



Original Article - Year 2014 - Volume 29 -
Omphaloplasty: back to the natural process
Onfaloplastia: o retorno ao processo natural
ABSTRACT
INTRODUCTION: Since the beginning of modern abdominoplasty, plastic surgeons have fixed their attention on the aesthetic aspect of the umbilicus. Reports show the efforts made to recreate a natural looking belly button and several techniques have been described, published, and put to use by surgeons. The author, imitating the course of action of the navel's natural healing process of a newborn child, presents another perspective in this surgical field.
METHOD: Results were collected between year 2008 to 2012, with patients ranging from 19 to 52 years of age, making a total 103 patients who were submitted to abdominoplasty and navel reconstruction under the technique proposed in this article. After the abdominal skin excess resection and rectiplication, the skin flap is correctly positioned, and a 2 cm vertical incision on the skin flap is performed to fit the new umbilicus position. Afterward a knot is made around the stalk and the extremity of the umbilicus is amputated. Finally the umbilicus is fixated in four cardinals points to the dermis of the skin incision with buried stitches and a secondary healing process begins. After about three weeks of postoperative period, the surgery concludes with the desired natural anatomic effect.
RESULTS: The umbilical shape and scar had a natural, clean aspect, leaving aside the common stigmata usually found after abdominoplasty such as noticeable scar, widening, stenotic appearance, etc.
CONCLUSION: The easy procedures and the final long-term youthful aspect of the umbilicus, make it suitable for the abdominoplasties armamentarium.
Keywords: Umbilicoplasty; Neo-omphaloplasty; Abdominoplasty.
RESUMO
INTRODUÇÃO: Desde do início da abdominoplastia moderna, os cirurgiões têm focado sua atenção na estética do umbigo. Relatos mostram os esforços realizados para recriar um aspecto natural do umbigo, sendo que diversas técnicas têm sido descritas, publicadas, e utilizadas pelos cirurgiões. Este estudo, imitando o processo de cicatrização natural do umbigo de um recém-nascido, apresenta outra perspectiva em relação a essa abordagem cirúrgica.
MÉTODO: Os dados foram coletados entre 2008 e 2012. Nosso estudo incluíu 103 pacientes, idade variando de 19 a 52 anos, submetidos a abdominosplastia e reconstrução do umbigo por meio da técnica imitando o processo de cicatrização natural do umbigo. Após ressecção do excesso de pele do abdome e replicação, o retalho é posicionado corretamente, e uma incisão vertical de 2cm é realizado no retalho para acomodar a nova posição do umbigo. Após um nó feito ao redor da pedúnculo a extremidade do umbigo é amputada. Finalmente, o umbigo é fixado nos quatro pontos cardinais da derme com sutura intradérmica, portanto, iniciando processo secundário de cicatrização. Em cerca de três semanas no período pós-operatório, a cirurgia é concluída e o efeito anatômico natural desejado é alcançado.
CONCLUSION: A facilidade para realizar o procedimento e o aspecto final jovial do umbigo ao longo prazo torna o procedimento apropriado para as abdominoplastias.
Palavras-chave: Umbilicoplastia; Neo-onfaloplastia; Abdominoplastia.
The umbilicus is the only natural scar in the body that is eulogized by all. In some cultures it is even considered a sexually appealing spot1, while in others a metaphoric symbol of personal independence. Its absence and/or distortions may call attention to it in a negative way.
Modern abdominoplasty, setting aside all technical details, determines the umbilicus to be positioned at the same level of the superior iliac crests to obtain an aesthetical aspect2. In an attempt to hide the scar3,4, despite the good results, there are also limited results and even unacceptable ones that can be observed such as hypertrophic scars, stenosis, widening, and perceptibly different skin color. On the other hand, scarless techniques5-7 may also have its defaults and present an unnatural skin tone continuity, or furthermore in long term postop, the intended navel indentation can lose depth resulting in a flattened appearance.
Trying to find a solution, the author observed the course of action of the umbilici healing process in newborns. During the first week after birth, the umbilicus mummifies and usually between the seventh and tenth day, it falls off leaving behind a small raw surface. Finally, by the end of the second week the navel's wound is completely healed and retracted. So by recreating the normal process of the umbilici scar formation of newborns, was created this neo omphaloplasty technique as an alternative procedure.
METHODS
From June 2008 until January 2012, 99 patients were submitted to abdominoplasties with neo omphaloplasty and the other four cases were of secondary omphaloplasty on patients who had prior undergone other techniques, making a total of 103 cases. The patients ranged from 19 to 52 years of age. The instance of this study was to follow the umbilical evolution for at least a year postoperative.
The process started with a single vertical incision on the abdominal flap, attaching it's borders to the umbilical stalk. We noticed that although we got an acceptable navel's depth, the scar retraction at the central portion ended up with a narrowed appearance. The results improved attaching together the skin, the umbilical stalk and the rectus abdominal fascia. The retraction of the central core gives natural aspect to the umbilicus after three weeks of secondary healing process.
SURGICAL TECHNIQUE
The umbilicaplasty is performed after the routine steps for abdominoplasty, through low pubic transversal incision, including the recti muscles plication, when necessary. Next we proceed to the skin excess resection; The abdominal skin flap and the pubis skin edge midline are provisionally sutured together and the new navel's position is located8-10. Routinely it is performed with the fingertip placed on the top of the umbilical stalk. At its projection, a vertical 2 cm long skin incision is performed at the skin flap, followed by a cylinder of subcutaneous tissue resection. Leaving a defatted area around the incision, helps to form a dimpled spot11. With the abdominal skin flap everted, the umbilical stalk is tied around its pedicle with a 2 - 0 silk, one centimeter above its implantation and the distal portion is resected (Figure 1, 2 and 3).
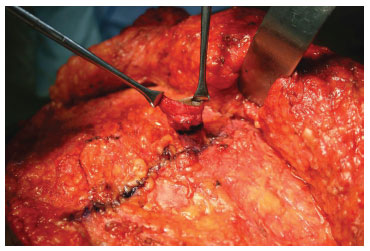
Figure 1. A horizontal line is marked with ink at about one centimeter from de insertion of the umbilical stalk.
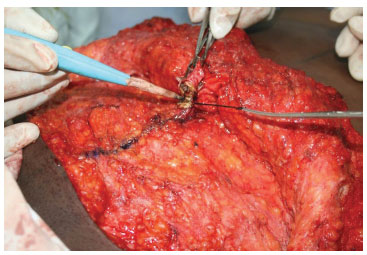
Figure 2. The stalk is tightly tied with 2-0 silk suture.
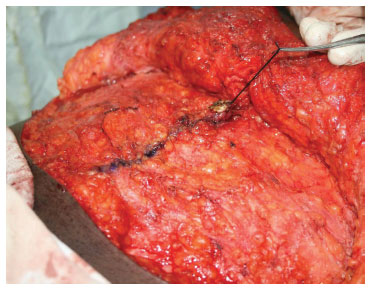
Figure 3. Ablation of the umbilical stalk above the loop.
Using long lasting absorbable sutures, four knots in the cardinal sides of the umbilical stalk, are sewed to the abdominal flap as follows: (i) A stitch at 12 and 6 hours bite the dermal extremities of the skin incision and the the umbilical stalk (Figure 4). (ii) In each side of the incision's lateral borders, at 3 and 9 hours, the stitch bites the dermis, fascia, and the umbilical stalk12. When tightened, a natural umbilical depth occurs. In specific cases where the patient does not need a complete rectus abdominal fascia plication, the navel's depth is obtained by plicating the periumbilical fascia vertically13.
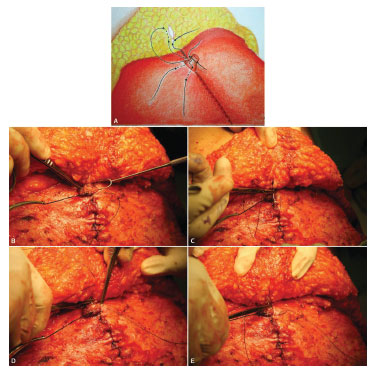
Figure 4. (A-E) Schematic and close up aspects how the umbilical stalk is fixed at the points 6:00h; 12:00h; 3:00h; 9:00h o'clock and at the 03.00 and 09.00 o'clock at the skin flap incision for its new position.
POSTOPERATIVE CARES
A gauze pad with ointment is applied for two days. After two postoperative days, the umbilicus' raw flesh remains exposed. The umbilical stalk should remain dry and disinfected daily with alcohol only. By the end of the second or third postoperative week, the stalk above the loop suture mummifies, necroses, and falls off (Figure 5A, B, C).

Figure 5. (A) Mummified umbilical stalk. (B) The scab eliminated with the raw surface exposed. (C) Healing process after three weeks.
As happens with the newborn's umbilicus, it begins the process of healing. The remaining stalk suffers retraction and some degree of contraction. Consequently, the healed navel has a completely natural appearance, which in many cases can almost be indistinguishable from the non-operated one.
RESULTS
The author found that the umbilici were reproduced without the well-known stigmata of abdominoplasties such as a noticeable scar, widening, stenosis or unmatching skin tone.
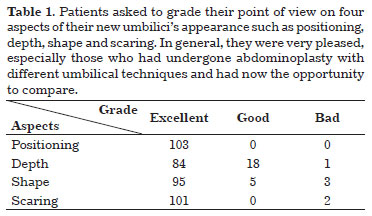
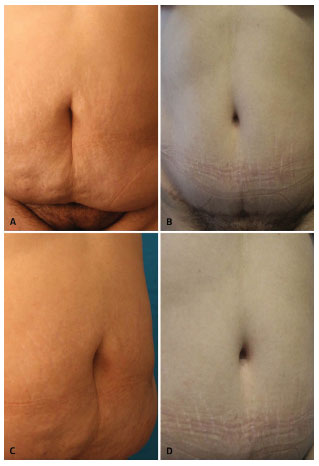
Patients in general were very pleased since some of them had the opportunity to compare their postoperative navel with that of friends who also got tummy tuck with another umbilical technique. Patients as seen in Table 1 graded four aspects of their umbilicus. They were extremely impressed with the superior quality of their result and expressed great satisfaction with the method (Cases 1, 2, 3, 4).

Case 1. (A-D) 46 year old female patient pre and two years postoperative period.
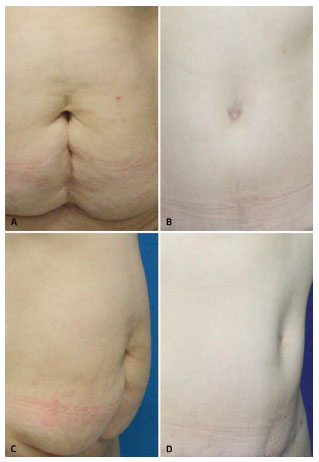
Case 2. (A-D) 38 year old female patient pre and two years postop.
Case 3. (A-D) 47-year-old patient pre and eleven months postoperative period.
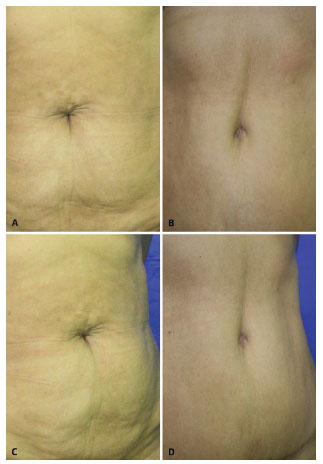
Case 4. (A-D) 56-year-old patient pre and eighteen months postoperative period.
COMPLICATIONS
One major complication related, not directly with the umbilicus, but to the abdominoplasty itself occurred. It consisted in a triangular area of abdominal skin necrosis having its base at the lower pubic suture and its apex at the umbilical level.
Reconstruction of the abdominal wall was performed with advanced local flaps; Nevertheless, the umbilical depth was lost. A few minor intercurrences, no complications, were related to delayed falling off or healing of the umbilical stalk. Patients expressed their worries for what they considered as a yellowish ugly appearance of their navel. Once patients got an explanation about what was going on, they were appeased.
DISCUSSION
Aspects such as positioning, shape, and depth are all involved in aesthetic omphaloplasty, but it has been the scar that has usually deserved the surgeons' full attention. This is why the great majority of techniques in omphaloplasty attempt to conceal or avoid the periumbilical scar, that remains exposed.
Some authors in an attempt to hide the scar, suture the umbilical skin to the rectus fascia, or use a single Y type of incision3, while others4 use a vertical incision at the abdominal skin flap. In literature, another method is registered14, where two small skin triangles are resected along with a fat cylinder underneath. The edges are then sutured to the underlying fascia to create a vertical slit appearance for the umbilicus. Deepithelialization of the skin and its incision at the midline of the neoumbilical position creates two dermal flaps that are then sutured down to the abdominal fascia, making a similar periumbilical concavity for the navel with inconspicuous scar through tensionfree closure15. Another scarless technique6 lifts and everts the skin's abdominal flap and an area of about 6 to 7 cm diameter is defatted from underneath the new navel site. Next, a purse string suture is stitched to the dermis at the margin of the defatted circle and tightened up to shrink its previous diameter to 2 cm, imitating the umbilical aspect. The preserved, original umbilicus skin is then deepithelialized, maintaining the cone shape into which the skin crater done by the purse string is then sutured.
In cases of absence or necrosis of the navel16, a two-centimeter transversal incision is performed on the abdominal flap and area around the new position is defatted. Stitches around the edge are applied to the fascia and the open area heals by second intention. This procedure is different from the one presented here. This technique preserves part of the umbilical stalk, gives natural skin color aspect and preserves the umbilical sensation.
The method presented in this article aims mostly to give back the navel natural appearance, preserving good positioning, shape, depth and normal scar. Not having the umbilicus' stigma of abdominoplasty is highly significant to the patient's self-esteem.
CONCLUSIONS
The umbilicus, as the central aesthetic attraction in the abdomen, has gained special attention in the process of cosmetic and reconstructive abdominoplasty. Navel loss or deformity may be a source of psychological distress for many patients17. We believe this statement to be true, especially among the younger ones.
A youthful and appealing umbilicus has been described as small, vertically oriented, and deep with a superior hooding4,18,19. All these aspects are related to wound contraction, growing process, periumbilical fat deposits, and gravity respectively.
Nevertheless, miscellaneous varieties of navel shapes are found in the general population. Imitating the natural umbilical scar formation allows the innate development of the above-mentioned characteristics, also marking in our hands a significant improvement over past procedures.
Based on the results and quality obtained, we believe this contribution to be a preferred option for future abdominoplasties.
REFERENCES
1. Pardo Mateu L, Chamorro Hernandez JJ. Neoumbilicoplasty through a purse-string suture of three defatted flaps. Aesthetic Plast Surg. 1997;21(5):349-51. http://dx.doi.org/10.1007/s002669900136. PMid:9299004
2. Abhyankar SV, Rajguru AG, Patil PA. Anatomical localization of the umbilicus: an Indian study. Plast Reconstr Surg. 2006;117(4):1153-7. http://dx.doi.org/10.1097/01.prs.0000204793.70787.42. PMid:16582780
3. Massiha H, Montegut W, Phillips R. A method of reconstructing a natural-looking umbilicus in abdominoplasty. Ann Plast Surg. 1997;38(3):228-31. http://dx.doi.org/10.1097/00000637-199703000-00007. PMid:9088459
4. Lee MJ, Mustoe TA. Simplified technique for creating a youthful umbilicus in abdominoplasty. Plast Reconstr Surg. 2002;109(6):2136-40. http://dx.doi.org/10.1097/00006534-200205000-00054. PMid:11994626
5. Baack BR, Anson G, Nachbar JM, White DJ. Umbilicoplasty: the construction of a new umbilicus and correction of umbilical stenosis without external scars. Plast Reconstr Surg. 1996;97(1):227-32. http://dx.doi.org/10.1097/00006534-199601000-00038. PMid:8532784
6. Schoeller T, Wechselberger G, Otto A, Rainer C, Schwabegger A, Lille S, et al. New technique for scarless umbilical reinsertion in abdominoplasty procedures. Plast Reconstr Surg. 1998;102(5):1720-3. http://dx.doi.org/10.1097/00006534-199810000-00064. PMid:9774037
7. Barreto L, Londoño G, Salazar D. Neoumbilicoplastia: técnica de tres suturas: Descripción de uma técnica quirúrgica. Rev Soc Col Cir Plast. 2008;14(1):43-58.
8. Kurul S, Uzunismail A. A simple technique to determine the future location of the umbilicus in abdominoplasty. Plast Reconstr Surg. 1997;100(3):753-4. http://dx.doi.org/10.1097/00006534-199709000-00035. PMid:9283578
9. Hoffman S. A simple technique for locating the umbilicus in abdominoplasty. Plast Reconstr Surg. 1989;83(3):537-8. http://dx.doi.org/10.1097/00006534-198903000-00026. PMid:2919207
10. Pitchon L, Rubinstein C. A (more) simple technique for locating the umbilicus in abdominoplasty. Aust N Z J Surg. 1993;63(1):42-3. http://dx.doi.org/10.1111/j.1445-2197.1993.tb00032.x. PMid:8466460
11. Juri J, Juri C, Raiden G. Reconstruction of the umbilicus in abdominoplasty. Plast Reconstr Surg. 1979;63(4):580-2. http://dx.doi.org/10.1097/00006534-197904000-00032. PMid:424470
12. Niranjan NS, Staiano JJ. An anatomical method for re-siting the umbilicus. Plast Reconstr Surg. 2004;113(7):2194-8. http://dx.doi.org/10.1097/01.PRS.0000122547.56709.08. PMid:15253213
13. Mazzocchi M, Dessy LA, Figus A. A versatile technique for repositioning of the umbilicus in abdominoplasty. Plast Reconstr Surg. 2008;121(5):357e-8e. http://dx.doi.org/10.1097/PRS.0b013e31816b11cd. PMid:18453967
14. Lim TC, Tan WTL. Managing the umbilicus during abdominoplasty. Plast Reconstr Surg. 1996;98(6):1113-8. http://dx.doi.org/10.1097/00006534-199611000-00036. PMid:8911488
15. Rozen SM, Redett R. The two-dermal-flap umbilical transposition: a natural and aesthetic umbilicus after abdominoplasty. Plast Reconstr Surg. 2007;119(7):2255-62. http://dx.doi.org/10.1097/01.prs.0000261037.69256.3e. PMid:17519729
16. Baroudi R. Body sculpturing. Clin Plast Surg. 1984;11(3):419-43. PMid:6147222.
17. Park S, Hata Y, Ito O, Tokioka K, Kagawa K. Umbilical reconstruction after repair of omphalocele and gastroschisis. Plast Reconstr Surg. 1999;104(1):204-7. http://dx.doi.org/10.1097/00006534-199907000-00032. PMid:10597697
18. Craig SB, Faller MS, Puckett CL. In search of the ideal female umbilicus. Plast Reconstr Surg. 2000;105(1):389-92. http://dx.doi.org/10.1097/00006534-200001000-00062. PMid:10627008
19. Akbaş H, Güneren E, Eroğlu L, Uysal OA. Natural-looking umbilicus as an important part of abdominoplasty. Aesthetic Plast Surg. 2003;27(2):139-42. http://dx.doi.org/10.1007/s00266-003-0109-7. PMid:14629069
Former Member of the Brazilian Society of Plastic Surgery (SBCP), Member of the Colombian Society of Plastic Surgery, Cali, Valle, Colombia.
Institution: This study was performed in private settings, in Cali, Valle, Colombia.
Corresponding author:
William Libardo Murillo
Calle 5D # 38 A 35, consultorio 816
Cali, Valle, Colombia
E-mail: williamurillo@gmail.com
Article received: February 27, 2014.
Article accepted: August 01, 2014.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket