



Ideas and Innovation - Year 2015 - Volume 30 -
Mammoplasty with bipedicled flap from the pectoral muscle: 30 years of experience
Mamoplastia com retalho bipediculado de músculo peitoral: 30 anos de experiência com a técnica
ABSTRACT
INTRODUCTION: Several breast augmentation techniques have been developed to avoid late ptosis. However, these techniques result in persistent pendulum and changed shape due to loss of filling in the upper pole. The combination of breast augmentation with a thoracic flap involving a bipedicled flap from the greater pectoral muscle has been used with good results that are maintained in late postoperative periods.
METHOD: More than 4,000 procedures were performed using the author's technique. The marking of traditional mammoplasty and construction of the inferior pedicle flap were performed as described by Ribeiro. A pectoral muscle strap was divulsed and the thoracic flap passed through and attached to the chest wall. The muscle and glandular flaps were wrapped by the upper pole tissue and sutured to the lateral breast pillars.
RESULTS: Use of the thoracic flap technique fixed by a pectoral muscle strap results in minimum pendulum, which provides better long-term aesthetic results. With this technique, the breast tissue is divided and repositioned in the desired location while maintaining the breast shape rather than depending on the dermal closure to provide the final shape.
CONCLUSION: This technique provides long-term preservation of the upper breast pole and reduced scar tension with consequent aspect improvement; it also eliminates post-operative pendulum movement (ptosis) without significantly increasing surgical time.
Keywords: Mammoplasty; Surgical flaps; Pectoral muscles.
RESUMO
INTRODUÇÃO: Existem inúmeras técnicas de mamoplastia com objetivo de evitar a ptose tardia. Observamos em todas estas técnicas que a forma da mama após a sua báscula permaneceu com perda de preenchimento do seu polo superior. A associação da mamoplastia com o uso do retalho de base torácica associado ao retalho bipediculado de músculo peitoral maior tem sido utilizada devido ao bom resultado que é mantido num pós-operatório tardio.
MÉTODO: Foram feitos mais de 4000 procedimentos utilizando a técnica do autor. Foi realizada a marcação de mamoplastia tradicional e confecção de retalho de pedículo inferior conforme descrito por Ribeiro. Divulsiona-se uma faixa do músculo peitoral e realiza-se a passagem completa do retalho torácico através da alça muscular com posterior fixação do retalho à parede torácica. Os retalhos muscular e glandular são envolvidos pelo tecido do polo superior fazendo se a sutura dos pilares laterais.
RESULTADOS: Com a utilização da técnica de um retalho torácico, fixado por uma alça de músculo peitoral, obtivemos uma báscula mínima que forneceu um melhor resultado estético a longo prazo. Com esta técnica, o tecido mamário é dividido e reposicionado para o local desejado, mantendo a forma da mama e não dependendo do fechamento dérmico para se obter o contorno final.
CONCLUSÃO: Observamos nos casos operados a manutenção do polo superior da mama mesmo tardiamente, redução da tensão sobre a cicatrização com consequente melhora do aspecto, ausência do movimento de báscula (ptose) pós-operatória, sem aumento significativo no tempo cirúrgico.
Palavras-chave: Mamoplastia; Retalhos cirúrgicos; Músculos peitorais.
The objectives of mammoplasty are to reduce excess glandular tissue and hypertrophy; remodeling of the breast cone to treat ptosis (mammary reduction) focuses on maintaining breast volume, while mastopexy addresses breast elevation and shape1.
Several breast augmentation techniques have been developed to avoid late ptosis. These various efforts have sutured the breast to the costal cartilages (Gaillard, 1882; Girard, 1910) or to the periosteum or fascia of the greater pectoral muscle (Micheland Pousson, 1897; De Quervain, 1926; Rangnell, 1946), fixing the gland to the pectoral muscle; other methods used silicone lamina to support the breast (Bustus, 1992). However, the pendulum movement persisted in all of these techniques, with loss of filling of the upper pole2.
The combination of breast augmentation with a thoracic-based flap such as the bipedicled flap from the greater pectoral muscle, has been used due to the good results that are maintained in late postoperative periods. The upper pole of the breast remains voluminous and the vertical breast scar remains above or at the level of the new inframammary crease, with minimum breast pendulum3,4.
OBJECTIVE
The objective of this study was to demonstrate results obtained after 30 years of experience with breast augmentation surgery using the muscle flap technique described by Milton Daniel.
METHODS
More than 4,000 procedures were performed using the author's technique. We present pre- and late post-operative (minimum three years) images.
Technique
The mammoplasty was marked with a periareolar inverted "t" or "L" construction of the inferior pedicle flap as described by Ribeiro. The flap was between 4 and 5 cm wide, extended up to 1 to 2 cm from the bottom edge of the areola, and was at least 2 cm thick. The muscle flap was lifted and the glandular flap passed beneath. A 4-cm wide strap of pectoral muscle was divulsed at the height of the fifth intercostal space. After complete passage of the thoracic flap through the muscle strap (Figures 1, 2, 3, 4, 5, and 6), the donor muscle area was sutured with two separate nylon 4.0 sutures, the chest wall flap was sutured with simple sutures to leave a more rounded format, and the flap was attached to the thoracic wall with nylon 3-0 sutures.
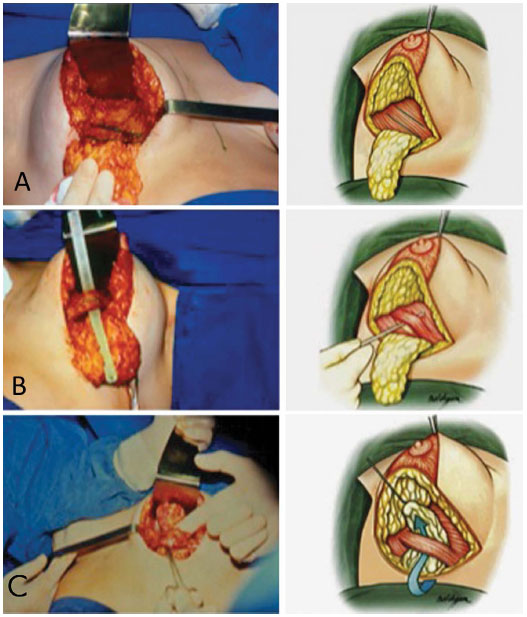
Figure 1. A: Construction of the dermofat flap and marking of the bipedicled muscular flap with methylene blue; B: Opening of the tunnel under the muscle strap to allow passage of the flap, and passage of the flap under the strap; C: Positioned flap.

Figure 2. Flap aspect after attachment to the pectoral muscle.

Figure 3. A: Preoperative aspect in the top left frontal photo and two-year postoperative aspect. B: Preoperative and two-year postoperative profiles. C: Breast movement with muscle and muscle strap contraction, and demonstration that lateralization of the breast does not occur when the patient is in ventral recumbency.

Figure 4. Pre-operative (right) and six-year postoperative (left) images.
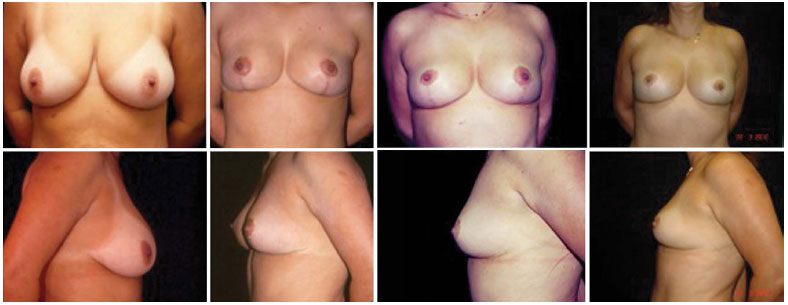
Figure 5. Sequence of images from right to left: preoperative, one-, nine-, and 19-year postoperative images.
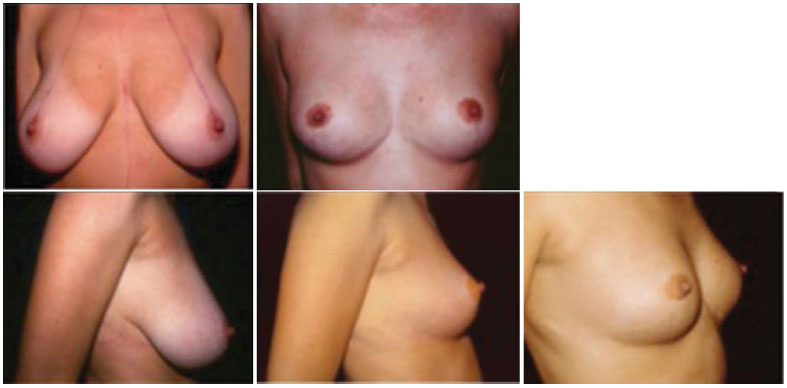
Figure 6. Pre- and 11-year postoperative images.
The muscle and glandular flaps were wrapped around the tissue of the upper pole and the lateral breast pillars were sutured with nylon 3-0 sutures.
On the eighth day, the patients started exercises to contract the pectoral muscle so that the breast was pulled up, thus controlling the weight on the scars. Normal activities were permitted on the 15th day post-operation.
The senior surgeon performed the operations in all cases.
RESULTS
Figure 1 - Thoracic flap and dissected muscle strap for flap passage. Side: schematic drawing of the technique.
Figure 2 - Pre-operative period (25 years) and two-, five-, 10-, and 20-year post-operative aspects.
Figure 3 - Pre-operative and two-year postoperative aspects.
Figure 4 - Pre-operative and six-year postoperative aspects.
Figure 5 - Pre-operative, one-year, nine-year, and 19-year post-operative aspects.
Figure 6 - Pre-operative and 11-year postoperative aspects.
DISCUSSION
Several common techniques used to prevent ptosis after mammoplasty utilize static mechanisms to correct breast ptosis. The breast is thus subject to the adverse and continuous action of gravity. A muscle flap involving the lower pole of the breast raises the breast when the muscle is contracted, thus dynamically counter-acting the effects of gravity and preventing ptosis.
The thoracic wall flap, maintained by a loop of the greater pectoral muscle and sutured in a top position, maintains the fill in the upper breast pole. The thoracic flap technique maintains the modified breast shape above the level of the new submammary crease, resulting in better long-term results.
The weight of glandular tissue on the vertical surgical scar increases the vertical length of the scar, leading to varied results according to technique. Thus, each pedicle type and location will press the lower pole differently and uniquely stretch each vertical scar5. Contraction of the pectoral muscle elevates the breast through the muscle strap, thus avoiding the action of gravity and preventing mammary ptosis. This technique prevents breast pendulum and decreases the weight of the breast on the scar, thus reducing its enlargement and hypertrophy.
Use of a thoracic flap supported by a pectoral muscle strap resulted in minimum pendulum, which provided better long-term aesthetic results. With this technique, the breast tissue is divided and repositioned in the desired location, thus maintaining the shape of the breast without relying on the dermal closure for the final shape.
CONCLUSION
Even many years after the operations, we observed preserved volume of the upper breast pole, reduced scar tension with consequent aspect improvement, and absence of post-operative pendulum movement (ptosis); furthermore, this technique can be performed without significant increase in surgical time.
REFERENCES
1. Mélega JM, Reiff ABM. Introdução à cirurgia plástica. In: Mélega JM. Cirurgia plástica: fundamentos e arte: princípios gerais. Rio de Janeiro: Medsi; 2002. p.3-8.
2. Ahmad J, McIsaac SM, Lista F. Does knowledge of the initial technique affect outcomes after repeated breast reduction? Plast Reconstr Surg. 2012;129(1):11-8. PMID: 22186496
3. Graf R, Araújo LRR, Rippel R, Graça Neto L, Pace D, Biggs T. Mamaplastia vertical com retalho de parede torácica. Rev Soc Bras Cir Plást. 2005;20(3):148-54.
4. Rinker B, Veneracion M, Walsh CP. Breast ptosis: causes and cure. Ann Plast Surg. 2010;64(5):579-84. PMID: 20354434 DOI: http://dx.doi.org/10.1097/SAP.0b013e3181c39377
5. Souza AA, Faiwichow L, Ferreira AA, Simão TS, Pitol DN, Máximo FR. Avaliação das técnicas de mamoplastia quanto a sua influência tardia na distância do complexo areolopapilar ao sulco inframamário. Rev Bras Cir Plást. 2011;26(4):664-9. DOI: http://dx.doi.org/10.1590/S1983-51752011000400022
1. Sociedade Brasileira de Cirurgia Plástica, Curitiba, PR, Brazil
2. Universidade Federal do Paraná, Curitiba, PR, Brazil
3. Hospital Universitário Evangélico de Curitiba, Curitiba, PR, Brazil
Institution: Clinica Dr. Milton Daniel - Curitiba, PR, Brazil.
Corresponding author:
Milton Jaime Bortoluzzi Daniel
Av. Visc. de Guarapuava, nº 4742, Batel
Curitiba, PR, Brazil Zip Code 80240-010
E-mail: mdaniel@milenio.com.br
Article received September 14, 2013.
Article accepted December 08, 2013.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket