



Case Report - Year 2014 - Volume 29 -
Treatment of congenital ptosis by using the Lester Jones technique
Tratamento de ptose palpebral congênita pela técnica de Lester Jones
ABSTRACT
INTRODUCTION: Palpebral ptosis or blepharoptosis is characterized by the dysfunction or inability of the patient to normally open the palpebral fissure. Usually, it is due to the involvement of the eyelid levator muscle. The congenital form occurs in 60%-70% of cases. In this study, we describe a case of moderate congenital palpebral ptosis in a 9-year-old patient who presented with a good eyelid levator muscle function in the left eye. The patient underwent surgical treatment with the Lester Jones technique, as indicated for cases of moderate ptosis, and achieved satisfactory aesthetic and functional results.
Keywords: Congenital Blepharoptosis; Eyelid levator muscle; Lester Jones.
RESUMO
INTRODUÇÃO: A ptose palpebral ou blefaroptose caracteriza-se pela disfunção, ou inabilidade do paciente em realizar a abertura da fenda palpebral de maneira normal. Geralmente é decorrente do acometimento do músculo levantador da pálpebra; a forma congênita ocorre em 60% a 70%. No presente trabalho é descrito um caso de ptose palpebral congênita moderada em uma paciente de nove anos, com boa função do músculo levantador da pálpebra, em olho esquerdo. A paciente foi submetida a tratamento cirúrgico pela técnica de Lester Jones, indicada nos casos de ptose de grau moderado, apresentando um resultado estético e funcional satisfatório.
Palavras-chave: Blefaroptose congênita; Músculo levantador da pálpebra; Lester Jones.
Palpebral ptosis or blepharoptosis is a deformity in which the course of the upper eyelid does not occur normally because of a congenital or acquired dysfunction of the upper eyelid levator muscle1. The congenital, bilateral, and simple forms correspond to 60%-70%, 25%, and approximately 75%-80%2 of all the cases2. Congenital ptosis can also be described as the drooping of the upper eyelid, in which the eyelid margin is situated below the level considered normal. This position of the upper eyelid is located 1 to 2mm below the upper boundary of the iris and with the vertical palpebral fissure measuring approximately 10mm3.
OBJECTIVE
This case report aims to demonstrate the resection of a segment of the eyelid levator muscle (Lester Jones technique) as treatment of congenital palpebral ptosis.
CASE REPORT
A 9-year-old female LSN patient from Campo Grande was brought by her mother for consultation at the plastic surgery clinic of the University Hospital of Federal University of Mato Grosso do Sul, because of a complaint of a "lazy eye." The patient was diagnosed with moderate congenital palpebral ptosis with good eyelid levator muscle function in the left eye (Figures 1 and 2).

Figure 1. Preoperative appearance.
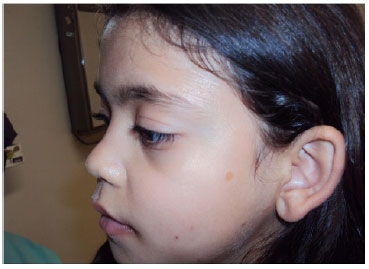
Figure 2. Preoperative appearance.
After preoperative examinations, the patient was subjected to surgical treatment of palpebral ptosis by transcutaneously shortening the eyelid levator muscle (Lester Jones technique). The procedure was performed under general anesthesia. The incision was demarcated approximately 9 mm from the ciliary line until the upper edge of the tarsus. Epitezan was used for eye protection. The area of the left eyelid was infiltrated with a lidocaine-adrenaline anesthetic solution at 1:100,000 concentration ratio. The incision was made at the demarcation site according to the following planes: the skin, orbicularis muscle, and orbital septum. The aponeurosis of the levator muscle, which is below the fat pockets, was identified. By dissecting cranially, below the fat pockets, the muscle belly of the eyelid levator muscle could be identified.
Resection of 10 mm of the eyelid levator muscle was performed. With careful monitoring of eustacia, the muscle was sutured with 6.0 nylon sutures at three points in separate U patterns and fixed to the tarsus. The septum was closed at separate points with 6.0 nylon sutures. The intradermal skin was sutured with 6.0 nylon sutures. Tarsorrhaphy was performed at two separate points, and occlusive dressing was maintained for 48 hours. After 7 days, the intradermal suture was removed, and the mother was instructed to massage the eyelid daily with Epitezan. The patient exhibited satisfactory results, with symmetry between the palpebral fissure and excursion (Figures 3-5).

Figure 3. Seven days after surgery.

Figure 4. Three months after surgery.

Figure 5. Three months after surgery.
DISCUSSION
The etiopathogenesis of congenital palpebral ptosis is the deficiency of striated muscle fibers of the levator muscle that occurs during the embryonic stage, the degree of which will determine ptosis severity1-3. The most used classification, aimed at surgical planning, considers the degree of ptosis as mild, moderate, and severe when the upper eyelid margin is 2-4 mm below the corneal limbus, 4-6mm below the corneal limbus, and 6 mm or more below the corneal limbus, respectively1-4. The eyelid levator muscle function can be evaluated by using the Berke and Wadsworth method. When the patient was in the primary position of gaze, the action of the frontal muscle is blocked by digit compression and the upper eyelid excursion between the infraversion (maximum relaxation) and supraversion (maximum contraction) is measured1-4. With this measurement, the eyelid levator muscle function can be graded as excellent, good, weak, or poor. Beard proposed a protocol for congenital ptosis, as shown in Table 12. According to the scientific literature, the Lester Jones technique5 is the most indicated for patients with moderate to severe ptosis, even with a poor eyelid levator muscle function.
CONCLUSION
Apart from causing undesirable cosmetic changes, palpebral ptosis becomes a functional problem when it reaches the pupillary area2. Unconsciously, the patient attempts to compensate it by contracting the frontal and corrugator muscles, raising the eyebrow and producing a horizontal sulcus on the forehead and vertical sulcus in the glabellar area. Thus, early treatment combined with an appropriate technique is important in order to achieve best results.
REFERENCES
1. Friedhofer H, Fernandes RO. Deformidades Congênitas e Adquiridas das Pálpebras. In: Carreirão S, Cardim V, Goldenberg D. Cirurgia Plástica. Sociedade Brasileira de Cirurgia Plástica. São Paulo, Atheneu, 2005. p.455-476.
2. Matayoshi S, Forno EA, Moura EM. Manual de Cirurgia Plástica Ocular. Atualidades Oftalmologia USP. São Paulo, Roca, 2004. p.87-107.
3. Friedhofer H, Oliveira RR. Ptose Palpebral. In: Mélega J M. Cirurgia Plástica Fundamentos e Arte. Cirurgia Reparadora de Cabeça e Pescoço. Rio de Janeiro, MEDSI, 2002. p.897-911.
4. Barbosa MV, Ferreira LM, Nahas FX. Ptose Palpebral. In: Ferreira L M. Cirurgia Plástica. Guias de Medicina Ambulatorial e Hospitalar, UNIFESP-EPM. São Paulo, Manole, 2007. p.349-354.
5. Pitanguy I, Sbrissa R. Atlas de Cirurgia Palpebral. Rio de Janeiro, Colina/Revinter, 1994. p.151-185.
1. Undergraduate, plastic surgery resident, Santa Casa de Campo Grande
2. Titular member of the Brazilian Society of Plastic Surgery, Regent of the Plastic Surgery Service at the Santa Casa de Campo Grande
3. Undergraduate, Plastic Surgery Resident, Santa Casa de Campo Grande
4. Undergraduate, Plastic Surgery Resident, Santa Casa de Campo Grande
5. Undergraduate, Plastic Surgery Resident, Santa Casa de Campo Grande
Institution: Santa Casa de Campo Grande UFMS University Hospital.
Corresponding Author:
Tatyanne Ferreira da Silva
TRua Teldo Kasper, 398 - Chácara Cachoeira
Campo Grande, MS, Brazil Zip code: 79040-840
E-mail: taty_1405@yahoo.com.br
Article submitted: July 19, 2011.
Article accepted: January 28, 2012.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket