



Original Article - Year 2014 - Volume 29 -
Epidemiological profile of patients treated by the plastic surgery service of the João XXIII hospital in Belo Horizonte/MG from March to August 2013
Perfil epidemiológico dos pacientes atendidos pelo serviço de cirurgia plástica do hospital João XXIII em Belo Horizonte/MG no período de março à agosto de 2013
ABSTRACT
INTRODUCTION: The Plastic Surgery Service of the João XXIII Hospital provides support to other specialties through interdepartmental consultation and follows patients admitted to the hospital for plastic surgery. This study analyzed the epidemiological profile of patients treated from March to August 2013.
METHODS: This was a prospective observational study with data collection performed by medical history and physical examination.
RESULTS: Of the patients evaluated, 75.23% were male and 21.34% female. The predominant age group was economically active, with 62.86% of the patients between 16 and 45 years. Traffic accidents were the main reason for care (44.85%). Pressure ulcers were the most frequent diagnoses, and other lesions evaluated were predominantly of the extremities. Internal Medicine and Orthopedics requested most consultations. Surgical treatment (52.9%) and follow-up with local care (47.1%) showed similar frequencies.
CONCLUSION: In order to propose measures for prevention and treatment of injuries within the scope of reconstructive plastic surgery, two issues were highlighted: traffic accidents and pressure ulcers. Both have well-defined causes, but remain at high prevalence. The need for public action that promotes better traffic education and reduction of accidents is clear. In the hospital environment, it is essential to take effective measures to prevent the emergence of dreaded pressure ulcers.
Keywords: Plastic surgery; Epidemiology; High-volume Hospitals; Inpatients; Surgical specialties; Diagnosis.
RESUMO
INTRODUÇÃO: O Serviço de Cirurgia Plástica Programada do Hospital João XXIII exerce o suporte às demais especialidades através de interconsultas e, realiza atendimento aos pacientes com entrada no Hospital pela cirurgia plástica. O escopo deste estudo foi analisar o perfil epidemiológico dos pacientes atendidos durante o período de Março à Agosto de 2013.
MÉTODOS: Trata-se de um estudo observacional prospectivo com coleta de dados realizada através de anamnese e exame físico.
RESULTADOS: Dentre os pacientes avaliados 75,23% eram do sexo masculino e 21,34% do sexo feminino. A faixa etária predominante foi a economicamente ativa com 62,86% dos pacientes entre 16 e 45 anos. Foi observado que os acidentes de trânsito figuraram como os principais determinantes de atendimentos (44,85%). As escaras constituíram os diagnósticos mais frequentes e dentre as outras lesões avaliadas, observou-se que se concentraram nos membros. A Clínica Médica e a Ortopedia solicitaram o maior número de interconsultas. Evidenciou-se que o tratamento através de abordagem cirúrgica (52,9%) e o acompanhamento com cuidados locais (47,1%) apresentaram frequências aproximadas.
CONCLUSÃO: Na busca por propor medidas para prevenir e tratar as lesões próprias de abrangência da cirurgia plástica reparadora destacaram-se dois pontos: os acidentes de trânsito e as escaras de decúbito. Ambos com fatores determinantes bem elucidados, porém mantendo alta prevalência. Torna-se evidente a necessidade de atuação nas esferas públicas para uma melhor educação no trânsito e redução da ocorrência de acidentes. No âmbito hospitalar é primordial que se adotem medidas eficazes que impeçam o surgimento das temíveis escaras de decúbito.
Palavras-chave: Cirurgia plástica; Epidemiologia; Hospitais com Alto Volume de Atendimentos; Pacientes Internados; Especialidades Cirúrgicas; Diagnóstico.
The Pronto-Socorro João XXIII Hospital (HPS), located in Belo Horizonte/MG and founded in 1973, was affiliated with the State Foundation for Emergency Medical Assistance (Feamur); in 1977, it was incorporated into the Hospital Foundation of the State of Minas Gerais (FHEMIG). The HPS acts as a referral center for patients with multiple trauma, major burns, poisoning, and clinical and/or surgical situations that present risk of death1. The Programmed Plastic Surgery Service provides support to other medical specialties through interdepartmental consultations requested by the patient's physician, and provides care to individuals followed by the specialty of reconstructive plastic surgery.
OBJECTIVE
This essential study analyzed the epidemiological profile of patients treated by the Programmed Plastic Surgery Service of the HPS from March to August 2013. This study is essential because additional knowledge of the patients may lead to effective measures for prevention and treatment of injuries covered by reconstructive plastic surgery.
METHOD
This was a descriptive, observational, and prospective study of the epidemiological profile of patients assessed by the Programmed Plastic Surgery Service from March to August 2013. Variables such as age, gender, diagnosis prompting consultation or care, specialty requesting consultation, admitting diagnosis, treatment administered, and length of stay on the Scheduled Plastic Surgery Service were analyzed. All patients followed by the Plastic Surgery Service in this period were assessed; this service exclusively follows users of the Unified Health System.
Data collection was performed through history and physical examination during consultation and care. Patients were divided into the following age groups: 0-15y, 16-30y, 31-45y, 46-60y, and over 60y. The diagnosis prompting evaluation was divided into two major groups: pressure ulcers and other injuries, the latter compiled in subgroups. In addition to direct admissions to the Plastic Surgery specialty, consultations requested by each medical specialty (Orthopedics, Internal Medicine, Neurosurgery, Pediatrics, General Surgery, Hand Surgery, and Vascular Surgery) and dental specialty (Oral and Maxillofacial Surgery and Traumatology) were recorded. The initial diagnosis that led to the hospitalization of the patient was classified into 11 groups: automobile accidents, motorcycle or bicycle accidents, being run over, assault with firearm or other weapon, assault without a weapon, falls from heights and landslides, simple falls, medical conditions, accidents involving animals, accidental trauma with glass/sharp objects/crushing/fireworks, and causes not classified in other groups.
The treatment was initially divided into two groups: surgical treatment and wound care dressings with no surgical intervention. The first group was further subdivided: debridement, skin grafting, flap construction, reconstruction of complex structures, incisional biopsy, and elastic and delayed suturing. The average length of stay of patients followed by plastic surgery was also determined.
RESULTS
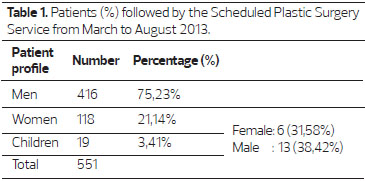
The total number of patients who visited HPS from March to August 2013 was 553, of whom 75.23% were male and 21.34% female. In all, 3.44% of patients were children (age less than 12 y), and 68.42% were male and 31.58% were female (Table 1).
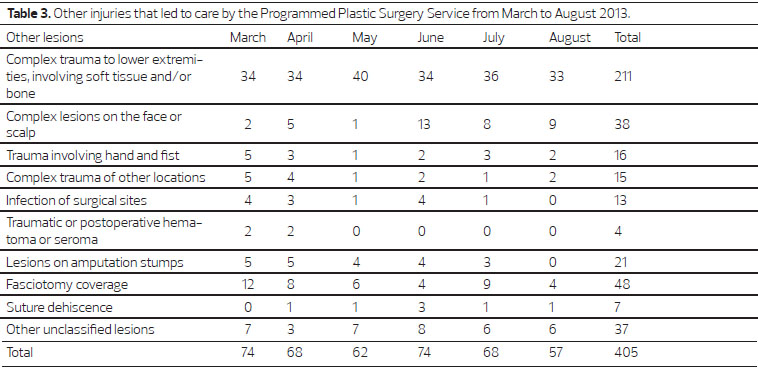
The predominant age range of the patients was economically active, with 30.82% of patients between 16 and 30 y and 32.04% between 31 and 45 y (Table 2). Among the injuries that led to treatment (Figure 1), pressure ulcers totaled 27%, and other lesions totaled 73%, grouped according to table 3.
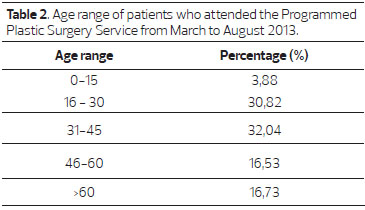
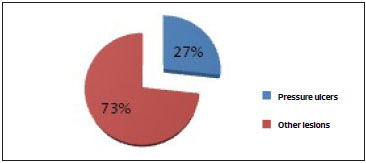
Figure 1. Injuries that prompted care by the at the Programmed Plastic Surgery Service from March to August 2013.
Pressure ulcers in the sacral region were present in more than 87% of cases (Table 4). The specialties of Internal Medicine (40.14%) and Orthopedics (21.52%) generated the largest consultation numbers. Direct admissions to Plastic Surgery accounted for 21.16% of patients under care (Figure 2).
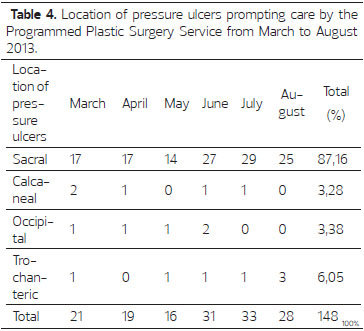
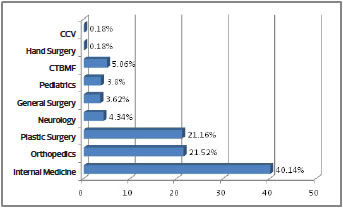
Figure 2. Specialties that requested consultation and attendance by the Scheduled Plastic Surgery Service from March to August 2013 (CCV- Vascular Surgery; CTBMF- Oral and Maxillofacial Surgery and Traumatology)
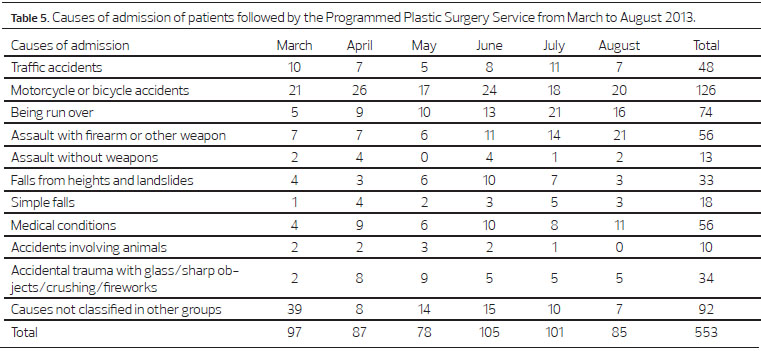
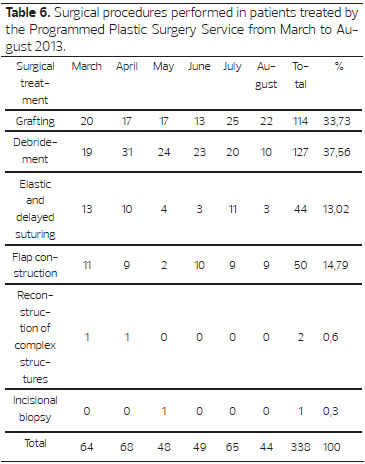
The initial events that led to hospitalization are listed in Table 5. Traffic accidents were clearly the major cause of hospitalization (248 cases, 44.85%). The preliminary collection of data resulted in a total of 338 (52.9%) surgical procedures, and 301 (47.1%) follow-ups with local specialist care without surgical intervention. Surgical treatment showed a predominance of graft procedures (33.73%) and debridement (37.56%) as shown in Table 6.
Patients with pressure ulcers were followed an average of 16.78 days by the Programmed Plastic Surgery Service, and patients with other lesions had an average of 11.70 days of follow-up (Figure 3).
Figure 3. Average length of stay of patients followed by the Programmed Plastic Surgery Service from March to August 2013.
DISCUSSION
The epidemiological profile of the patients who visited the HPS revealed a predominance of male patients and an economically active age group; 75.23% of the treated patients were male. This highlights the high social and financial costs to the state, since these cases are associated with prolonged hospitalization and subsequent post-discharge absence from the patients' professional rehabilitation services. These patients usually are the main, if not the only, income providers for their family.
Traffic accidents directly affect citizens, are related to death, physical disability, and material losses, and may cause serious psychological damage that is often difficult to overcome2. The association found in this study between male patients in the age groups of 16-30 and 31-45 y and the occurrence of traffic accidents with injuries, is in agreement with the already solid statistics of the National Department of Transport Infrastructure (DNIT)2,3. According to data presented by the DNIT for 2011 and 2012, the number of male individuals involved in traffic accidents with injuries greatly exceeds the number of women involved in the same type of accidents, a common trend in all states of this country2. In this study, plastic surgery was the main reason why individuals involved in traffic accidents underwent interconsultations, accounting for 44.85%. The age group between 16 and 45 accounted for 62.86% of the patients evaluated from March to August 2013.
In all, 27% of all injuries requiring treatment were pressure ulcers or bedsores. These injuries can affect the cutaneous and subcutaneous tissues, can sometimes involve muscle tissue, and even bone or joints. They are common in patients who are bedridden for prolonged periods or those who are immobilized; being bed-bound or immobilized clinically causes tissue compression, followed by ischemic damage and subsequent necrosis4. These ulcers are usually located over a bony prominence5, and are a major complication in critically ill, hospitalized patients6. Four factors extrinsic to the patient can lead to these lesions: pressure, friction, shear, and moisture, with pressure considered the main cause6. The moisture resulting from perspiration, fecal, or urinary incontinence predisposes a patient to ulcers formation due to tissue maceration and damage5. Intrinsic factors that accompany the appearance of ulcers involve age, nutritional status, tissue perfusion, medication use, and chronic diseases, such as diabetes mellitus and cardiovascular disease6. Because HPS is a referral center for care of patients with multiple trauma and clinical and/or surgical situations with a risk of death1, patients who visit this institute have serious illnesses requiring admission in intensive care units and are immobilized in the supine position for prolonged periods; this predisposes patients to pressure ulcers in regions wherein ischemia developed owing to a prolonged supine position7-9. In this study, sacral ulcers were present in 87.16% of patients with pressure ulcers, and calcaneal ulcers were present in 3.38% patients, occipital ulcers in 3.38%, and trochanteric ulcers in 6.08 %. In Brazil, between 17.7% and 39.8% chronically ill and bedridden patients admitted to general hospitals have decubitus ulcers; in a study conducted with spinal cord injury patients in a teaching hospital, ulcers were observed in 42.5%10.
According to a proposal by the National Pressure Ulcer Advisory Panel (NPUAP)9, ulcers are defined by four stages. Stage I presents as non-blanching hyperemia in the intact skin, usually over a bony prominence; the color of darkly pigmented skin may differ from the surrounding area; the skin may be painful, with either firm or soft consistency. Stage II presents with partial-thickness dermis loss and a pale red-pink wound bed without sloughing, but can also present as an intact or open/ruptured, serum-filled or serosanguinous blister. Stage III presents with full-thickness skin loss, with visible subcutaneous fat, but no bone, tendon, or muscle exposure; sloughing may be present, and there may be undermining and tunneling. Stage IV presents with full-thickness tissue loss, with exposed bone, muscle or tendon; sloughing or eschar may be present in some parts of the wound bed; there is often undermining and tunneling; the depth of the lesion varies by anatomical location, and may be shallow or deep9. In addition to generating high costs, the development of pressure ulcers in patients seen by health services has a negative impact on their lives, as well as on their families10.
Among other injuries evaluated by the Reconstructive Plastic Surgery department during this period, the majority involved the limbs and included complex lesions with traumatic loss of substance, skin necrosis, or assessments for fasciotomy coverage, requiring debridement, grafting, or flap rotation.
The Internal Medicine and Orthopedics departments requested most of the consultations, to ensure complete clinical support in multiple trauma patients by the former, and due to the association between trauma of bone and soft tissue by the latter; this highlights the need for collaboration among specialties.
Surgical treatment (52.9%) and follow-up with local specialist care without surgical intervention (47.1%) had approximately similar frequencies; this demonstrates the importance of the specialty, not only for procedures, but also for the primary evaluation and the observation and clinical treatment of the patient.
The average length of hospital stay of patients with pressure ulcers was 16.78 days and of those with other lesions was of 11.70 days, under the supervision of the Programmed Plastic Surgery Service. This is consistent with the prolonged hospital stays in these patients; such long durations hinder recovery of the patient and increase the risk of infection or other complications, such as osteomyelitis6. This also increases physical and emotional suffering by the patient.
CONCLUSION
This study enabled understanding of the epidemiological profile of all patients treated and followed by the Scheduled Plastic Surgery Service of the HPS. In the quest for measures to prevent and treat injuries relevant to reconstructive plastic surgery, two areas were highlighted: traffic accidents and pressure ulcers. Both have well-known causes, but are highly prevalent. This highlights the need for preventive and effective public action to improve traffic education and reduce accidents. In the hospital environment, it is vital to strengthen measures that prevent the emergence of dreaded pressure ulcers.
In conclusion, plastic surgery is important for the primary evaluation and clinical treatment of the patient and for the support of other medical specialties, in order to provide a complete, ethical and decisive treatment for the patient.
REFERENCES
1. Hospital João XXIII Complexo de Urgências e Emergências. Histórico/Missão. Disponível em: <http://www.fhemig.mg.gov.br/pt/atendimento-hospitalar/complexo-de-urgencia-e-emergencia/hospital-joao-xxiii>. Acessado em: 23/10/2013.
2. DNIT - Departamento Nacional de Infraestrutura de Transportes. Disponível em: < http://www.dnit.gov.br/rodovias/operacoes-rodoviarias/estatisticas-de-acidentes>. Acessado em: 23/10/2013 às 17:55:23.
3. Brasil.gov.br. O trânsito em números. Disponível em: < http://www.brasil.gov.br/sobre/cidadania/gentileza-urbana/paz-no-transito/o-transito-em-numeros>. Acessado em: 23/10/2013 às 18:00:03.
4. Soares DA, Vendramin FS, Pereira LM, Proença PK, Marques MM. Análise da incidência de úlcera de pressão no Hospital Metropolitano de Urgência e Emergência em Ananindeua, PA. Rev Bras Cir Plást. 2011;26(4):578-81.
5. Michelone AP, Cardoso LA, Motta RP, Borella AC, Mello AP. Incidência de úlceras por pressão no Hospital de Clínicas I da Faculdade de Medicina de Marília- SP. Rev Esc Enf USP. 1999;23:207-10.
6. Blanes L, Duarte IS, Calil JA, Ferreira LM. Avaliação clínica e epidemiológica das úlceras por pressão em pacientes internados no Hospital São Paulo. Rev Assoc Med Bras. 2004;50(2):182-7.
7. Costa MP, Sturtz G, Costa FP, Ferreira MC, Filho TEP. Epidemiologia e tratamento das úlceras de pressão: Experiência de 77 casos. Acta Ortop Bras. 2005;13:124-33.
8. Costa IG. Incidência de úlcera por pressão em hospitais regionais de Mato Grosso, Brasil. Rev Gaúcha Enferm. 2010;31(4):693-700.
9. National Pressure Ulcer Advisory Panel (NPUAP). Conceito e classificação de úlcera por pressão: atualização do NPUAP. Rev Estima. 2007;5:43-4.
10. Ursi ES, Galvão CM. Ocorrência de úlcera por pressão em pacientes submetidos a cirurgias eletivas. Acta Pau Enf. 2012;25:653-9.
1 - Resident in Plastic Surgery - Resident on the Plastic Surgery and Burns Service, João XXIII Hospital, FHEMIG, Belo Horizonte, MG, Brazil
2 - Full member of the Brazilian Society of Plastic Surgery - Plastic Surgeon, member of the Brazilian Society of Plastic Surgery, Chief of the Plastic Surgery and Burns Service, João XXIII Hospital, FHEMIG, Belo Horizonte, MG, Brazil
3 - Full member of the Brazilian Society of Plastic Surgery. - Plastic Surgeon, member of the Brazilian Society of Plastic Surgery, Coordinator of the Scheduled Plastic Surgery Service, João XXIII Hospital, FHEMIG, Belo Horizonte, MG, Brazil
4 - Resident in Plastic Surgery - Resident on the Plastic Surgery and Burns Service, João XXIII Hospital, FHEMIG, Belo Horizonte, MG, Brazil
5 - Resident of Plastic Surgery - Resident of the Plastic Surgery and Burns Service, João XXIII Hospital, FHEMIG, Belo Horizonte, MG, Brazil
6 - Resident in Plastic Surgery - Resident on the Plastic Surgery and Burns Service, João XXIII Hospital, FHEMIG, Belo Horizonte, MG, Brazil
7 - Resident in Plastic Surgery - Resident on the Plastic Surgery and Burns Service, João XXIII Hospital, FHEMIG, Belo Horizonte, MG, Brazil
Institution: This study was conducted at the Pronto Socorro João XXIII Hospital affiliated with the FHEMIG Network, Belo Horizonte, MG, Brazil.
Corresponding author:
Cecília Borges de Souza
Rua Batista Carneiro, n. 174, apto 408 - Salgado Filho
Belo Horizonte, MG, Brasil - CEP: 30550-090
Telefone: (31) 8523-2538
E-mail: cecilia_borgesdesouza@yahoo.com.br
Article received: February 8, 2014
Article accepted: June 1, 2014
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket