



Special Article - Year 2015 - Volume 30 -
The reverse adipofascial thenar flap for coverage of the hypertrophied median nerve in macrodactyly
Retalho tenar adipofascial reverso para cobertura do nervo mediano hipertrofiado em macrodactilia
ABSTRACT
Macrodactyly is a rare congenital anomaly characterized by the disproportionate growth of bone, fat, nervous, vascular, and dermal tissue in the digits . There are many different theories about its etiopathogenesis, the most accepted being a hyperstimulation by growth factors conducted through nerves. A few cases have been described in conjunction with carpal tunnel syndrome. Here, a clinical case of carpal tunnel syndrome due to hypertrophy of the median nerve is presented, showing an increase of content within the flexor retinaculum. Successful surgical treatment was accomplished by conducting a retinaculotomy of the anterior annular ligament along with a reverse transposition adipofascial flap of the hypertrophied thenar region for coverage of the median nerve at the wrist.
Keywords: Hypertrophy; Hands; Congenital abnormalities; Gigantism; Reconstructive surgical procedures.
RESUMO
A macrodactilia é uma anomalia congênita infrequente, caracterizada pelo crescimento desproporcional dos tecidos ósseo, gorduroso, nervoso, vascular e dérmico nos dedos das mãos ou dos pés. Existem muitas teorias sobre a sua etiopatogenia, sendo a mais aceita a hiperestimulação por fatores de crescimento enviados através dos nervos. Foram descritos alguns casos associados com a síndrome do túnel do carpo. Apresenta-se um caso clínico de síndrome do túnel do carpo por hipertrofia do nervo mediano, evidenciando um aumento de conteúdo dentro do retináculo flexor, o qual foi tratado cirurgicamente com sucesso pela realização de uma retinaculotomia do ligamento anular do carpo junto a um retalho de transposição tenar adipofascial reverso da região tenariana hipertrofiada visando à cobertura do nervo mediano na região do punho.
Palavras-chave: Hipertrofia; Mãos; Anomalias congênitas; Gigantismo; Procedimentos cirúrgicos reconstrutivos.
Definition and Epidemiology
Macrodactyly, also called digital gigantism1, is a rare condition of unknown origin, in which genetic inheritance has no important role2,3. The term macrodactyly refers to the hypertrophy of one or multiple digits of the hand or foot. It affects all digital mesenchymal structures, such as skin, fat, nails, nerves, tendons, blood vessels, and bone tissue1-7. According to Barski (1967) and Tuli et al. (1969), this condition does not affect the bones of the metacarpus or metatarsus, although their involvement has been described by some authors8. All types of digital hypertrophies secondary to hemangiomas or other tumor processes must be discarded during the evaluation4.
The first cases of macrodactyly were described by Von Klein, in 18249,10 and then by Feriz, in 1925, with the designation of partial gigantism of the lower extremity5.
The frequency with which macrodactyly presents is very low, as Barski demonstrated in a study of cases observed over 140 years4. Kotal and Farooque6 note that the condition represents 0.9% of all congenital abnormalities.
The disease presents with greatefr frequency in men, in the right hand, index and middle fingers, affects two fingers in 60% of cases, associates with syndactyly in 10% and is bilateral in 5% of cases4-6. When it presents tardily, the symptoms are related to nerve compression9. Dennyson et al. more frequently observed an impairment of the hand than the foot in macrodactyly3.
Etiopathogenesis
The most accepted theory is that there is a nerve anomaly, which produces a cellular hyperstimulation in the innervation areas4,5,8,11,12. Another possible cause of this malformation is abnormal blood and humoral supply to the nerve, which would eventually stimulate tissue overgrowth5,9. Kalen et al. described the growth of the nerve in 90% of cases with the hand affected, and Boren et al. designated this phenomenon as "nerve territory-oriented macrodactyly"5. Inglis suggested that growth is influenced by intrinsic factors of neurofibromatosis acting locally3.
The patients present with joint stiffness, ulceration of the fingertips, trigger finger, pain, and paresthesia9. The nerves thicken and become tortuous, which may lead to carpal tunnel syndrome (CTS)13. CTS caused by hypertrophy of the median nerve in macrodactyly has been described by some authors9 and is considered a late complication of the disease13,14. This can present concomitantly with tumors of the nerve, such as hamartomas15,16 or macrodystrophia lipomatosa17.
Classification
Clinically, the disorder may be classified as either static macrodactyly, present since birth and with proportional growth, or as progressive macrodactyly, which is more frequent and is characterized by faster development of the affected fingers and angular deformity4,9.
Another possible classification of this disease is symmetric macrodactyly, in which all digital elements are changed similarly, or as asymmetric macrodactyly, in which hypertrophy of fat tissue and bone occurs. Richardiere described the condition as true or false macrodactyly if growth is regular or irregular, respectively4.
Clinical and anatomical features are also used to differentiate patients by using the terms "lipomatous" for those with accentuated growth of adipose tissue with a lower degree of neural growth, and "guided by the innervation path" for those with coarsely extended nerves that are infiltrated with fat and positioned inside or adjacent to the area of excessive growth7,11.
Treatment
There is no medical or surgical treatment that offers fully satisfactory results for macrodactyly. Many surgical techniques have been described to reduce the size of the digit: dermolipectomy, reductive osteotomy of phalanges, and epiphysiodesis. Phalangectomy has also been reported to reduce the length of the digit6, but often results in digital amputation9.
A surgical procedure proposed by Barsky11 involves digital shortening and preservation of the fingernail-a good option in the case of enlarged digital pulps. In the procedure described by Tsuge12, the digital pulp is reduced and the skin is removed longitudinally from the side of the finger. This technique can be used in moderate cases because there is no bone removal.
The surgical procedure proposed by Bertelli et al.18 for the treatment of macrodactyly basically involves en bloc hemidigital resection with collateral ligament transplantation to the proximal interphalangeal articulation. After six months, the patient is subjected to another surgical procedure on the contralateral side of the digit. The digital artery and the nerve are preserved. With this procedure, the sensitivity, active motion, and stability of the proximal interphalangeal joint are also preserved.
Akinci et al.1 described a surgical technique that involves calculating the amount of tissue required to coat a normal-sized finger, using the same finger of the opposite hand as a reference. This reveals the amount of tissue that is necessary on the digit that is to be operated upon. The dimensions of the nail are delimited by a reconstruction of the lateral area of the nail bed by flaps. There is a narrowing of the distal phalangeal joint. The tendons of the extensor and flexor muscles are left intact.
Indications for digital transposition include a severely affected middle finger with a usable index finger7.
Procedures for coverage of the median nerve
The decompression of the carpal tunnel by canal narrowing is performed by open surgery or with the use of endoscopic methods. Complications are rare but can occur with both techniques19,20. In the cases of CTS caused by macrodactyly, decompression can also be performed by endoscopic surgery21.
Several surgical procedures have been described to protect the median nerve and these are typically used in cases of recalcitrant CTS. Among them are adipose flaps of the hypothenar region, reverse adipofascial flaps based on the radial artery, muscular flaps of the pronator quadratus muscle, little finger abductor muscle, and palmar brevis muscle, in addition to free or pedicled flaps from the forearm19,20,22. Noor et al.22 described an adipofascial flap based on perforating branches of the ulnar artery as an alternative. Reverse adipofascial flaps based on perforating branches of the ulnar artery or of the radial artery of the forearm region are efficient in covering defects in the wrist, with the advantage of being esthetically pleasing23.
If there is fibrous proliferation around the median nerve, coverage of the nerve by soft tissues is recommended to prevent the formation of scars on the anterior face of the nerve and in other regions of the carpus. When the nerve is very fibrous, the entire circumference of the nerve should be involved, to isolate it from the flexor tendons and adjacent skin, thus increasing its vascularization19.
The hypothenar flap is irrigated by the ulnar artery, which traverses the Guyon canal. This type of flap has easy mobility for covering the surface of the median nerve in the distal forearm. The procedure can be performed under local or general anesthesia. The Guyon canal is sectioned and adipose tissue is dissected until the hypothenar muscles and palmar brevis muscle are identified. The flap is raised and transposed in the radial direction and may be transferred to the median nerve and housed in the radial wall of the carpal canal by measuring the tension on the pedicle24,25.
There are few reported cases describing the application of flaps of the thenar region in pediatric patients. The indications for this type of flap are generally lesions in the phalanges with bone involvement and without disruption of nerves or tendons. The flap is constructed from the skin of the thenar region, being dissected in a subcutaneous plane from the distal part to the proximal part26.
There is no description of thenar flaps for coverage of the median nerve.
METHOD
We conducted a review of the literature about macrodactyly and the surgical techniques for coverage of the median nerve. A reverse adipofascial thenar flap for coverage of the hypertrophied median nerve is described.
CLINICAL CASE
We present the case of a 14-year-old boy without a family history of congenital malformations. He was diagnosed with progressive macrodactyly and underwent dermolipectomy of the first right digit at the age of 9 years. Upon consultation, symptoms and signs of compression of the median nerve at the wrist, confirmed on electroneuromyography, led to a diagnosis of CTS. (MNE: findings compatible with CTS of very serious intensity on the right side, without associated cervical radiculopathy.)
Retinaculotomy of the flexors was performed under general anesthesia. During the operation, a hypertrophied median nerve was observed (Figure 1) and soon after the opening of the anterior annular ligament, the most anterior portion of the nerve (1/3 anterior circumference of the nerve) was released from the canal.
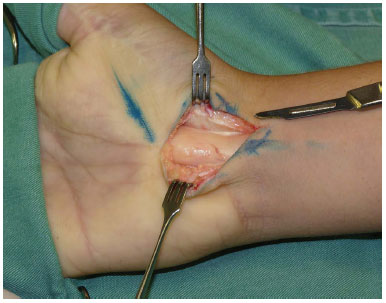
Figure 1. Hypertrophy of the median nerve and opening of the flexor retinaculum.
Before skin suture, we observed that the coverage of the median nerve at the wrist would be incomplete with only the skin and a thin layer of subcutaneous tissue, leaving the nerve too exposed.
A reverse adipofascial transposition flap was chosen, making use of the hypertrophy of the subcutaneous cellular tissue of the thenar region caused by macrodactyly. A distal extension of the incision was held together by constructing the adipofascial flap with a proximal pedicle, while maintaining an adequate thickness to prevent skin necrosis of the thenar region (Figure 2).

Figure 2. Transposition of the reverse adipofascial flap of the thenar region.
The dissection plane extended to the thenar muscles with posterior retrograde transposition of the flap to cover the hypertrophied median nerve (Figure 3), in addition to posterior coverage with the skin of the wrist.

Figure 3. Good coverage of the median nerve by the flap.
RESULTS
The patient progressed satisfactorily after surgery, reporting a progressive improvement of the symptoms associated with median nerve compression (Figures 4 to 6).

Figure 4. Result 7 days after surgery.

Figure 5. Functional outcome after 6 months of surgery (clamp).

Figure 6. Functional outcome after 6 months of surgery (opposition).
DISCUSSION
CTS is one of the most frequent pathologies within the hand surgery specialty. First described by Paget and then studied in depth by Phalen, the etiopathogenesis is based on the reduction of the canal (anterior annular ligament or flexor retinaculum), which produces a compression on the content (median nerve), thus resulting in the characteristic symptoms of the disease27.
However, few cases have been described wherein the situation reverts, such that the contents within the carpal canal are increased. The compression can be a consequence of synovial hypertrophy, rheumatism, amyloidosis, presence of abnormal supernumerary muscles inside the canal, and hypertrophy of the artery of the median nerve, among other factors. Typically, the literature describes cases of intrinsic growth of the nerve due to tumors or infiltrative growth27.
In cases with signs of recalcitrant nervous compression, a few techniques have been described to protect the median nerve, such as the synovial flap, hypothenar adipose flap, pedicled flaps, or the use of biomaterials28.
The particular features of macrodactyly in the case presented here are consistent with those described in the literature: more frequent in men and in the right hand when in its progressive form, with more frequent nerve impairment when affecting the hand. However, although the disease generally affects the second and third digits, the case described involves the thumb.
The most accepted theory for the development of macrodactyly is the hyperstimulation of tissue by growth factors conducted through nerves. In the case described here, despite the total hypertrophy of the median nerve, the patient only presented hypertrophy of the thumb, without impairment of all the digits innervated by the median nerve. This strengthens the idea, as has been stated by some authors, that multiple intrinsic and environmental factors are required to cause the disease or that only some nerve fascicles are affected.
During the surgical procedure, in addition to retinaculotomy, we took advantage of the hypertrophy that was presented in the fatty tissue of the thenar region to construct an adipofascial thenar flap with a proximal pedicle in order to cover the median nerve (and not leave it covered exclusively by the anterior skin of the wrist). This decreases the postoperative morbidity related to wrist trauma in the area of the median nerve.
CONCLUSIONS
We present a case of CTS caused by median nerve hypertrophy associated with progressive macrodactyly of the thumb that was successfully treated surgically, with an opening of the carpal canal and using a reverse adipofascial thenar flap to protect the median nerve.
REFERENCES
1. Akinci M, Ay S, Erçetin O. Surgical treatment of macrodactyly in older children and adults. J Hand Surg Am. 2004;29(6):1010-9. DOI: http://dx.doi.org/10.1016/j.jhsa.2004.07.004
2. Lagoutaris ED, DiDomenico LA, Haber LL. Early surgical repair of macrodactyly. J Am Podiatr Med Assoc. 2004;94(5):499-501. DOI: http://dx.doi.org/10.7547/0940499
3. Syed A, Sherwani R, Azam Q, Haque F, Akhter K. Congenital macrodactyly: a clinical study. Acta Orthop Belg. 2005;71(4):399-404. PMID: 16184993
4. Martín García JA, Molina Carballo A, Hernández Gomez MV, López Moratalla M. Macrodactilia. Aportación de un caso y consideraciones anatomopatológicas, clínicas y terapéuticas. Rev Esp Cir Osteoarticular. 1987;21:411-9.
5. Khan F, Asif SA, Khan NU, Ullah I, Ullah F. Our experience with macrodactyly: a rare congenital anomaly. Pak J Surg. 2010;26(3):242-5.
6. Kotwal PP, Farooque M. Macrodactyly. J Bone Joint Surg Br. 1998;80(4):651-3. DOI: http://dx.doi.org/10.1302/0301-620X.80B4.8489
7. Carrato F, Eberlin K, Waters P, Upton J, Taghinia A, Labow BI. Presentation and treatment of macrodactyly in children. J Hand Surg. 2013;38(11):2112-23.
8. Kalen V, Burwell DS, Omer GE. Macrodactyly of the hands and feet. J Pediatr Orthop. 1988;8(3):311-5. DOI: http://dx.doi.org/10.1097/01241398-198805000-00011
9. Batista KT, Cauhi AF, Almeida CEF, Araújo EA, Jesus GAB, Araújo HJ, et al. Macrodactilia na mão: relato de um caso. Rev Bras Cir Plast. 2008;23(2):128-30.
10. Klein V, Germann G, Bosse A, Müller KM, Steinau HU. Clinical aspects, morphology and therapy of an unusual case of bilateral macrodactyly. Handchir Mikrochir Plast Chir. 1993;25(1):12-9.
11. Barsky A. Macrodactyly. J Bone Joint Surg Am. 1967;49(7):1255-66. PMID: 4293291
12. Tsuge K. Treatment of macrodactyly. Plast Reconstr Surg. 1967;39(6):590-9. PMID: 6025687 DOI: http://dx.doi.org/10.1097/00006534-196706000-00008
13. Mirza MA, King ET, Reinhart MK. Carpal tunnel syndrome associated with macrodactyly. J Hand Surg Br. 1998;23(5):609-10. PMID: 9821604 DOI: http://dx.doi.org/10.1016/S0266-7681(98)80012-0
14. Ganske JG. Enlarged median nerve of macrodactyly associated with carpal tunnel syndrome. Iowa Med. 1986;76(8):364-5. PMID: 3759375
15. Dogan A, Kalender AM, Atik B, Karabulut S, Sebik A. Giant clinodactyly and macrodactyly of the hand associated with carpal tunnel syndrome. J Plast Surg Hand Surg. 2014;48(6):432-3. PMID: 25399959 DOI: http://dx.doi.org/10.3109/2000656X.2013.812762
16. Lorenzoni PJ, Lange MC, Kay CSK, Silvado CE, Scola RH, Werneck LC. Hamartoma fibromatoso de nervo mediano. Arq Neuropsiquiatr. 2005;63(3):881-4. DOI: http://dx.doi.org/10.1590/S0004-282X2005000500033
17. Mantadakis E, Deftereos S, Sivridis E, Michailidis L, Chatzimichael A, Prassopoulos P. Macrodactyly of the right ring finger due to macrodystrophia lipomatosa: Pathologic and imaging characteristics. Int J Case Rep Image. 2011;2(4):6-10. DOI: http://dx.doi.org/10.5348/ijcri-2011-04-27-CR-2
18. Bertelli JA, Pigozzi L, Pereima M. Hemidigital resection with collateral ligament transplantation in the treatment of macrodactyly: a case report. J Hand Surg Am. 2001;26(4):623-7. DOI: http://dx.doi.org/10.1053/jhsu.2001.26195
19. Jones NF, Ahn HC, Eo S. Revision surgery for persistent and recurrent carpal tunnel syndrome and for failed carpal tunnel release. Plast Reconstr Surg. 2012;129(3):683-92. PMID: 22090245 DOI: http://dx.doi.org/10.1097/PRS.0b013e3182402c37
20. Soltani AM, Allan, BJ, Best MJ, Mir HS, Panthaki ZJ. A systematic review of the literature on the outcomes of treatment for recurrent and persistent carpal tunnel syndrome. Plast Reconstr Surg. 2013;132(1):114-21. DOI: http://dx.doi.org/10.1097/PRS.0b013e318290faba
21. Yoshida A, Okutsu I, Hamanaka I, Morimoto S. Two cases of endoscopic management of carpal tunnel syndrome in macrodactyly patients. Hand Surg. 2007;12(1):41-6. DOI: http://dx.doi.org/10.1142/S0218810407003353
22. Noor S, Rajaratnam V, Jose R. The adipofascial flap based on an ulnar artery perforator: an alternative option for recurrent carpal tunnel syndrome. Hand Surg Eur Vol. 2012;37(9):895. DOI: http://dx.doi.org/10.1177/1753193412439827
23. Ignatiadis IA, Xeinis SF, Tsiamba VA, Yiannakopoulos CK, Nomikos GN, Gerostathopoulos NE. Distal radial and ulnar arteries perforator-based adipofascial flaps for covering hand traumatic defects. Microsurgery. 2007;27(5):372-8. DOI: http://dx.doi.org/10.1002/micr.20374
24. Tollestrup T, Berg C, Netscher D. Management of distal traumatic median nerve painful neuromas and recurrent carpal tunnel syndrome: hypothenar fat pad flap. J Hand Surg Am. 2010;35(6):1010-4. DOI: http://dx.doi.org/10.1016/j.jhsa.2010.03.035
25. Stickland JW, Idler RS, Lourie GM, Plancher KD. The hipothenar fat pad flap for management of recalcitrant carpal tunnel syndrome. J Hand Surg Am. 1996;21(5):840-8.
26. Barr JS, Chu MW, Thanik V, Sharma S. Pediatric thenar flaps: a modified design, case series and review of the literature. J Pediatr Surg. 2014;49(9):1433-8. PMID: 25148754 DOI: http://dx.doi.org/10.1016/j.jpedsurg.2013.11.066
27. Chammas M, Boretto J, Burmann LM, Matta RM, Santos Neto FC, Silva JB. Síndrome do túnel do carpo - Parte I (anatomia, fisiologia, etiologia e diagnóstico. Rev Bras Ortop. 2014;49(5):429-36. DOI: http://dx.doi.org/10.1016/j.rbo.2013.08.007
28. Chammas M, Boretto J, Burmann LM, Matta RM, Santos Neto FC, Silva JB. Síndrome do túnel do carpo - Parte II (tratamento). Rev Bras Ortop. 2014;49(5):437-45. DOI: http://dx.doi.org/10.1016/j.rbo.2013.08.008
1. Serviço de Cirurgia Plástica do Hospital São Lucas da PUC-RS, Porto Alegre, RS, Brazil
2. Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, RS, Brazil
3. Serviço de Cirurgia da Mão e Microcirurgia Reconstrutiva do Hospital São Lucas da PUC-RS, Porto Alegre, RS, Brazil
Institution: Serviço de Cirurgia da Mão e Microcirurgia Reconstrutiva, Hospital São Lucas, Pontifícia Universidade Católica do Rio Grande do Sul. Porto Alegre Porto Alegre, Rio Grande do Sul, Brazil.
Corresponding author:
Renato Franz Matta Ramos
Av. Ipiranga, 6690
Porto Alegre, RS, Brazil Zip Code 90610-000
E-mail: renatomatta82@hotmail.com
Article received: February 25, 2015.
Article accepted: April 22, 2015.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket