



Reviw Article - Year 2015 - Volume 30 -
Risk factors of burn injury and prevention methods in the elderly
Fatores de risco e métodos de prevenção de queimaduras em idosos
ABSTRACT
INTRODUCTION: As the population ages, the elderly become more susceptible to burn injuries. Studies that assess the epidemiological data and risk factors of burn injuries in the elderly are valuable tools to evaluate the strategies developed with the aim of preventing these injuries.
OBJECTIVE: We aimed to describe the risk factors of burn injury and prevention methods in the elderly. In addition, we aimed to determine the correlation between the risk factors and the epidemiological data on the incidence and mortality from studies published in the literature worldwide.
METHODS: In the literature review, we consulted 21 articles published between January 2000 and December 2012 in 4 continents from the following databases: Lilacs, Medline, PubMed, Cochrane, and ScienceDirect.
RESULTS: We selected 21 articles from 4 continents. The research period ranged from 2 to 28 years. The number of elderly patients ranged from 45 to 308. Their mean age ranged from 64.5 to 85 years. The predominant accident site was the place of residence (68% to 98%), with the kitchen being the most prevalent location (17% to 65%), followed by the bathroom (9% to 31%). The main causes were direct fire or flammable liquids (29% to 73%) and scalding (17% to 66%). Injury by inhalation was found in 12% to 41% of the elderly, with mortality ranging from 6% to 65%.
CONCLUSION: We conclude that the place of residence is the most important and prevalent location of burn injuries in the elderly. Therefore, preventive measures against burn injuries in this type of environment should be intensified.
Keywords: Burn injury; Elderly; Risk factors; Primary prevention.
RESUMO
INTRODUÇÃO: Com o envelhecimento populacional, os idosos estão sujeitos a aumento dos traumas por queimadura. Estudos que realizam mensuração de dados epidemiológicos e fatores de risco de queimadura em idosos são um recurso importante para avaliar resultados de tratamento e desenvolvimento de estratégias que visem à prevenção.
OBJETIVO: Descrever os fatores de risco e os métodos de prevenção de queimadura em idosos, correlacionando-os aos dados epidemiológicos de incidência e mortalidade em estudos publicados na literatura mundial.
MÉTODO: Na revisão da literatura realizada, foram consultados 21 artigos de 4 continentes nas bases de dados: Lilacs, Medline, PubMed, Cochrane e ScienceDirect, de janeiro de 2000 a dezembro de 2012.
RESULTADOS: Foram selecionados 21 artigos de 4 continentes. O período variou de 2 anos a 28 anos. O total de pacientes idosos variou de 45 a 308. A idade média foi de 64,5 a 85 anos. O gênero foi descrito em 18 trabalhos, sendo 1132 homens e 1076 mulheres. O local predominante do acidente foi a residência (68 a 98%), com a cozinha sendo a localidade prevalente (17 a 65%), seguindo o banheiro em 9 a 31%. Os agentes principais foram o fogo direto ou líquidos inflamáveis (29 a 73%) e a escaldadura (17 a 66%). Lesão por inalação foi encontrada em 12 a 41% dos idosos e a mortalidade variou de 6 a 65%.
CONCLUSÃO: Conclui-se que a residência é o local de maior importância e prevalência da queimadura em idosos e devem ser intensificadas as medidas de prevenção deste acidente neste ambiente.
Palavras-chave: Fatores de risco; Idosos; Prevenção primária; Queimaduras.
The world's elderly population is continuously increasing owing to the improvements in health and medical care. This increase leads to a higher number of elderly people that require medical care for injuries1. During the year 2012, the American Burn Association surveyed the data collected in the United States, Canada, and Sweden, and found that among the 183,000 patients who were assisted in the period between 2002 and 2011 in 91 hospitals specialized in the treatment of burn injuries, 12% corresponded to people older than 60 years2. The population of elderly burn victims brings high costs to the health system, with an approximate average expenditure of US$ 1,000.00/day in the United States, referring to patients hospitalized in reference centers for burn treatment, with longer hospitalization periods and higher rates of complications and mortality1,3. These patients are at a higher risk of burn injury because of known risk factors such as slower reaction to injury, limited mobility, lower capacity to interpret risks due to the weakening of reasoning ability, and premorbid factors that influence both incidence and prognosis, such as chronic diseases, alcoholism, medication use, senility, and psychiatric or neurological disorders1,3. In prevention studies, most of the risks factors have been shown to be preventable with education of the elderly population, family members, and caregivers. Thus, effective elderly burn prevention programs are required. These same studies also emphasized professional training since graduation and continuous training of experts in the fields of geriatrics and family physicians in order to effectively prevent burn cases in the elderly4.
Therefore, development of burn prevention systems for the elderly is essential, focused mainly on the place of residence, provided that most burn injury cases in patients older than 60 years occur during their stay at home, unlike in young adults, in which most accidents, according to the literature, occur during work-related activities5.
The objective of this study was to describe the risk factors and burn prevention methods in the elderly. In addition, we aimed to determine the correlation between the risk factors and the epidemiological data on the incidence and mortality from studies published in the literature worldwide.
METHODS
This study consisted of a systematic review of specialized literature. We selected articles published in Portuguese and English languages between January 1, 2000, and December 31, 2012, in the following databases: Lilacs, Medline, PubMed, Cochrane, and ScienceDirect. The articles were indexed according to the Health Sciences Descriptors (DeCS) and MESH (burn, elderly, primary prevention, queimados, idosos, and prevenção). The search returned 189 articles in the PubMed/Medline database, 46 articles in the Cochrane database, 70 articles in the Lilacs database, and 240 articles in the ScienceDirect database. We included original articles that established a relationship between burn injury characteristics such as burn localization, type of burn, average burned body surface, country, time of the year, total number of patients with burn injuries and studied, age, sex, mortality, percentage of injuries caused by inhalation, and information on injury pre-morbidity conditions. We excluded studies performed in animals and any review study that did not address burn injuries in humans or burn injuries in the elderly, or had no data referring to the epidemiology of the case in the study. Of the articles found in the search, 21 met the inclusion and exclusion criteria and showed epidemiological data regarding the circumstances of the burn injury.
RESULTS
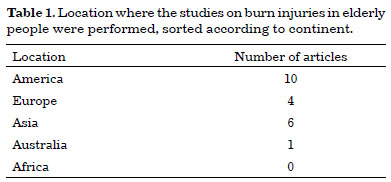
The studies were grouped according to the search variables (inclusion criteria), as not all of them were included in the reviewed studies. The studies were representative of several world regions, representing 4 of the 5 world continents. Table 1 shows the representativity of the studies based on the study's location in each continent. The research period referring to each study ranged from 2 to 28 years.
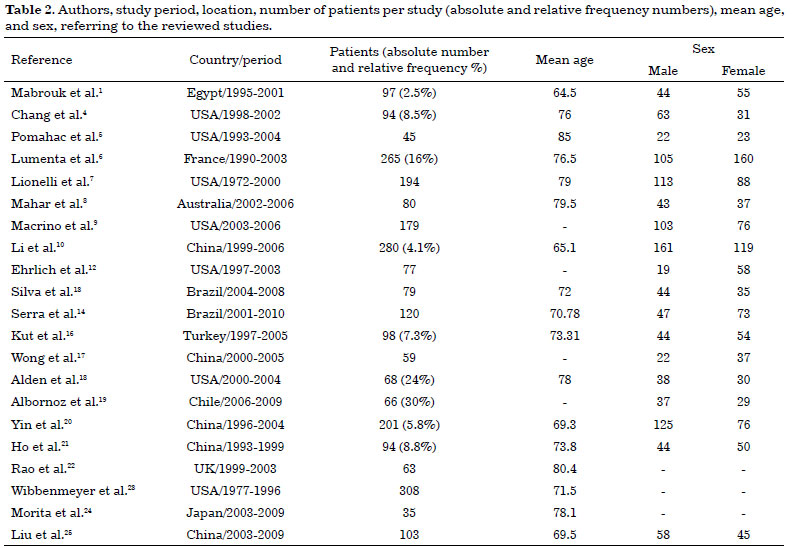
The total number of elderly patients studied ranged from 45 to 308 per study, which represented 2.5% to 30% of the total number of burn injury patients from all ages in healthcare services. The mean age ranged from 64.5 and 85 years, with a standard deviation of 5.38. The sex was described in 18 studies, including 1132 men and 1076 women across all studies (Table 2).
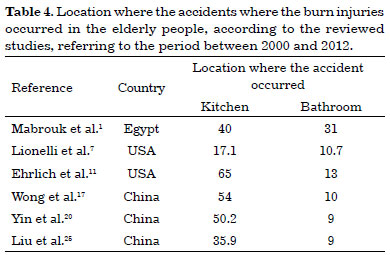
In 10 of these studies, the elderly's location when the burn injury occurred was described (Table 3). Among these locations, the most predominant was the patient's place of residence, ranging from 68% to 98% of the time. In 6 of these studies, the authors specified the location within the residence where the elderly became injured, the kitchen (17% to 65%) during food preparation being the most prevalent place, followed by the bathroom (9% to 31%), mostly associated with baths with hot water (Table 4).

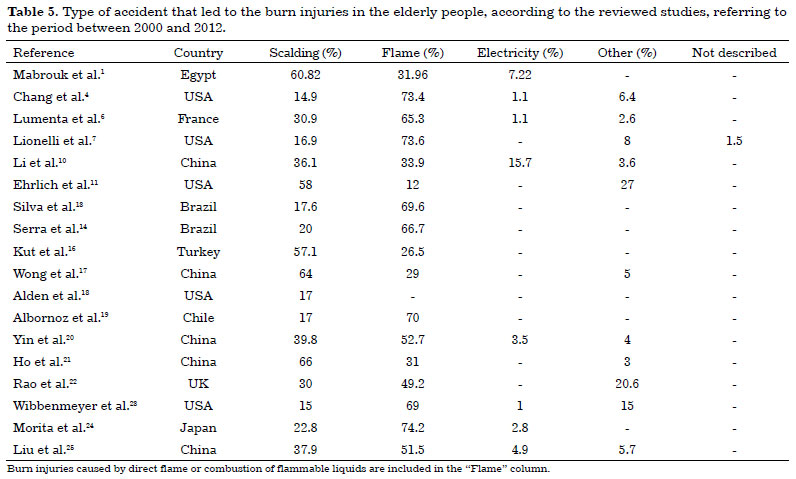
In 18 of the reviewed studies published between 2000 and 2012, the most prevalent type of burn injury was analyzed. In 12 of these studies, direct flame or combustion of flammable liquids was the main cause of burn injuries (29.0% to 73.6%). Scalding with hot liquid was the second highest cause and the most frequent type of injury in 6 of the studies (17% to 66%; Table 5).
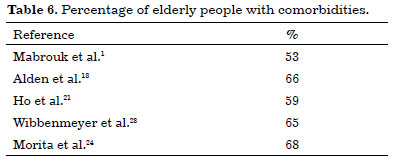
The number of elderly people who had pre-injury morbidities was high in the 5 studies that considered this information. Table 6 shows that in these studies, more than 50% of the elderly population with burn injuries had some chronic disease at the time of injury.
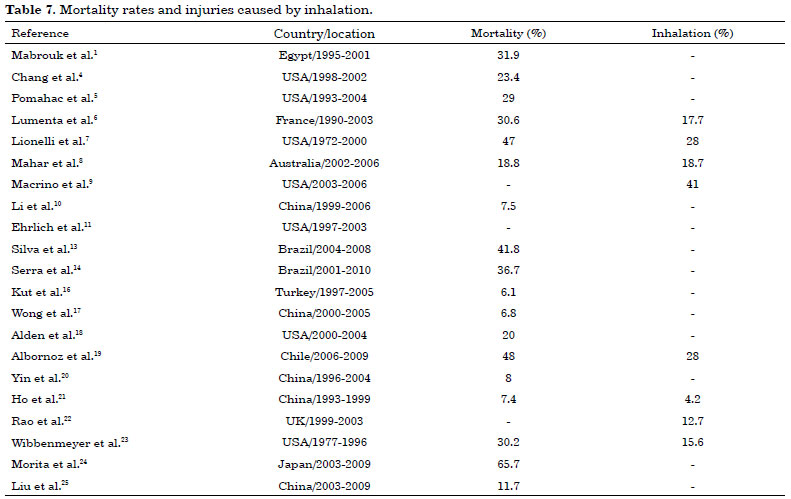
Injury caused by inhalation was described in 6 studies, with an incidence ranging from 12% to 41% in the affected elderly and mortality ranging from 6.8% to 65% of all elderly people (Table 7).
DISCUSSION
Several studies have demonstrated an increase in the world's elderly population1,6. The elderly are more susceptible to injuries and are more likely to have a poor prognosis due to physiological changes that are typical of senility such as poor vision, slower reaction to injuries, movement limitations with more time spent on the bed, neurological problems leading to a lower capacity to evaluate risks, skin atrophy with slower scarring, and an immune system with lower efficacy and more susceptible to infections5,7-10.
In the United States, burn injuries are the fifth leading cause of death by accident and the second leading cause of death in home-related accidents11-13. Considering the increase in the world's elderly population and the risk of injury that the elderly are exposed to, an increase in the prevalence of burn injury in this age group is expected7. Given the limitations of elderly people, they are described as having a higher risk of mortality from burn injuries compared to young adults, with an estimated mortality risk 4 times higher than in the younger age groups8,11,14-16. Even with the improvement in the treatment of burn injuries and the decrease in mortality among young patients, the literature fails to show an improvement in the prognosis in the elderly, which remains associated with high mortality rates and injury sequelae, mainly due to chronic diseases that complicate aspects of the treatment, such as fluid resuscitation in patients with heart disease or infections in those with diabetes and decreased immune response. Furthermore, the literature shows that the elderly have a lower probability of returning to their previous activities due to sequelae derived from burn injuries, especially when compared with young adults5,9,14,17-19.
This study aimed to collect epidemiological data and identify possible burn causes in the elderly in order to promote the development of methods to prevent these accidents. This type of accident is prevalent in several regions of the world, and the results in this study are representative of 10 countries in 4 of the 5 continents of the world. Our data show that the prevalence is not sex-based, as the studies show a similar prevalence for each sex.
The most frequent location where burn injuries occur in the elderly was their own residence, ranging from 68% to 98% of the time, whereas in young adults, burn injuries were associated with their work-related activities5. Burn injuries occur more frequently in the elderly who live alone or during the day, when their families are at work, and who perform their daily activities such as cooking or using hot water for the bath, without any family supervision1,20. In our literature search for locations within the place of residence in which the elderly are more often involved in accidents and which activities they were involved during the accident, we found that the most of the accidents occurred in the kitchen, with a prevalence of up to 65%, followed by the bathroom, as demonstrated in this study. This shows how much the elderly require supervision when performing daily activities that are as simple as cooking or bathing, as a great part of these elderly people lose their sense of danger when performing those activities. The most prevalent type of accident was by direct flame, followed by scalding. Scalding is a common occurrence in the winter months and in countries with colder climates, especially during the preparation of the bath, in which tap water at high temperatures is used11,16. Most of the elderly have chronic diseases, with a comorbidity prevalence of 53% to 68%, which makes their healing and treatment more difficult. Thus, the mortality of these elderly people remains high, especially in those who are older, who have a larger portion of body surface burned, or whose injury was by inhalation, as these are the factors that have more influence on prognosis6,21-25. In this study, we found data indicating that 4% to 28% of the elderly were injured by inhalation, with mortality rates as high as 65% of the burn injury cases (6.8% to 65%), showing that the mortality rates are high and described as being up to 400% higher in the ones with injuries by inhalation7.
Most of the accidents involving the elderly are preventable9. In a study that conducted interviews with elderly people after incurring burn injuries, up to 85% of the interviewees reported that the accident could have been prevented26. As demonstrated, most of the accidents occurred inside the place of residence, especially when the elderly were alone and performing their daily tasks. The supervision of patients with comorbidities, movement restrictions, or any kind of debility is important to avoid accidents associated with high mortality rates and functional impairment of those who survive. Government programs that aim to promote the supervision of elderly patients, training of healthcare teams, family members, and caregivers for elderly orientation are important to decrease the incidence of accidents that occur in this group age, as well as the use of multimedia as a means to promote the preventive methods to a wider scope2. Preventive strategies should be focused on the residences, especially in places such as the kitchen and the bathroom, because of the high prevalence of accidents in these locations. Visits to the residencies in order to provide orientation, detection of risks, with respective changes and adaptations of the surroundings, are important to promote the prevention of accidents and to reduce damages when these occur. Among the methods described that reduce the damage caused by these accidents are as follows: improvement of first aid, fast service response, shortening the interval from onset of injury to admission to hospitals, and multidisciplinary care that aim at early functional recovery. Thus, understanding the epidemiology of each region, individually, is important in order to propose and improve burn prevention systems based on their prevalence, as well as to provide orientation to healthcare teams regarding the need to focus on possible region-associated risks.
CONCLUSION
Owing to the increase in the worldwide elderly population, the prevalence of burn injury accidents in this population has increased. The need for preventive measures against this type of accident has become even more relevant according to the mortality from this type of injury in the elderly population, as even with the improvement in the treatments, the mortality rates remain high, with high costs to the health system.
Implementing prevention systems based on regional statistics regarding the detection of the risks of burn injuries to which the elderly are susceptible is the best method to avoid tragic accidents with major repercussions, thus requiring the involvement of governmental departments in order to improve these prevention methods.
REFERENCES
1. Mabrouk A, Maher A, Nasser S. An epidemiologic study of elderly burn patients in Ain Shams University Burn Unit, Cairo, Egypt. Burns. 2003;29(7):687-90. DOI: http://dx.doi.org/10.1016/S0305-4179(03)00071-8
2. 2012 National Burn Repositoy. Report of Data from 2002-2011. Chicago: American Burn Association; 2012.
3. Keck M, Lumenta DB, Andel H, Kamolz LP, Frey M. Burn treatment in the elderly. Burns. 2009;35(8):1071-9. DOI: http://dx.doi.org/10.1016/j.burns.2009.03.004
4. Chang EJ, Edelman LS, Morris SE, Saffle JR. Gender influences on burn outcomes in the elderly. Burns. 2005;31(1):315. DOI: http://dx.doi.org/10.1016/j.burns.2004.07.011
5. Pomahac B, Matros E, Semel M, Chan RK, Rogers SO, Demling R, et al. Predictors of survival and length of stay in burn patients older than 80 years of age: does age really matter? J Burn Care Res. 2006;27(3):265-9. DOI: http://dx.doi.org/10.1097/01.BCR.0000216795.90646.4E
6. Lumenta DB, Hautier A, Desouches C, Gouvernet J, Giorgi R, Manelli JC, et al. Mortality and morbidity among elderly people with burns-evaluation of data on admission. Burns. 2008;34(7):965-74. DOI: http://dx.doi.org/10.1016/j.burns.2007.12.004
7. Lionelli GT, Pickus EJ, Beckum OK, Decoursey RL, Korentager RA. A three decade analysis of factors affecting burn mortality in the elderly. Burns. 2005;31(8):958-63. DOI: http://dx.doi.org/10.1016/j.burns.2005.06.006
8. Mahar P, Wasiak J, Bailey M, Cleland H. Clinical factors affecting mortality in elderly burn patients admitted to a burns service. Burns. 2008;34(5):629-36. DOI: http://dx.doi.org/10.1016/j.burns.2007.09.006
9. Macrino S, Slater H, Aballay A, Goldfarb IW, Caushaj PF. A three-decade review of thermal injuries among the elderly at a regional burn centre. Burns. 2008;34(4):509-11. DOI: http://dx.doi.org/10.1016/j.burns.2007.06.010
10. Li X, Peng Y, Shang X, Liu S. Epidemiologic investigation of geriatric burns in Southwest China. Burns. 2009;35(5):714-8. DOI: http://dx.doi.org/10.1016/j.burns.2008.10.012
11. Ehrlich AR, Bak RY, Wald-Cagan P, Greenberg DF. Risk factors for fires and burns in homebound, urban elderly. J Burn Care Res. 2008;29(6):985-7. DOI: http://dx.doi.org/10.1097/BCR.0b013e31818ba1ab
12. Ehrlich AR, Kathpalia S, Boyarsky Y, Schechter A, Bijur P. Elderly patients discharged home from the emergency department with minor burns. Burns. 2005;31(6):717-20. DOI: http://dx.doi.org/10.1016/j.burns.2004.12.008
13. Silva GPF, Olegario NBC, Pinheiro AMRS, Bastos VPD. Estudo epidemiológico dos pacientes idosos queimados no Centro de Tratamento de Queimados do Hospital Instituto Doutor José Frota do município de Fortaleza-CE, no período de 2004 a 2008. Rev Bras Queimaduras. 2010;9(1):7-10.
14. Serra MC, Guimarães Junior LM, Sperandio A, Stoffel C, Zocrato K, Neves L, et al. Queimadura em pacientes da terceira idade: epidemiologia de 2001 a 2010. Rev Bras Queimaduras. 2011;10(4):111-3.
15. Solanki NS, Greenwood JE, Mackie IP, Kavanagh S, Penhall R. Social issues prolong elderly burn patient hospitalization. J Burn Care Res. 2011;32(3):387-91. DOI: http://dx.doi.org/10.1097/BCR.0b013e318217f90a
16. Kut A, Turk E, Tarim A, Basaran O. Burn injuries in elderly patients attending to a hospital network in turkey: a descriptive study. Burns. 2007;33(Suppl 1):S52. DOI: http://dx.doi.org/10.1016/j.burns.2006.10.124
17. Wong P, Choy VY, Ng JS, Yau TT, Yip KW, Burd A. Elderly burn prevention: a novel epidemiological approach. Burns. 2007;33(8):995-1000. DOI: http://dx.doi.org/10.1016/j.burns.2007.03.017
18. Alden NE, Bessey PQ, Rabbitts A, Hyden PJ, Yurt RW. Tap water scalds among seniors and the elderly: socio-economics and implications for prevention. Burns. 2007;33(5):666-9. DOI: http://dx.doi.org/10.1016/j.burns.2006.10.003
19. Albornoz CR, Villegas J, Sylvester M, Peña V, Bravo I. Burns are more aggressive in the elderly: proportion of deep burn area/total burn area might have a role in mortality. Burns. 2011;37(6):1058-61. PMID: 21571438 DOI: http://dx.doi.org/10.1016/j.burns.2011.03.006
20. Yin Z, Qin Z, Xin W, Gomez M, Zhenjiang L. The characteristics of elderly burns in Shanghai. Burns. 2010;36(3):430-5. DOI: http://dx.doi.org/10.1016/j.burns.2009.06.204
21. Ho WS, Ying SY, Chan HH. A study of burn injuries in the elderly in a regional burn centre. Burns. 2001;27(4):382-5. DOI: http://dx.doi.org/10.1016/S0305-4179(00)00146-7
22. Rao K, Ali SN, Moiemen NS. Aetiology and outcome of burns in the elderly. Burns. 2006;32(7):802-5. DOI: http://dx.doi.org/10.1016/j.burns.2006.03.024
23. Wibbenmeyer LA, Amelon MJ, Morgan LJ, Robinson BK, Chang PX, Lewis R 2nd, et al. Predicting survival in an elderly burn patient population. Burns. 2001;27(6):583-90. DOI: http://dx.doi.org/10.1016/S0305-4179(01)00009-2
24. Morita S, Higami S, Yamagiwa T, Iizuka S, Nakagawa Y, Yamamoto I, et al. Characteristics of elderly Japanese patients with severe burns. Burns. 2010;36(7):1116-21. DOI: http://dx.doi.org/10.1016/j.burns.2010.02.006
25. Liu Y, Chen JJ, Crook N, Yu R, Xu XW, Cen Y. Epidemiologic investigation of burns in the elderly in Sichuan Province. Burns. 2013;39(3):389-94. DOI: http://dx.doi.org/10.1016/j.burns.2012.04.012
26. Redlick F, Cooke A, Gomez M, Banfield J, Cartotto RC, Fish JS. A survey of risk factors for burns in the elderly and prevention strategies. J Burn Care Rehabil. 2002;23(5):351-6. DOI: http://dx.doi.org/10.1097/00004630-200209000-00009
1. Fundação de Ensino e Pesquisa em Ciências da Saúde-FEPECS, Brasília, DF, Brazil
2. Sociedade Brasileira de Cirurgia Plástica, São Paulo, SP, Brazil
3. Hospital Regional da Asa Norte-Brasília, Brasília, DF, Brazil
4. Universidade Federal do Rio de Janeiro, Rio de Janeiro, RJ, Brazil
5. Escola de Medicina da Escola de Superior de Ciências da Saúde, Brasília, DF, Brazil
6. Universidade de Brasília, Brasília, DF, Brazil
7. Comitê de Ética em Pesquisa em Seres Humanos da Secretaria de Saúde, Brasília, DF, Brazil
Institution: Hospital Regional da Asa Norte, Brasília, DF, Brazil.
Corresponding author:
Rodrigo Vieira Silva
Rua 09 Sul Lote 10, 1701, Aguas Claras
Aguas Claras, SP, Brazil Zip Code 71938-360
E-mail: rvmed13@gmail.com
Article received January 29, 2014.
Article accepted June 1, 2014.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket