



Case Report - Year 2015 - Volume 30 -
Reconstruction of the dorsal foot with a retrograde flow lateral supramalleolar flap in a 4-year-old child
Reconstrução de dorso do pé com retalho supramaleolar lateral de fluxo reverso em menor de 4 anos de idade
ABSTRACT
INTRODUCTION: Injuries in the distal third of the leg may expose noble areas that should be covered. The lateral supramalleolar flap is one of a series of flaps described in the last decade; it is an elevated fasciocutaneous flap in the lateral aspect of the lower leg, and is employed as a distally based pedicled flap. The purpose of this case report is to present the surgical results and the effectiveness of the lateral supramalleolar flap in extensive lower limb injuries with significant loss of substance in a 4-year-old child.
CASE REPORT: Patient A. K. E. S., a girl, was admitted 13 years previously. She had been in an accident, and had extensive injuries on the dorsum of the left foot, with exposure of noble areas approximately 6 cm in diameter. After debridement, lesion coverage was performed on the fifth day by using a fasciocutaneous lateral supramalleolar flap. The patient was discharged for outpatient monitoring and progressed without complication. She only returned to the hospital 13 years later, overweight and complaining of swelling on the dorsal aspect of the foot. Lipectomy of the distal third of the flap was performed, with uncomplicated progress. A second procedure for the proximal third was scheduled six months later.
DISCUSSION: Injuries in the distal third of the leg may expose noble areas. Lateral supramalleolar, sural, and pedicled perforating flaps have similar applications, but show individual technical peculiarities. The lateral supramalleolar flap has no need for microsurgery, is rapidly performed, and simulates the receiving area while considering several local characteristics.
CONCLUSION: This flap is easily implemented and reproducible, and can be used in children younger than 5 years of age. It is an alternative for injuries in the lower third of the leg, the ankle, and the foot.
Keywords: Surgical flaps; Lower extremity; Reconstructive surgical procedures; Leg injuries.
RESUMO
INTRODUÇÃO: Lesões em terço distal da perna podem deixar expostas áreas nobres, que devem ser recobertas. O retalho supramaleolar lateral faz parte de uma série de retalhos descritos na última década, é fasciocutâneo elevado no aspecto lateral da perna inferior, sendo empregado como um retalho pediculado com base distal. O objetivo do presente relato de caso é apresentar os resultados cirúrgicos e a eficácia do retalho supramaleolar lateral em lesões extensas no membro inferior com perdas de substâncias significativas em criança de 4 anos.
RELATO DE CASO: Paciente A.K.E.S., sexo feminino, foi internada há 13 anos, vítima de atropelamento, com lesão extensa em dorso de pé esquerdo com exposição de áreas nobres de aproximadamente seis centímetros de diâmetro. Após desbridamento, no quinto dia foi realizada cobertura da lesão com retalho fasciocutâneo supramaleolar lateral. A paciente teve alta para acompanhamento ambulatorial, evoluindo sem intercorrência. Ela retornou ao serviço apenas 13 anos após com sobrepeso e reclamando do aumento de volume no dorso do pé. Foi realizada lipectomia do terço distal do retalho, evoluindo sem intercorrência. Um segundo procedimento do terço proximal foi programado para seis meses após.
DISCUSSÃO: Lesões no terço distal da perna podem expor áreas nobres. Os retalhos supramaleolar lateral, sural e de perfurantes pediculados possuem aplicações semelhantes, mas apresentam peculiaridades técnicas individuais. Como vantagens no retalho supramaleolar lateral: não há necessidade de microanastomoses, é rápido para ser executado e simula a área receptora em várias características locais.
CONCLUSÃO: É um retalho de maior facilidade de execução e reprodutível, podendo ser realizado em crianças menores de 5 anos. Tem sua aplicação como alternativa para lesões em terços inferiores da perna, tornozelo e pé.
Palavras-chave: Retalhos cirúrgicos; Extremidade inferior; Procedimentos cirúrgicos reconstrutivos; Traumatismos da perna.
There has been an improvement in the quality and success of orthopedic salvage in association with advances in trauma and emergency management. Consequently, there has been an increase in the need for repair of injuries in hard-to-reach places. For the treatment of injuries in the lower third of the foot, local and microsurgical flaps are used1.
The decision on the best technique depends on several factors, including location, extent of injury, exposure of noble areas, and the experience of the surgeon2. Injuries in the distal third of the leg may expose noble areas that should be covered with good quality vascularized tissue3.
The lateral supramalleolar flap is one of a series of flaps described in the last decade. It is based on secondary arteries, and is an elevated fasciocutaneous flap in the lateral aspect of the lower leg, employed as a distally based pedicled flap1.
The vascular supply of the lateral supramalleolar flap is based on the anastomotic arcade of the ankle. The perforating branch of the fibular artery forms anastomoses with the anterior lateral malleolar artery, which emerges from the anterior tibial artery, descends anteriorly to the tibiofibular syndesmosis, and anastomoses with the lateral tarsal artery on the lateral side of the foot. It is accompanied by a venous network that can replace the dorsalis pedis artery (dorsal artery of the foot). The cutaneous branches run anterior to the fibula, taking an upward course and anastomosing with the vascular network that accompanies the superficial fibular nerve1.
Skin flaps based on pedicled perforating vessels, especially for coverage of the distal third of the leg in children, have hardly been explored, with few reports in the literature.
Thus, the purpose of this case report is to present the surgical outcomes and the efficacy of the lateral supramalleolar flap in extensive injuries in the lower limb, with significant tissue loss, in a 4-year-old child.
CASE REPORT
Patient A. K. E. S., a girl, was admitted 13 years previously, after being in an accident, with extensive injuries on the dorsum of the left foot, including bone and ligament exposure approximately 6 cm in diameter. After debridement of the injury upon admission, coverage with a fasciocutaneous lateral supramalleolar flap on the anterior region of the left foot was scheduled and performed on the fifth day (Figure 1). The patient was hospitalized for 14 days. On outpatient follow-up, the flap presented without necrosis and with good perfusion (Figure 2).
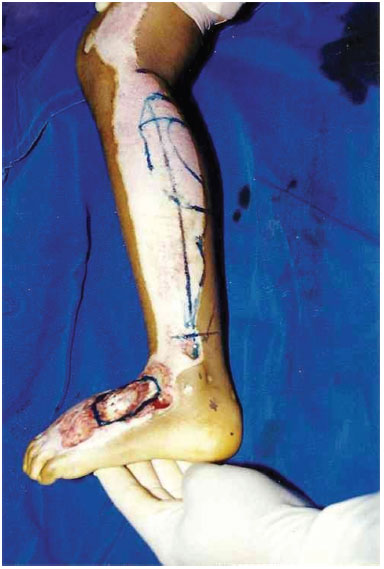
Figure 1. Preoperative appearance with the demarcations of the flap.

Figure 2. Three-month postoperative appearance.
After outpatient discharge, the patient only returned to the hospital 13 years later, overweight and complaining of swelling on the dorsal aspect of the foot. A new surgical treatment was planned, to reduce the thickness of the flap (Figure 3). Lipectomy of the distal third of the flap was performed. The patient was hospitalized for 24 hours, discharged for outpatient follow-up, and progressed without complications. A second procedure on the proximal third was scheduled six months later (Figure 4).

Figure 3. Preoperative planning of refinements.

Figure 4. Postoperative surgical refinement.
DISCUSSION
Injuries of the distal third of the leg may expose noble areas, such as bones, tendons, nerves, and vessels. These require highly complex surgeries, such as microsurgical flaps, to ensure satisfactory aesthetic and functional results4.
The donor and recipient areas of the distal leg allow good functional and aesthetic results, due to their greater elasticity and thinner flaps; however, the flaps are thicker in children5. Fasciocutaneous flaps include the fascia, and result in increased vascularization. This has resulted in an increase in their indication for coverage of lesions in distal areas6. With the introduction of 180º rotated helical flaps, based on a perforating vessel as the axis, the versatility for the repair of difficult lesions has expanded7.
The distribution of perforating arteries is random in the leg. However, 10 predictable fasciocutaneous locations were described by Whetzel et al., based on intermuscular septa. These studies are useful for the planning of flaps for coverage of the lower third of the leg, and can be used to perform different types of treatments8.
Lateral supramalleolar, sural, and pedicled perforating flaps have similar applications, but display individual technical peculiarities. The lateral supramalleolar flap, described by Masquelet1, aroused little interest among other authors. In a study comparing the lateral supramalleolar and sural flaps, Touam et al.9 reported an 18.5% incidence of partial or total necrosis with the lateral supramalleolar flap. More recently, Voche et al.10, in a series of 41 cases, reported a 7.3% rate of necrosis. However, these two studies agreed that the lateral supramalleolar flap presents a high level of technical difficulty, and is a second option to the distally based sural flap.
As a fasciocutaneous flap, the lateral supramalleolar flap expanded the possibility of appropriate skin coverage of lesions in distal regions of the leg, ankle, and foot, and may be performed in adults and children. Success is due to a thinner flap, which offers like-for-like features, such as similarity in color and texture10.
The indications for the lateral supramalleolar flap outweigh those of the sural flap, and its success rate makes it an alternative to microsurgical flaps (which are more complex and have a greater risk of losses)11.
The lateral supramalleolar flap has no need for microsurgery, is rapidly performed, simulates the receiving area in several aspects, and is reproducible in children.12 The complications are the same as for any type of flap, including infection, hematomas, dehiscence, and necrosis4.
CONCLUSION
This is an easily executed and reproducible flap, and can be performed in children. Refinements were needed to obtain optimal aesthetic quality, with good functional recovery. It can be applied as an alternative for injuries in the lower third of the leg, the ankle, and the foot.
REFERENCES
1. Masquelet AC, Gilbert A. Atlas colorido de retalhos na reconstrução dos membros. Rio de Janeiro: Revinter; 1997. p.160-6.
2. Rezende MR, Rabelo NTA, Benabou JE, Wei TH, Mattar Junior R, Zumiotti AV, et al. Cobertura do terço distal da perna com retalhos de perfurantes pediculados. Acta Ortop Bras. 2008;16(4):223-9. DOI: http://dx.doi.org/10.1590/S1413-78522008000400007
3. Ramos RR, Bloch RJ. Reparações do membro inferior. In: Bloch RJ, Andrews JM, Chem RC, Azevedo JF, Psillakis JM, Santos ID, eds. Atlas anatomoclínico dos retalhos musculares e miocutâneos. São Paulo: Roca; 1984. p.311-68.
4. Batista JC. Retalho supramaleolar de fluxo reverso: aplicações clínicas. Rev Bras Cir Plást. 2011;26(1):140-6. DOI: http://dx.doi.org/10.1590/S1983-51752011000100025
5. Demirtas Y, Kelahmetoglu O, Cifci M, Tayfur V, Demir A, Guneren E. Comparison of free anterolateral thigh flaps and free muscle-musculocutaneous flaps in soft tissue reconstruction of lower extremity. Microsurgery. 2010;30(1):24-31.
6. Monteiro Jr AA, Morais J, Figueiredo JCA, Amaral AB, Kalô FJ. Cirurgia reparadora do membro inferior. In: Mélega JM, ed. Cirurgia reparadora de tronco e membros. Cirurgia Plástica Fundamentos e Arte. Rio de Janeiro: Guanabara Koogan; 2004. p.714.
7. Jiga LP, Barac S, Taranu G, Blidisel A, Dornean V, Nistor A, et al. The versatility of propeller flaps for lower limb reconstruction in patients with peripheral arterial obstructive disease: initial experience. Ann Plast Surg. 2010;64(2):193-7. PMID: 20098106 DOI: http://dx.doi.org/10.1097/SAP.0b013e3181a72f8c
8. Monteiro Júnior AA, Alonso N. Reparação de perdas cutâneas na perna e no pé com retalho fasciocutâneo de pedículo distal. Rev Soc Bras Cir Plást. 1991;6(1/2):33-40.
9. Touam C, Rostoucher P, Bhatia A, Oberlin C. Comparative study of two series of distally based fasciocutaneous flaps for coverage of the lower one-fourth of the leg, the ankle, and the foot. Plast Reconstr Surg. 2001;107(2):383-92. DOI: http://dx.doi.org/10.1097/00006534-200102000-00013
10. Voche P, Merle M, Stussi JD. The lateral supramalleolar flap: experience with 41 flaps. Ann Plast Surg. 2005;54(1):49-54. DOI: http://dx.doi.org/10.1097/01.sap.0000139565.36738.b3
11. Chang SM, Zhang K, Li HF, Huang YG, Zhou JQ, Yuan F, et al. Distally based sural fasciomyocutaneous flap: anatomic study and modified technique for complicated wounds of the lower third leg and weight bearing heel. Microsurgery. 2009;29(3):205-13. DOI: http://dx.doi.org/10.1002/micr.20595
12. Amarante J, Costa H, Reis J, Soares R. A new distally based fasciocutaneous flap of the leg. Br J Plast Surg. 1986;39(3):338-40. DOI: http://dx.doi.org/10.1016/0007-1226(86)90043-3
1. Santa Casa de Campo Grande, Campo Grande, MS, Brazil
2. Sociedade Brasileira de Cirurgia Plástica, São Paulo, SP, Brazil
3. Universidade Federal de Mato Grosso do Sul, Campo Grande, MS, Brazil
4. Hospital Regional Rosa Pedrossian, Campo Grande, MS, Brazil
Institution: Hospital Santa Casa de Campo Grande, MS, Brazil.
Corresponding author:
Fábio Tacla Saad
Rua Alagoas, 761, Bairro Jardim dos Estados
Campo Grande, MS, Brazil Zip code 79020-121
E-mail: fabiotsaad@gmail.com
Article received: October 25, 2011.
Article accepted: February 19, 2012.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket