



Ideas and Innovation - Year 2014 - Volume 29 -
Mucosal and local skin flap reconstruction for loss of substance in the cheek region
Associação de retalho mucoso e retalho cutâneo local na reconstrução de perda de substância em região da bochecha
ABSTRACT
The face is an important structure, because it is the most visible part of the body and contains delicate and complex elements that are essential for aesthetics and functionality. Facial reconstruction of areas with substantial substance loss remains a surgical challenge. There are several repair options, with corresponding advantages and disadvantages. We present a case of a patient with substance loss of the total thickness of the cheek region who received mucosal and local skin flap surgery, with good results and functional preservation.
Keywords: Reconstruction; Face; Cheek; Surgical flaps.
RESUMO
A face representa uma estrutura importante nos seres humanos, devido a ser a parte mais visível do corpo e conter elementos delicados e complexos, que são essenci ais em termos de beleza e funcionalidade. As reconstruções faciais, em áreas de grandes perdas de substâncias, permanecem como um desafio para os cirurgiões. Apresentam várias opções de reparo, todas com suas vantagens e desvantagens. Mostramos o caso de um paciente apresentando perda de substância de espessura total em região de bochecha, que foi submetido à associação de retalho mucoso e retalho cutâneo local, apresentando bom resultado e preservação funcional.
Palavras-chave: Reconstrução; Face; Bochecha; Retalhos cirúrgicos.
The face is an important structure because it is the most visible part of the body and contains delicate and complex elements that are essential for aesthetics and functionality1.
From an aesthetic point of view, the cheek area can be divided into three units according to location: suborbital, preauricular, and buccomandibular2. The buccomandibular region is comprised of four layers: the skin, subcutaneous region, superficial musculoaponeurotic system (SMAS), and oral mucosa, that are reconstructed in multiple surgical planes.
Many forms of reconstruction have been described, from the superficial layer to the oral mucosa.
Primary closure, partial and full skin grafts, local flaps (cutaneous and myocutaneous), free flaps, and tissue expansion have been described as options for reconstruction of the superficial plane1-10.
Mucosal defects in the oral cavity resulting from tumor resections or acute or chronic infectious processes may cause significant functional and aesthetic deficits, but can be reconstructed with primary closure, closure by secondary intention with mucosalization, skin grafting, tongue flap, local skin flaps, and free flaps7,9.
METHODS
A 33-year-old male mulatto university student from Pirapora, Minas Gerais, was single, HIV-positive, and had a history of tonsillitis six years prior, which evolved to bilateral facial cellulitis (oral region). He was initially treated with penicillin, but had an allergic reaction and remained hospitalized for (unnamed) antibiotic therapy. The cellulitis evolved to abscess and local necrosis. The left side closed spontaneously, but the right side had a large area with total thickness loss of substance. A graft was attempted at the time without satisfactory results.
On examination, we found significant bilateral facial atrophy and extensive areas with loss of substance on the right side, as shown in Figures 1 and 2. During the previous six years, the patient used occlusive dressings, changing them several times daily and whenever he ate.

Figure 1. Previous view showing important bilateral hypotrophy and area of complex susbtance losses on the right.

Figure 2. Lateral view showing significant hypotrophy and area with complete substance loss on the right side.
His infectious disease was monitored frequently, he correctly used his prescribed antiretroviral therapy, and did not have contraindications to surgery.
RESULTS
Surgical procedure
The patient was placed under general anesthesia, with skin and oral cavity antisepsis therapy. First, an incision was made on the border between the skin and oral mucosa regions (mucosalization), with dissection of the mucosal plane, to form two mucosal flaps. Sutures were inserted two planes to preserve the mucosal layer in the intraoral region (Figures 3, 4, and 5).

Figure 3. Image showing detachment of the mucosal area.

Figure 4. Image showing the end stage of making a mucosal flap.

Figure 5. Image showing the suturing of two planes of the mucosal flap.
Next was dissection of the skin flap in the supra-SMAS plane of the third middle facial region to fabricate a lateral transposition flap and closing by planes, followed by site dressing (Figures 6 and 7).

Figure 6. Making local skin flap.

Figure 7. Final appearance after surgery. Note the suction drain.
After surgery, the patient underwent antibiotic treatment with clindamycin as well as vacuum aspiration drainage.
On the seventh day after the procedure, the patient presented with a small skin flap with purulent local secretion at the edges. Ciprofloxacin and metronidazole antibiotics were prescribed for seven days, with good performance and closure by secondary intention. Thus, the procedure provided satisfactory results, with no salivary fistula, preservation of masticatory function, and maintenance-free dressings (Figures 8, 9, and10).

Figure 8. View at the three month post-operative follow-up.

Figure 9. Right profile view at the three month postoperative follow-up.
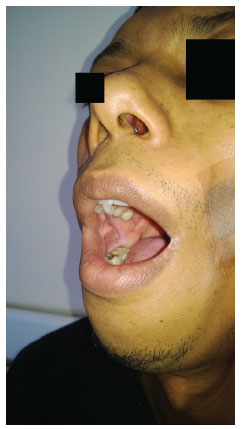
Figure 10. Intraoral view showing the integral mucous membranes.
DISCUSSION
Facial reconstruction of areas with large loss of substance remains a challenge for surgeons1,3. There are several repair options with corresponding advantages and disadvantages1.
Skin grafts are a simple option with little associated morbidity, but the grafts are often a different color and thickness compared to the receiving region, and consequently have generally unsatisfactory aesthetic results1,3,6.
Free flaps are an excellent choice, but the procedure requires appropriate structure and staff with microsurgery experience. They may present complications such as infection, thrombosis, and flap loss3,4,8,9.
Local flaps, as presented here, are often a good choice because they offer matching skin color and similar texture, and have reduced risks for patients with comorbidities; however, they have limited application for correcting extensive damage. Examples of commonly used flaps and techniques include Esser flaps, Blascowicz, Ferris Smith, Mustardé, Converse, Stark, Juri and Juri, Zide and Schruder, and Kroll6,11,12.
Proper oral function and aesthetic results are the goal of oral cavity reconstruction, and skin grafts, local skin flaps, and free flaps are options for reconstruction of the oral mucosa. Tongue flaps are also an option, but may result in chewing and swallowing changes7,9.
Reconstruction of large facial substance loss is a surgical challenge and the combined use mucosal and local skin flaps is a good option for reconstruction of the total thickness of the cheek region, offering low morbidity and similar tissue.
REFERENCES
1. Motamed S, Fadaee-Naeeni A. Reconstruction of the cheek, moustache, and beard by transferring an expanded cervical flap. Arch Iran Med. 2008;11(2):221-3. PMid:18298305.
2. Heller L, Cole P, Kaufman Y. Cheek reconstruction: current concepts in managing facial soft tissue loss. Semin Plast Surg. 2008;22(4):294-305. http://dx.doi.org/10.1055/s-0028-1095888. PMid:20567705
3. Saito N, Tsutsumida A, Furukawa H, Sekido M, Oyama A, Funayama E, et al. Reconstructive considerations in the treatment of soft tissue sarcomas of the cheek. Acta Otorhinolaryngol Ital. 2010;30(2):103-6. PMid:20559481.
4. Colletti G, Autelitano L, Tewfik K, Rabbiosi D, Biglioli F. Autonomized flaps in secondary head and neck reconstructions. Acta Otorhinolaryngol Ital. 2012;32(5):329-35. PMid:23326014.
5. Fenton CC, Kertesz T, Baker G, Sándor GKB. Necrotizing fasciitis of the face: a rare but dangerous complication of dental infection. J Can Dent Assoc. 2004;70(9):611-5. PMid:15473945.
6. Liu FY, Xu ZF, Li P, Sun CF, Li RW, Ge SF, et al. The versatile application of cervicofacial and cervicothoracic rotation flaps in head and neck surgery. World J Surg Oncol. 2011;9(1):135. http://dx.doi.org/10.1186/1477-7819-9-135. PMid:22018437
7. Eckardt AM, Kokemüller H, Tavassol F, Gellrich NC. Reconstruction of oral mucosal defects using the nasolabial flap: clinical experience with 22 patients. Head Neck Oncol. 2011;3(1):28. http://dx.doi.org/10.1186/1758-3284-3-28. PMid:21605443
8. Reis J, Amarante J, Malheiro E, Santa-Comba A, Costa-Ferreira A, Barroso ML. Retalhos livres na reconstrução de cabeça e pescoço. Acta Med Port. 1998;11(2):103-10. PMid:9567406.
9. Denewer AT, Steet AE, Mohamed OH, Aly OF. Locally advanced cheek carcinoma; radical surgery and reconstruction of though and through defects. Journal os the Egyptian Nat. J Egypt Natl Canc Inst. 2006;18(2):141-6. PMid:17496939.
10. White CP, Rosen N, Muhn CY. The usefulness of the bilobed flap for lateral cheek defects. Can J Plast Surg. 2012;20(1):e19-21. PMid:23598770.
11. Mehrara BJ. Reconstrução das bochechas. In: Thorne CH, Beasley RW, Aston SJ, Bartlett SP, Gurtner GC, Spear SL. Grabb e Smith: cirurgia plástica. 6. ed. Rio de Janeiro: Guanabara Koogan; 2007. p. 366-79.
12. Beirigo MF, D'Alessandro GS, Oksman D, Nunes TR, Busnardo FF, Pinto WS. Reconstrução da porção medial da pálpebra inferior com retalho de Imre. Rev Bras Cir Plást. 2009;24(4):569-72.
1. Resident Doctor of Plastic Surgery of Hospital das Clínicas of Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, MG, Brazil
2. Full Member of the Brazilian Society of Plastic Surgery (BSPS), Preceptor of the Service of Plastic Surgery of Hospital das Clínicas of Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, MG, Brazil
Institution: Work conducted at the Clinical Hospital of the Federal University of Minas Gerais, Belo Horizonte, MG, Brazil.
Corresponding author:
Jose Mauro de Oliveira Squarisi
Serviço de Cirurgia Plástica do Hospital das Clínicas da Universidade Federal de Minas Gerais
Avenida Professor Alfredo Balena, 110 - Santa Efigênia
Belo Horizonte, MG, Brazil CEP 30130-100
E-mail: josemauroeu@yahoo.com.br
Article received: December 30, 2013.
Article accepted: August 3, 2014.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket