



Case Report - Year 2015 - Volume 30 -
Soft tissue chondroma case report and review of the literature
Condroma de partes moles relato de caso e revisão da literatura
ABSTRACT
The present study presents a case report of extraskeletal chondroma or soft tissue chondroma, a rare and benign lesion, diagnosed by clinical findings, imaging studies and histopathological exam. The 24-year-old patient presented at the Orthopedics Section of Unimed Betim Hospital with a slow painless growth on the left thumb about 1 year ago. During the physical examination, a nodular lesion was noted; it had a hard consistency, was mobile and painless, and didn't cause functional impairment for the finger. The patient was referred to the imaging unit of the hospital, where an X-ray was performed; later on, ultrasound and magnetic resonance imaging of the left thumb was done. After the imaging studies, the medical team chose excisional biopsy of the lesion. The histopathological examination confirmed the diagnosis of extra-skeletal chondroma or soft-tissue chondroma. Soft tissue chondroma is usually not considered for a soft-tissue tumor of the hand. Excision is easy and must be complete if recurrences are to be avoided. Histopathological evaluation is required for the final diagnosis.
Keywords: Chondroma; Soft tissues neoplasm; Thumb.
RESUMO
O presente estudo tem o objetivo de apresentar um relato de caso sobre condroma extra-esquelético ou de partes moles, uma lesão rara e benigna diagnosticada através da clínica, radiologia e exame histopatológico. O paciente (24 anos) compareceu ao Setor de Ortopedia do Hospital Unimed Betim com queixa de aumento de volume no polegar esquerdo, indolor há aproximadamente um ano. Durante o exame físico verificou-se presença de uma lesão nodular, de consistência dura, móvel, indolor que não acarretava em alteração funcional do dedo. O paciente foi encaminhado para setor de radiologia do hospital onde foi realizado RX e posteriormente ultrasonografia e ressonância magnética do polegar esquerdo. Diante dos achados dos estudos de imagem a equipe optou pela biópsia excisional da lesão. O exame histopatológico confirmou o diagnóstico de condroma extra-esquelético. Os elementos definidores do condroma de partes moles são: 1) curso clinico benigno e sintomatologia frusta; 2) ausência de conexão entre o tumor e estruturas adjacentes como periosteo, capsula articular ou osso; 3) crescimento lento; 4) ausência de prevalência por sexo; 5) características radiológicas e histológicas do tumor. O diagnóstico raramente é aventado quando confrontamos tumores de partes moles das mãos. A excisão é simples e deve ser completa para se evitar recorrências. A avaliação histopatológica deve ser realizada para confirmação diagnóstica.
Palavras-chave: Condroma; Tumor benigno; Relato de caso.
Soft tissue chondromas are rare, slowly progressing benign cartilaginous tumors that probably arise from the fibrous stroma and not from mature cartilaginous or osseous tissue.1 This benign soft-tissue lesion affects hands and feet in 90% of cases, with the fingers being the most common site.2-4 They most commonly begin in middle age (between 30 and 60 years), and have an uncertain pathogenesis.3,4
Periosteal chondroma was first described by Lichtenstein and Hall in 19525, thereafter, other authors described more cases of this entity; approximately 200 cases have now been reported.6 It is obvious from the review of the literature that under the term "extraskeletal chondroma," many authors have also included juxtacortical or periosteal chondroma, a benign tumor located between bone and periosteum. Therefore, the number of cases of soft tissue chondroma is actually smaller than the number quoted.1,6 These tumors are totally independent of cartilaginous or bone structures, but since they originate from cartilaginous tissue, like osseous chondromas, they should be considered soft tissue chondroma or extraskeletal chondroma. Some authors resist this designation or simply classify them as cartilaginous cutaneous tumors that should not be confused with articular tumors, called para-articular chondromas.1,2,7
This report presents a case of a soft tissue chondroma in the left thumb, diagnosed by clinical findings, imaging studies and histopathological exam in a 24-year-old patient.
CASE REPORT
The patient, a 24-year-old man presented on March 10, 2005, at the orthopedic department of the Unimed Betim Hospital reporting an approximately 1-year history of a painless, slowly growing mass on the left thumb between the proximal and the distal phalanx.
Physical examination revealed asymmetry of the left thumb and absence of phlogistic signs. Palpation showed a nodular lesion; it had a hard consistency, was mobile and painless, and did not affect the functio of the thumb. Laboratory investigations showed no abnormality.
The patient was taken to the radiology unit for complementary exams (RX). Radiography of the left thumb revealed no significant alterations. Ultrasonography was than performed and showed in the flexor face of the thumb, in the active palpation area, adjacent to the flexor tendon, a nodular solid formation, measuring 8 x 6 mm diameter, 1.7 mm below the skin surface. The articular joints of the thumb were normal, with no signs of shedding, and the tendinous muscle transition was normal.
To increase the accuracy of the imaging diagnosis, magnetic resonance imaging was done. It revealed a small cystic lesion, measuring 7.4 x 4.8 mm, on the volar region of the left thumb. The T1-weighted image showed a hypointense signal and the fat-suppressed and T2-weighted image showed a hyperintense signal; an intense halo ring was seen after an intravenous infusion of a contrast agent. The ligament and tendinous tissue showed no pathologic signs. The interphalangeal articulation of the thumb was normal. There were no signs of intra-articular swelling or synovitis. No osseous abnormalities were seen (Figure 1).
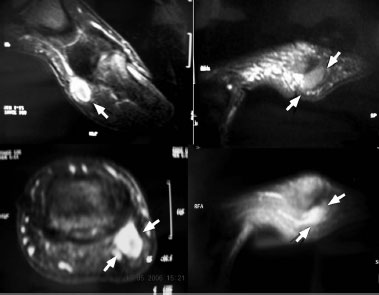
Figure 1. Small cystic formation measuring 7.4 x 4.8 mm, visible on the volar region of the left thumb (arrow). The ligament structures and tendinous tissue showed no alterations. The interphalangeal joint of the thumb showed normal aspect.
Because the patient had left thumb pain, the medical team performed excisional biopsy. The histopathological exam of the lesion revealed a small, nodular and lobulated macroscopic lesion with a grayish white color and hard consistency. The lesion featured a small section of fibroadipose tissue. The microscopic review showed a thick fibroconjuntive membrane around the cortex without any osseous tissue surrounding. The neoplasm was composed of mature adult hyaline cartilage arranged in a lobular manner (Figure 2A). In the middle of the cartilaginous matrix were multiple nests filled with large and proliferated chondrocyte cells, without atypical signs. Small myxoid areas and calcification were also seen.
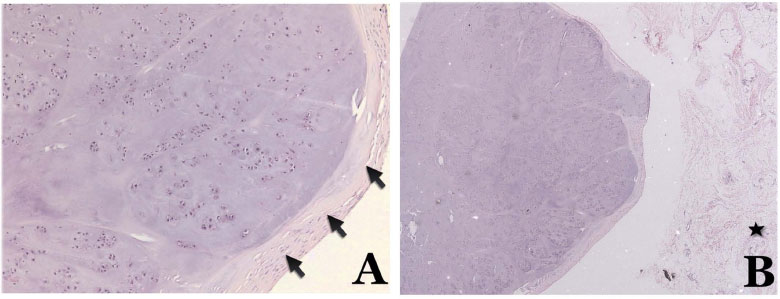
Figure 2. Chondroma. A - Detail of the previous image showing thick fibrous connective capsule (arrows) and lobules made of proliferated chondrocytes, in a cartilage matrix with calcification focus (hematoxylin-eosin [HE], 100X). B - Circumscribed nodular lesion, with lobulated aspect, surrounded by fibrofatty tissue (star) (HE - 25 X).
Several nests contained more voluminous proliferated chondrocytes, not atypical, amid the cartilage matrix (Figure 2B). Small myxoid areas and sparse calcification focus could be noted. Proliferated chondrocyte groups, not atypical, formed lobules amid the cartilage matrix. There were sparse, more voluminous and vacuolated chondrocytes (Figures 2 and 3).
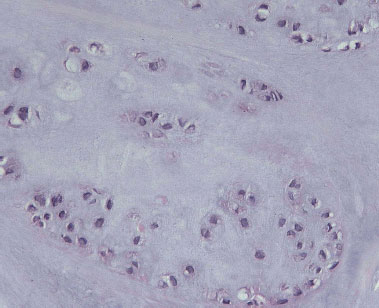
Figure 3. Chondroma. Notice groups of proliferated chondrocytes, without atypia, forming lobule, amid the cartilage matrix. Sparse, more voluminous and vacuolated chondrocytes are shown (HE - 400X).
The morphologic picture was compatible with soft tissue chondroma or extraskeletal chondroma.
DISCUSSION
Extraskeletal chondroma is a benign cartilaginous soft tissue tumor. According to Chung and Enzinger,3 the age group most affected ranges from 30 to 60 years, with no prevalence by sex. The most affected areas are mainly the upper members (72%), lower members (24%), head and neck (2%) and body (2%). The majority of studies so far reported indicate that hands are the most frequently site for this lesion.3,8 The thumb is the digit least affected, and the middle finger is the most commonly affected area.3,4 Other locations, such as kidneys, liver and tongue, have been reported.
The pathogenesis of this tumor is unclear. Several theories explain the origin of this entity in soft tissue.4 Some authors suggest that these tumors originate from the synovial sheath, whereas other authors believe in the theory of island activation of heterotopic cartilaginous tissue. The microtrauma hypothesis has also been suggested as an etiological factor. According to Kho and Chen,9 there are reports of multiple soft tissues chondroma as a result of an autosomal dominant inheritance. Recently, nonrandom clonal changes of chromosomes 6, 11 and 12 have been implicated in the etiology of soft tissue chondroma. In another study, molecular analysis showed that the gene hmga2, located at 12q15, is related to this pathology, as well as with lipoma.
The first symptom is the appearance of a small nodular lesion that gradually increases in size but rarely causes pain.1-4 The tumor rarely compresses the peripheral nerve, but there are reports of the involvement of the ulnar, radial and median nerves. On x-ray, 60% of the lesions present some degree of calcification.1,2,9 The bones around the lesion are rarely affected. Macroscopically the tumor has a diameter of approximately 3 cm or less; it is easily delimited and has a hard consistency. This tumor can attach to tendons, to joint capsules, to ligaments or to other soft tissues, but it can be easily removed and, unlike periosteal chondroma, is located outside the periosteum3,4,10.
Biopsy frequently reveals a benign lobulated cartilaginous tumor, with remarkable cellularity and prominent calcification. The histopathology is characteristic, showing cartilaginous cells with centralized zones of cellular polymorphism and proliferation of giant cells on the tumor margin. Occasionally, this tumor may present atypical morphologic characteristics, which makes the differential diagnosis with malignant lesions difficult.2,11
The differential diagnosis of the extra-osseous chondroma must be done with other tumors that have similar characteristics but different clinical behavior. The most important conditions are chondroblastoma, juxtacortical chondrosarcoma, osteochondroma, synovial chondromatosis and, sometimes, juxtacortical chondromyxoid fibroma, periosteal desmoid tumor and tumoral calcinosis.8,11
Although some of the chondroblastoma forms of extra-osseous chondromas may be of interest because of their atypical cellular characteristics, there is no evidence in the literature that these tumors behave differently from the well-differentiated forms composed of mature hyaline cartilage.1 So it is remarkable that the transformation of the extra-osseous chondroma into chondrosarcoma has not been described before now; however, this is rare in the chondroid lesions of the bone.1 Complete excision is recommended according to the literature.1-4,9 Primary biopsy is contraindicated.12 The recurrence rate is 18%, mainly due to incomplete resection of the lesion.3
In summary, the defining elements of the extra-osseous chondroma or soft tissue chondroma are 1) benign and asymptomatic clinical course; 2) absence of connection between the tumor and the adjacent structures, such as the periosteum, joint capsules or bone; 3) slow tumor growth; 4) absence of prevalence among sex; 5) specific histological and radiological characteristics. The diagnosis of soft-tissue chondroma is usually not considered for a soft-tissue tumor of the hand. Excision is easy and must be complete if recurrences are to be avoided. Histopathological evaluation is required for the final diagnosis.
REFERENCES
1. Anthouli-Anagnostopoulou FA, Papachristou G. Extraskeletal chondroma, a rare soft tissue tumor. Case report. Acta Orthop Belg. 2000;66(4):402-4. PMID: 11103495
2. Saito N, Horiuchi H, Toriumi H, Miyasaka T. Extraskeletal chondroma of the hand accompanied by proliferating chondroblast-like cells with an eleven-year follow-up. Case Rep Clin Pract Rev. 2003;4(2):66-8.
3. Chung EB, Enzinger FM. Chondroma of soft parts. Cancer. 1978;41(4):1414-24. PMID: 76505 DOI: http://dx.doi.org/10.1002/1097-0142(197804)41:4<1414::AID-CNCR2820410429>3.0.CO;2-O
4. Khedhaier A, Maalla R, Ennouri K, Regaya N. Soft tissues chondromas of the hand: a report of five cases. Acta Orthop Belg. 2007;73(4):458-61. PMID: 17939475
5. Lichtenstein L, Hall JE. Periosteal chondroma; a distinctive benign cartilage tumor. J Bone Joint Surg Am. 1952;24 A(3):691-7. PMID: 14946224
6. Lewis MM, Kenan S, Yabut SM, Norman A, Steiner G. Periosteal chondroma. A report of ten cases and review of the literature. Clin Orthop Relat Res. 1990;(256):185-92. DOI: http://dx.doi.org/10.1097/00003086-199007000-00027
7. Enzinger FM, Weiss SW. Cartilaginous tumors and tumorlike lesions of soft tissue. In: Enzinger FM, Weiss SW, eds. Soft Tissue Tumors. St. Louis: CV Mosby; 1983. p.698-705.
8. Suganuma S, Tada K, Tsuchiya H. Giant extraskeletal chondroma of the index finger: a case report. J Plast Reconstr Aesthet Surg. 2011;64(10):1377-9. PMID: 21440522 DOI: http://dx.doi.org/10.1016/j.bjps.2011.02.024
9. Kho VK, Chen WC. Extraskeletal osteochondroma of the foot. J Chin Med Assoc. 2010;73(1):52-5. DOI: http://dx.doi.org/10.1016/S1726-4901(10)70023-X
10. De Smet L. Posterior interosseous neuropathy due to compression by a soft tissue chondroma of the elbow. Acta Neurol Belg. 2005;105(2):86-8. PMID: 16076062
11. Cates JM, Rosenberg AE, O'Connell JX, Nielsen GP. Chondroblastoma-like chondroma of soft tissue: an underrecognized variant and its differential diagnosis. Am J Surg Pathol. 2001;25(5):661-6. DOI: http://dx.doi.org/10.1097/00000478-200105000-00015
12. Fnini S, Sennoune B, Zamiati S, Ouarab M, Largab A, Trafeh M. Soft-tissue chondroma of the hand. A new case. Chir Main. 2004;23(3):153-6. DOI: http://dx.doi.org/10.1016/j.main.2004.04.008
1. Sociedade Brasileira de Cirurgia de Mão, São Paulo, SP, Brazil
2. Hospital Geral Governador Israel Pinheiro, Belo Horizonte, MG, Brazil
3. Hospital Unimed Betim, Betim, MG, Brazil
4. Sociedade Brasileira de Cirurgia Plástica, São Paulo, SP, Brazil
5. Hospital Unimed BH, Belo Horizonte, MG, Brazil
6. Biocor Instituto, Nova Lima, MG, Brazil
7. Hospital Vera Cruz, Belo Horizonte, MG, Brazil
8. IMOP - Instituto de Mastologia, odontologia e cirurgia plástica, Belo Horizonte, MG, Brazil
Institution: Unimed Betim Hospital, Betim, MG, Brazil.
Corresponding author:
Gustavo Augusto Matos Saliba
Rua Raul Saraiva Ribeiro, 633
Betim, MG, Brazil Zip Code 32610-320
E-mail: salibagustavo@yahoo.com.br
Article received April 23, 2012.
Article accepted July 1, 2012.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket