



Original Article - Year 2014 - Volume 29 -
Cost analysis in patients admitted to the Santa Casa Misericórdia de Campo Grande, treated with and without the aid of hyperbaric oxygen therapy
Análise dos custos de pacientes internados na Santa Casa Misericórdia de Campo Grande, tratados com e sem auxílio de oxigenoterapia hiperbárica
ABSTRACT
INTRODUCTION: Burns are among the leading external causes of death in Brazil, generating huge costs and having physical, psychological, and social consequences. The objective of this study was to compare two groups of burn patients, i.e., those with and those without adjuvant treatment with hyperbaric oxygen (HBO) therapy and to perform a cost analysis.
METHODS: A retrospective study was carried out between 2011 and 2013, comparing 20 patients with moderate to severe burns who were hospitalized at the Santa Casa de Misericórdia de Campo Grande and treated with HBO (group I) and 22 patients treated without HBO (group II).
RESULTS: Most of the patients, i.e., 24 (57.1%), were male. Flammable product was the most frequent etiologic agent in both groups, accounting for 56.6% of the burn cases. The average age of group I patients was of 26.6 years and that of group II was of 23.3 years, with a prevalence (50.4%) of those aged between 13 and 35 years. The average final cost per patient was R$17,292.00 for group I and R$25,360 for group II (p = 0.028).
CONCLUSION: We conclude that, in our service, patients presenting moderate and severe burns and treated with HBO therapy underwent a lower number of surgical procedures, e.g., grafts and debridement that allowed reduced hospitalization time and led to significant savings in hospital costs.
Keywords: Burn; Treatment; Hyperbaric.
RESUMO
INTRODUÇÃO: As queimaduras estão entre as principais causas externas de morte no Brasil, geram enormes gastos financeiros e são responsáveis por sequelas físicas, psicológicas e sociais. O Objetivo deste estudo foi comparar os dois grupos de pacientes queimados com e sem tratamento coadjuvante com Oxigenoterapia Hiperbárica, assim como, realizar uma análise dos custos.
MÉTODOS: Foi realizado estudo retrospectivo, período de 2011 a 2013, selecionando, 20 pacientes com queimaduras moderadas e graves, internados na Santa Casa de Misericórdia de Campo Grande, tratados com auxílio de OHB (grupo I) e 22 pacientes sem auxílio de OHB (grupo II).
RESULTADOS: A maioria dos pacientes pertencia ao sexo masculino, 24 pacientes (57,1%). O agente etiológico mais frequente nos dois grupos foi produtos inflamáveis com 56,6% dos casos. A idade média do grupo I foi de 26,6 e a do grupo II 23,3, predominando a faixa etária entre 13 e 35 anos 50,4% dos pacientes. Custo médio final por paciente do Grupo I foi R$17.292,00, e grupo II R$25.360 (p=0,028).
CONCLUSÃO: Concluímos que, no nosso serviço, o grupo de pacientes com queimaduras moderadas e graves tratados com auxílio da Oxigenioterapia Hiperbárica teve um menor número de procedimentos cirúrgicos, como enxertos e desbridamento, e menor tempo de internação, levando a uma economia importante dos gastos hospitalares.
Palavras-chave: Queimado; Tratamento; Hiperbárica.
Burns are among the leading external causes of death in Brazil, generating large costs and having physical, psychological, and social consequences1.
Gaining knowledge in epidemiology is important in all areas of medical expertise, to support the evaluation and organization of treatment programs and prevention campaigns that present burns as severe accidents that can be avoided through the application of epidemiological principles, besides conducting awareness campaigns and educational programs2,3.
Data from the Brazilian Society of Burns show that, in Brazil, there are 1 million cases of burns each year, of which 200,000 are treated in emergency services. Of these, 40,000 require hospitalization and about 2500 result in death, directly or indirectly due to the injuries, which entail a high social and economic impact. Several methods have been used to reduce the costs associated with burn injuries; one of such methods is hyperbaric oxygen (HBO) therapy4,5.
OBJECTIVE
The aim of this study was to compare the final costs of burn patients treated with and without HBO therapy and to perform a cost analysis.
METHODS
A retrospective study was carried out between 2011 and 2013, including patients presenting moderate to severe burn who were admitted to the Santa Casa de Misericórdia of Campo Grande. Of these patients, 23 were treated with HBO (group I) and 23 were treated without HBO (group II). For the HBO therapy, the protocol included only patients with severe burns (second-degree burns exceeding 20% of the body surface area [BSA]; third-degree burns exceeding 10% of the BSA; electrical burns; or burns in delicate areas such as the face, neck, hands, feet, perineum, armpits, groin, and popliteal region) and moderate burns (second-degree burns involving between 10% and 20% of the BSA, or third-degree burns involving between 3% and 10% of the BSA). All patients needed to be hemodynamically stable to receive the treatment. Each session was performed at 2.5 atm for a period of 120 min, once a day. Throughout the procedure, patients were followed by a hyperbaric physician. Variables such as sex, age, etiology, and severity of the burn were evaluated using the chi-square test. The comparison between patients treated or not treated with HBO in relation to the number of sessions, debridement, grafts, dressings, and final costs was carried out using Student's t test. Statistical analysis was performed by using SPSS software, version 17.0, with the level of significance set at 5%.
RESULTS
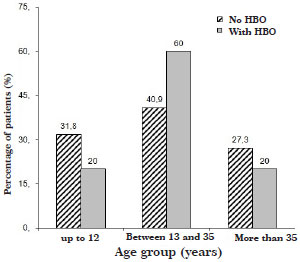
Most of the patients were male, among whom 56.5% and 60.9% were treated with and without HBO, respectively (Graph 1 and Table 1).
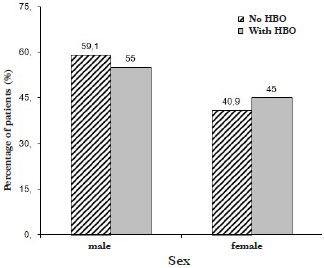
Graph 1. Distribution of patients treated with and without the aid of hyperbaric oxygen (HBO) therapy, according to sex.
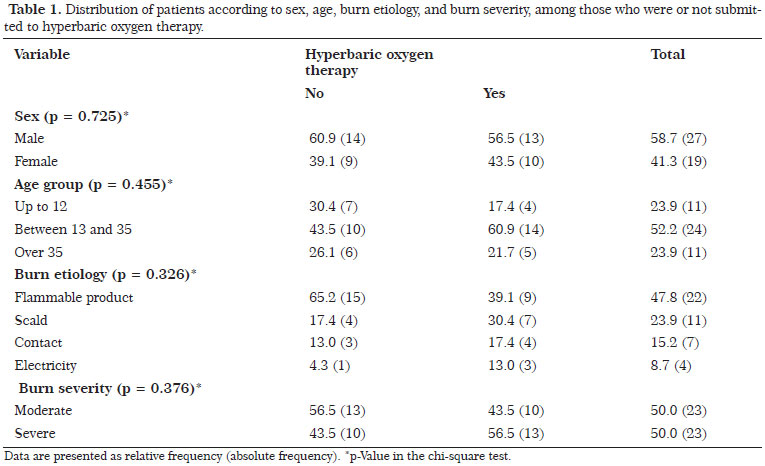
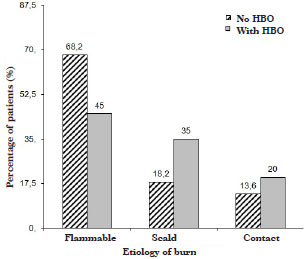
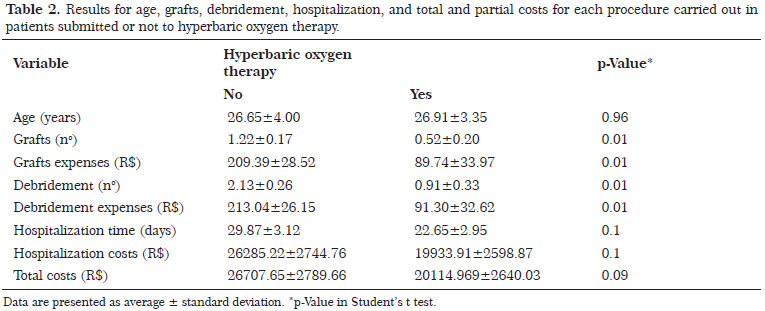
A flammable product was the most frequent etiologic agent in both groups, with 39.1% and 65.2% of these patients treated with and without HBO, respectively (Graph 2 and Table 1). The average age of group I patients was of 27.9 years, and that of group II patients was of 26.7 years. There was a prevalence of patients aged between 13 and 35 years-accounting for 60.9% of group I and 43.5% of group II (Graph 3 and Table 1). The classifications of burns presented by group I patients were moderate in 10 and severe in 13. In group II, 13 burns were moderate and 10 were severe (Graph 4 and Table 1). The number of debridement performed was 21 in group I and 49 in group II. The number of graft procedures carried out in was 12 in group I and 28 in group II. The average hospitalization time was 23.3 days in group I and 29.8 days in group II. The average cost for the grafts in groups I and II was 89.74 and 209.39 reals, respectively, whereas the average cost for debridement procedures was 91.30 and 213.04 reals, respectively. The average cost of hospitalization was 19,933.91 reals in group I and 26,285.22 reals in group II. The final average costs per patient 20,114 reals in group I and 26,707 reals in group II (p=0.093). The number of HBO sessions in group I varied from 2 to 20, with an average of 11.04 sessions (Table 2).
Graph 2. Distribution of patients treated with and without the aid of hyperbaric oxygen (HBO) therapy, according to burn etiology.
Graph 3. Distribution of patients treated with and without the aid of hyperbaric oxygen (HBO) therapy, according to age group.
DISCUSSION
Burn is a complex and dynamic lesion characterized by a coagulation region surrounded by a stasis zone, which is, in turn, surrounded by an erythema area. This coagulation region can extend up to 10 times in the first 48 h, and can then rapidly evolve into ischemic necrosis. Hemoconcentration and microthrombosis occur in postcapillary venules and decrease or suppress the microcirculation flow. This is associated with increased capillary permeability, promoting plasma transudation into the injured tissues and leading to a rapid edema formation and progression to ischemic necrosis6. Changes in microcirculation in distant areas are also observed and are due to the action of vasoactive mediators, leading to edema of unburned tissues. This ischemic process is progressive and can extend the damage during the first days after trauma7. Prolonged thermal damage is due to the inability of surrounding tissues to provide the cells of the injured area with the oxygen and nutrient supply necessary to maintain their viability, thus leading to the progression of the lesion to the deeper layers7.
The treatments of burns are aimed at reducing edema, preserving viable tissues around the burned area, increasing the body's defenses, and promoting wound healing. Therefore, HBO therapy is a complementary treatment to accelerate this process of tissue recovery8.
Adjuvant treatment with HBO therapy should be started as early as possible after the injury for initial resuscitation. This treatment can be carried out two times, lasting 90 min each, at 2.5 atm, starting in the first 24 h and continued until the wound is epithelialized. Children should be treated for 45 min. In large burns involving 40% or more of the BSA, the treatment may be longer than 15 days with an average between 20 and 30 sessions, but not exceeding 40-50 sessions, except in special cases1.
The use of HBO therapy as an aid in burns treatment has shown several benefits such as:
1. Decrease in erythema, edema formation, and burn exudation9,10;
2. Improvement in perfusion and tissue oxygenation10,11, with a significant increase in tissue pO2, which can remain high after interrupting the HBO therapy12;
3. Early reversal of capillary stasis with decreased progression of thermal injury and more rapid epithelialization of the wound11,12;
4. Improvement of the immune response by increasing the activity of macrophages12;
5. Decreased time of wound healing, with decreased rates of infections of the burned area12.
HBO therapy also restores depleted levels of ADP, reduces high levels of lactate and phosphorylases, maintains the integrity of the microcirculation, and provides the substrates necessary to maintain the vitality of tissues surrounding the burn area, thus preventing the progression of the lesion13. These effects reduce the need for performing graft procedures in addition to diminishing the hospitalization time, infection rate, mortality, and hospital costs8, as confirmed in this study in which a significant reduction in grafts and debridement requirement as well as in final hospital costs was observed.
In this study, most of the patients were male, aged between 13 and 35 years-an age group representing the greatest production force and manpower, according to other studies published in the literature14-16. In the article "Burn patients evaluated for hyperbaric oxygen therapy," by Marra et al.14, most of the patients were male (75%), and the average age of groups I and II was 38.1 and 52.8 years, respectively. Concerning the etiologic agent, we confirmed the data reported in the literature that highlight flammable agents, e.g., alcohol, gasoline, and thinner, as the main etiologic factor; this etiology accounts for 39.1% and 65.2% of the patients treated with and without HBO, respectively, according to the studies by Macedo et al.15 and Leão et al.16.
Several clinical series demonstrated a more rapid recovery, reduced need for fluids, surgeries, and hospital stay, as well as reduced mortality and hospitalization costs. In 1974, Hart et al.2 reported a series of randomized cases showing a reduced need for fluids, fast wound healing, and reduced mortality when treated patients were compared to controls. Cianci et al.1, in a comparative study on patients presenting burns involving between 18% and 39% of the BSA, showed a significant reduction in hospitalization time, from 33 to 20.8 days (p=0.012), when HBO was added to the treatment. In this study, a reduction in the average hospitalization time was also observed, from 29.8 days in the group treated without HBO to 23.3 days in the group treated with HBO. A significant reduction in hospital costs was also observed, from 26,707 reals to 20,114 reals when HBO was added as adjuvant treatment (p=0.093). Cianci et al.8, in another study on patients presenting burns involving between 40% and 80% of the BSA, observed a reduction from 8 to 3.7 (p=0.041) in the number of surgical interventions when HBO was added to the treatment. This confirms the results obtained in our study, in which we observed a decrease in the number of debridement from 49, in the group of patients treated without HBO, to 21, in the group of patients treated with HBO, thus saving 2800 reals. Similarly, the number of graft procedures also reduced, from 28 in the group of patients treated without HBO to 12 in those treated with HBO, which saved 1548 reals. The HBO costs in patients with this treatment as adjuvant therapy was included in the final cost calculated for patients of group I, with an average value of 264 reals per session. In both groups, the CTI costs were also added to the final costs.
CONCLUSION
We conclude that in our service, patients with moderate and severe burns who were treated with HBO therapy required a reduced number of surgeries, e.g., grafts and debridement. This treatment also resulted in reduced hospitalization time, thus leading to significant savings in hospital costs.
REFERENCES
1. Cianci P, Lueders HW, Lee H, Shapiro RL. Adjunctive hyperbaric oxygen reduces length of hospitalization in thermal burns. J Burn Care Rehabil. 1989;19:432-6.
2. Hart GB, O'Reilly RR, Broussard ND, Cave RH, Goodman D. Treatment of burns with hyperbaric oxygen. Surgery, Gynecol Obstet 1974;139:693-6.
3. Mélega JM. Cirurgia Plástica. 2 ed. Rio de Janeiro: Medsi 1992.
4. Ferreira E, Lucas R, Rossi LA, Andrade D. Treatment of the burned patient: a review of the literature. Rev Esc Enferm USP. 2003;37(1):44-51.
5. Kliemann JD, Lehugeur DS, Franche GLS, Seara SC. Acidentes por queimaduras em crianças: estudo epidemiológico. Rev HPS. 1990;36(1):36-41.
6. Boykin JV, Eriksson E, Pittman RN. In vivo microcirculation of a scalp and progression of postburn dermal ischemia. Plast Reconstr Surg. 1980; 66:191.
7. Arturson G. Pathophysiology of the burn wound. Ann Chir Gynaecol. 1980;69:178.
8. Cianci P, Lueders HW, Lee H, Shapiro RL, Sexton J, Williams C, Green B. Adjunctive hyperbaric oxygen reduces the need for surgery in 40-80% burns. J Hyper Med. 1988;3:97.
9. Niezgoda JA, Cianci P. The effect of hyperbaric oxygen therapy on a burn wound model in human volunteers. Plast Reconstr Surg. 1997;1620-25.
10. Gruber RAP, Brinkley B, Amatto JJ, Mendelson JA. Hyperbaric oxygen and pedicle flaps, skin, grafts, burns. Plast Reconstr Surg. 1970;45(1):24-30.
11. Kindwall EP, Gottlieb LJ, Larson DL. Hyperbaric oxygen therapy in plastic surgery. A review article. Plast Reconstr Surg. 1991;88(5):898.
12. Hohn DC, Mackay RD, Halliday B, Hunt TK. Effect of O2 tension on the microbiocidal functions of leukocytes in wound and in vitro. Surg Forum. 1976;27(62)18-20.
13. Nylander G. Tissue ischemia and hyperbaric oxygen treatment: an experimental study. Acta Chir Scand Suppl. 1986;533:1-109.
14. Marra A. et al. Burn patients evaluated for hyperbaric oxygen therapy. RBTI 2003;15(4):142-3.
15. Macedo JLS, Rosa SC. Estudo epidemiológico dos pacientes internados na Unidade de Queimados: Hospital Regional da Asa Norte, Brasília, 1992-1997. Bras Méd. 2000;37(3/4):87-92.
16. Leão CEG, et al. Epidemiologia das queimaduras no estado de Minas Gerais. Rev. Bras. Cir. Plást. 2011;26(4):573-7.
1. Plastic Surgery Resident
2. Preceptor Physician at the Plastic Surgery Service of the Santa Casa de Campo Grande-MS, a title conceived by BSPS and SBHM
3. Plastic Surgeon, Associate Member of BSPS
4. Plastic Surgery Resident
5. General Surgery - Plastic Surgery Resident at the da Santa Casa de Campo Grande - MS
6. Plastic Surgery Resident
7. Prof. Dr. at the Biological and Health Sciences Center of the Federal University of Mato Grosso do Sul
8. Plastic Surgery Resident
Institution: Santa Casa Misericórdia de Campo Grande.
Corresponding author:
Elson Taveira Adorno Filho
Rua São Paulo, 661 - Apto 90 - Ed. Manhhattan
Campo Grande, MS, Brazil Zip code: 79010-050
E-mail: elsonadorno@hotmail.com.br
Article submitted: January 7, 2014.
Article accepted: December 13, 2014.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket