperative thoracic reconstruction.
Case 2
A 34-year-old female patient underwent maxillectomy and orbital exenteration of invasive contralateral breast cancer (CBC). The left hemiface was reconstructed with an ALT flap (Figure 3A-C; Figure 4A and B).
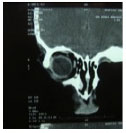
Figure 3(A)- Coronal computed tomographic scan demonstrating the absence of the orbital floor and side wall of the orbit and jaw. (B)- Frontal view of the patient after exenteration of the left orbit. (C)- Profile picture.

Figure 4(A) - Oblique view of the patient after reconstruction with the anterolateral thigh flap. (B)- Front view.
Case 3
A 52-year-old male patient underwent orbital exenteration of invasive CBC with reconstruction using an ALT flap (Figure 5A and B).

Figure 5(A) - Frontal view of the patient after exenteration of the right orbit. B- Oblique image after reconstruction with an anterolateral thigh flap.
DISCUSSION
The ALT flap is versatile, as it can be modified to suit the receptor area. It is considered an ideal flap owing to the following factors: long pedicle, vessels with good diameter, availability of several types of cutaneous tissue or muscles with the same pedicle, great extension of the skin, and low morbidity of the donor area3.
These characteristics of the flap allow successful thoracic reconstructions because it is a larger flap and has the advantage of being fasciocutaneous without causing functional damage to the donor area.
The location of the donor area and possibility of lifting the flap in the supine position allow two teams to work simultaneously in the reconstruction of the head, neck, and upper limbs, reducing the total surgery time, and physical and mental fatigue of the team. In reconstruction of the legs, it allows surgical manipulations to be restricted to only one lower limb with regional anesthesia4.
The cases described demonstrate satisfactory functional and esthetic results with the use of the ALT flap for head and neck reconstruction surgeries, besides the high resolution in the treatment of oral and nasal fistulas after maxillary removal. It also results in lower morbidity of the donor area compared to the radial anterobrachial flap. ("Chinese").
The descending branch of the femoral circumflex artery is primarily responsible for the arterial irrigation of the ALT area. The system of this vessel is formed by the femoral circumflex artery itself, its ascending, transverse, and descending branches, and perforating cutaneous, muscular, facial, and bone tissue branches5.
This rich vascular system allows creation of flaps with the following tissues: skin from the anterolateral and anteromedial thigh region, and lateral vastus, femoral rectus, sartorius, fascia lata tensor, and iliac crest muscles, totaling 120 different combinations6.
The flap under discussion can also be transferred in the form of a fascial or adipofascial flap, and a cutaneous flap with the graft of the vascularized femoral nerve for the simultaneous reconstruction of skin and peripheral nerve7.
In an experience with 8,500 microsurgical flaps, Chen and Tang (2003), from the Chang Gung Memorial Hospital in Taiwan, affirmed that the ALT flap replaces other flaps. Among 1,500 ALT flaps, in only 12% of the patients the path of the perforating vessels was septocutaneous, while in the other 88%, the path of the vessels was musculocutaneous. The peduncle, in turn, varied from 8 to 20 cm. The anatomy was relatively constant, allowing easy and safe dissection. Only 2-3% of the dissections were considered difficult due to the absence of perforating vessels or a perforator artery that did not accompany the vein8.
More recently, in his doctorate thesis, Ishida (2006) studied 100 thighs of 50 fresh cadavers. He found 0-4 perforator arteries per thigh, all in an area of 6 cm from the midpoint between the anterosuperior iliac spine and the upper lateral edge of the patella. The perforating vessels had a musculocutaneous path in 75.76% and septocutaneous in 24.24%. The pedicle presented a mean length of 11.31 ± 3.12cm. The arterial diameter was 2.21 ± 0.85mm, and the diameters of the veins from the same area were 2.66 ± 1.33mm and 2.1 ± 1.11mm. Finally, he highlighted that the mean subcutaneous thicknesses of the skin were 8.98 ± 6.25mm and 1.6 ± 0.76mm.1
CONCLUSION
The ALT flap can be lifted safely, independent of whether the path of the perforating vessels is septocutaneous or musculocutaneous. It has an ideal donor area due to the characteristics of its vascular anatomy mentioned earlier, such as easy lifting and great versatility. Thus, the ALT flap represents one of the most useful free flaps available9.
REFERENCIS
1. Ishida, L. C. Estudo anatômico do retalho perfurante ântero-lateral da coxa; Anatomic study of the anterolateral thigh flap. Universidade de São Paulo. Faculdade de Medicina, 2006.
2. Pinheiro BS, Freitas FB, Olivan M., Soller PC, Castro MF. Retalho anterior da coxa estendido: uma variação do retalho ântero-lateral para a cobertura de grandes defeitos de partes moles.Rev. Bras. Cir. Plást. 2010;25(supl):1-102
3. Wei, FC, Jain, V, Celik, N, Chen, HC, Chuang, DC, Lin, CH. Have we found an ideal soft-tissue flap? An experience with 672 anterolateral thigh flaps.Plast Reconstr Surg. 2002;109:2219-2226; discussion 2227-2230.
4. Koshima, I, Yamamoto, H, et al. Free combined composite flaps using the lateral circumflex femoral system for repair of massive defects of the head and neck regions: an introduction to the chimeric flap principle. Plast Reconstr Surg. 1993;92:411-420.
5. Kawai, K, Imanishi, N, Nakajima, H. Aiso, S, Kakibuchi, M, Hosokawa, K. Vascular anatomy of the anterolateral thigh flap. Plast Reconstr Surg. 2004;114:1108-1117.
6. Hallock, G. G. Muscle perforator flaps: the name game. Ann Plast Surg. 2003;51:630-632.
7. Kimata, Y, Uchiyama, K, Ebihara, S, et al. Versatility of the free anterolateral thigh flap for reconstruction of head and neck defects. Arch Otolaryngol Head Neck Surg. 1997;123:1325-1331.
8. Chen, HC, Tang, YB. Anterolateral thigh flap: an ideal soft tissue flap. Clin Plast Surg. 2003;30:383-401.
9. Gedebou, TM, Wei, FC, Lin, CH. Clinical experience of 1284 free anterolateral thigh flaps. Handchir Mikrochir Plast Chir. 2002;34:239-244.
1- Plastic Surgeon , Member of the Brazilian Society of Plastic Surgery , Head of the Plastic Surgery Department of Erastus Gaertner Hospital , Curitiba - PR - Brasil.- Head of the Plastic Surgery Department of Erastus Gaertner Hospital , Curitiba - PR - Brazil
2- Plastic Surgeon , Member of the Brazilian Society of Plastic Surgery, Plastic Surgery Department of Erastus Gaertner Hospital , Curitiba - PR - Brazil.- Member of the Brazilian Society of Plastic Surgery
3- Surgeon General- Resident Plastic Surgery, Clinical Hospital of UFPR
4- Plastic Surgeon and craniomaxillofacial , Specialist Member of the Brazilian Society of Plastic Surgery and the Brazilian Association of Craniomaxillofacial Surgery, Plastic Surgery Department of Erastus Gaertner Hospital , Curitiba - PR - Brazil.- Specialist Member of the Brazilian Society of Plastic Surgery and the Association Brazilian craniomaxillofacial surgery
5- Resident of Plastic and Reconstructive Surgery of UFPR Clinical Hospital , Curitiba - PR - Brazil.- Resident of Plastic and Reconstructive Surgery at the Hospital of the UFPR , Curitiba - PR - Brazil
6- Resident of Plastic and Reconstructive Surgery at the Hospital Cajuru PUC- PR , Curitiba - PR - Brazil- Resident of Plastic and Reconstructive Surgery at the Hospital Cajuru PUC- PR , Curitiba - PR - Brazil
Institution: Federal University of Paraná, Hospital Erasto Gaertner - Curitiba, Paraná.
Autor correspondente:
Ivan Maluf Júnior
Rua Riachuelo, 31 - Centro
Curitiba/PR - Brasil - CEP: 80240-020
E-mail: ivanmaluf@yahoo.com.br
Article received: November 9, 2013
Article accepted: June 1, 2014
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket