



Original Article - Year 2016 - Volume 31 -
Modification in Webster technique for lower lip reconstruction, using bilateral nasolabial flaps to improve reconstruction of vermilion
Modificação na técnica de Webster para reconstrução total de lábio inferior, com uso da pele da região nasogeniana para aumentar o volume do vermelhão
ABSTRACT
INTRODUCTION: Many authors consider the Bernard technique modified by Webster the first choice for total lower lip reconstruction. This technique preserves skin folds and anatomical landmarks on the face, and interferes minimally with the tactile sensibility of the reconstructed lip, resulting in satisfying cosmetic and functional outcomes. Despite agreeing with the principles of the Webster technique, a modification is proposed to improve reconstruction of vermilion, by using bilateral nasolabial flaps associated with the original advancement flaps.
METHODS: We report five surgical cases carried out between 2003 and 2008, and discussion of results.
RESULTS: Dissection need to advance flaps in Bernard-Webster technique does not make nasolabial flaps unviable, and they can be rotated properly to add volume and skin to the reconstructed vermilion.
CONCLUSION: Proposed modification of Bernard-Webster technique does not increase risk or damage compared with classic technique, and it maintains the same reconstructive capabilities or even enhances it.
Keywords: Lip/Surgery; Reconstructive surgical procedures; Surgical flaps.
RESUMO
INTRODUÇÃO: A técnica de Bernard modificada por Webster é considerada por diversos autores a primeira escolha para reconstrução total de lábio inferior. Ela preserva as linhas e pontos de referência estética da face, e proporciona boa sensibilidade no lábio reconstruído, permitindo alcançar resultados estéticos e funcionais satisfatórios. Apesar de concordar com os princípios da técnica de Webster, uma modificação é proposta visando aperfeiçoar a reconstrução do vermelhão, usando retalhos nasogenianos bilaterais associados aos retalhos de avançamento originais.
MÉTODOS: São apresentados cinco casos operados pelo autor no período de 2003 a 2008, e os resultados são discutidos.
RESULTADOS: Demonstrou-se que a dissecção necessária para avançar os retalhos da bochecha na técnica de Bernard-Webster não inviabiliza os retalhos nasogenianos, e estes podem ser rotados adequadamente para acrescentar pele e volume ao vermelhão reconstruído.
CONCLUSÃO: A modificação proposta não impõe risco aumentado ou prejuízo sobre a técnica original, e mantém ou aumenta a sua capacidade reconstrutiva.
Palavras-chave: Reconstrução de lábio inferior; Técnica de Webster; Retalhos nasogenianos.
The loss of lower lip tissue may occur due to trauma, infectious diseases or vasculitis. In most cases, however, they are secondary to tumor resection. The main goal of the lower lip reconstruction is to obtain tissue with motor function and tactile sensibility, maintain the oral competence with enough depth of the gengivolabial groove, and allow sufficient mouth opening. Besides, it is important to preserve aesthetic reference points and lines on the face such as oral commissure position, nasolabial fold and labiomental crease1.
A variety of techniques for partial or total reconstruction of lower lip have been described with varying degrees of success using local tissue, distant flaps or microvascular free flaps1. Many authors consider that distant and free flaps should be used for extensive damages, comprising ,more than lower lip limits, because they frequently provide excessively bulky tissue with unmatched color and texture2. The Bernard techniques (1853) modified by Webster in 19603 are particularly interesting for total reconstructions of the lower lip. This technique employs advancement cheek flaps, with tissue resection along the nasolabial fold such as Burow's triangles, placing incisions in accordance with the lines of aesthetic reference of the face.
Despite Webster technique3 allows good functional and aesthetic results, good sensibility and motor functions of the reconstructed lip, minute improvements have been added in publications, for example, more careful dissection of the remaining orbicular muscle and its advancement, which avoid it sectioning1,4. Another minor improvement has been the slightly downwards positioning of the horizontal incision line along the commissure, as described by Konstantinovic2, bringing about more natural-looking results. However, the Bernard principles modified by Webster are still accepted, and most authors consider this technique the first option in total or near-total lower lip reconstruction1,2,4,5.
In 2003, Rudkin et al.6 published an article reporting their experience using bilateral nasolabial flaps to completely reconstruct the lower lip. At that time, the excellent results had drawn the attention, particularly when the tissue resection presented great horizontal extension on the vermillion and little vertical extension. These results supported the appearance of the idea to combine Webster advancement flaps with bilateral nasolabial flaps. This idea goal was to maintain good results of the traditional Webster technique and add volume (skin and projection) to the vermillion by using nasolabial flaps.
Commenting on Rudkin et al. manuscript (published in April 2004 as "brief communication") we suggested: "An interesting idea to modify the Bernard-Webster technique would be to preserve nasolabial skin and subcutaneous tissue, and rotate it as additional flaps to improve the vermillion reconstuction."7.
OBJECTIVE
To describe and analyze results obtained from the technique idealized in 20037, based on the Bernard-Webster principles, but, at the same time, preserving and rotating bilaterally the nasolabial tissue to function as additional flaps in order to improve the vermilion reconstruction.
METHODS
We included five patients who underwent, from 2003 to 2008, total lower lip reconstruction using the modified Webster technique. Four patients underwent reconstruction at the same time of tumor resection, and the fifth patient was submitted to a secondary procedure about six months after jaw reconstruction using pectoralis major myocutaneous flap and a mandibular reconstruction plate.
Surgical technique
The planning of the advancement flaps and nasolabial flaps may be seen in the pre-surgical outline of cases presented in this study (Figure 1). Medial limit of the nasolabial flap must be medially dislocated in the lower part towards oral commissure. The initial dissection must include the nasolabial flaps along with the advancement flaps. Dissection of muscular plane and oral mucosa follows the same principles of the Webster technique, as well as the closing by planes, starting with the mucosa.

Figure 1. Case 1 - A 65-year-old man with recurrent squamous cell carcinoma on the central lower lip, without ulcer. A wide resection with cervical lymphadenectomy was carried out before reconstruction. Subsequently preoperative reconstruction was planned. Transoperative aspect and results about 1 month after the first surgical time (posteriorly, retouching of scar was done).
To use oral mucosa flaps to reconstruct the vermillion is not necessary because the nasolabial skin flaps are enough for the reconstruction. The nasolabial flaps are outlined to cross the median line, and be overlap on the central part of the lip. After suture, near to the end of surgery, the skin excess at the base of the nasolabial flaps is removed to define the lower and lateral limits of the vermilion and avoid volume excess at flap folds. This suture line, over the base of the nasolabial flaps, must be superficial to not compromise its vascularization.
RESULTS
We report four cases of total lower lip reconstruction done immediately after oncological resection. In these four cases (Figures 1 and 4) the pre-operative, plan and post-operative of single surgery is shown of a single surgical time, even though complementary secondary procedures may have been planned. All oncologic surgeries were performed by head-and-neck surgeon.
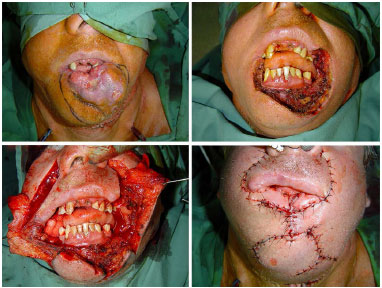
Figure 2. Case 2 - A 42-year-old man with ulcerated and extensive squamous cell carcinoma. Preopeative period. Oncological resection encompassing right oral commissure until left cheek (an cervical lymphadenectomy was carried out through submandibular incision), wide dissection of three planes - skin, muscle and mucosa, final aspect of the surgery.

Figure 3. Case 3 - A 48-year-old woman immediately after recurrent squamous cell carcinoma resection, result after 14 days, and result 2 months later. Posteriorly, a retouching was planned to reduce volume excess in the reconstructed vermilion.

Figure 4. Case 4 - A 59-year-old woman with recurrent squamous cell carcinoma resection in vermilion. Surgical planning, aspect immediately after oncological resection, wide dissection of three planes, final aspect of the surgery, and result after 2 months and a half. Posteriorly, a retouching of scar was planned and adjustment of right reconstructed vermilion limits to the right.
In the fifth case (Figure 5), different of previous ones, the lower lip reconstruction was carried out to improve the previous surgery. The patient had undergone mandibulectomy to treat squamous cell carcinoma on the lower lip, reconstruct pectoralis major myocutaneous flap and mandibular reconstruction plate. The previous surgery allowed to adequate cover the metallic plate, however, there were undefined anatomical contours of the lower lip and chin, lack of vermilion and oral incontinence - this situation was presented before the second surgery.

Figure 5. Case 5 - A 73-year-old woman who had previously undergone mandibulectomy to treat squamous cell carcinoma on the lower lip, reconstruct pectoralis major myocutaneous flap, and mandibular reconstruction plate. In preoperative we observed an excessive volume and thickness of the flap, identification of anatomic contours of lower limb and mento , lack of vermilion, and oral incontinence. In addition, she had cervical scar retractions and volume caused by the pectoralis pedicle flap. Surgery was planned to define aesthetical reference lines on the face, reconstruction of vermilion, improve of oral continence, and also to treat cervical region. Result after surgery and 3 months later.
DISCUSSION
Our patients had different stages of the same disease: squamous cell carcinoma of the lower lip. This region is prone to aggression by physical agents, particularly to sun exposure and chemical agents, such as tobacco, which makes neoplasia more probable1. We may consider social aspects involved is some cases and problems with access to adequate healthcare as contributing factors for worsening the disease8. Another contributing factor, which worsened the cases in this series, was the incidence of tumor recurrence that required a more aggressive treatment.
The modified Webster technique proposed in this article applies only to these relatively advanced cases that require a reconstruction of the lower lip almost close to 100%. In our series of cases, we observed a wide range of reconstructive needs, and best results occurred when the resection did not cross over the limits of lower lip (such as in cases 1 and 3).
In even more severe cases, in which the resection extends further beyond the oral commissure or in cases of associated jaw reconstruction, the use of distant or microsurgical free flaps may be paramount. In these cases, however, excessive volume and unmatched color and texture from distant or free flaps tend to present poor aesthetical results. In addition, in most cases do not have a reconstructed lip with proper motor and tactile sensibility functions2.
The fifth case presented in this study is an example of this kind of situation: the patient had previously undergone an oncological resection of the lower lip and jaw, reconstruction with a pectoralis major myocutaneous flap, and mandibular reconstruction plate. As common observed in these cases, the patient had excessive volume and thickness on the reconstructed lip, undefined aesthetic reference points and lines on the face, absence of tactile sensibility and motor skills on the flaps, and, as a consequence, oral incontinence. This results obtained with this patient showed gain in anatomical definition of the lower third of the face, improvement in the previously existing disproportion between the lower and upper lips, reconstruction of the vermillion with tactile sensibility (according to the patient self-report) and improvement in the oral continence.
The improvement in oral continence perceived of this patient deserves attention in future studies. The reconstruction of vermillion from the skin on the nasolabial flaps maintains the anatomical continuity with the face, and it may preserve some degree of tactile sensibility, which is indispensable for adequate oral continence. Besides, the base of the nasolabial flaps connects with the modiolus in which zygomaticus major muscles have cutaneous insertion and promote superolateral traction at this point9-11. Probably the vermilion reconstruction with nasolabial flaps may promote a belt over the lower lip with ability to elevate it, therefore, favoring oral continence.
CONCLUSIONS
The dissection needed to advance the cheek flaps of the Bernard-Webster technique does not make nasolabial flaps infeasible, which can be properly rotated to add skin and volume to the reconstructed vermilion. It is important to highlight that correct surgical principles of the original technique are kept to preserve its positive aspects.
The modification proposed in our study allowed to add quality to the results, and it provided more volume and projection to the reconstructed vermilion. In more complex cases in which the reconstruction with distant or microsurgical free flaps are necessary, the described technique can also be used secondary in order to improve aesthetical and functional results.
COLABORATIONS
VVO Study design; participation in all operations; analyzing the results; photographic documentation; writing of the manuscript; review and approval of the final text.
ACPO Study design; participation in some surgeries; analyzing the results; photographic documentation; writing of the manuscript; review and approval of the final text.
DS Study design; participation in some surgeries; analyzing the results; photographic documentation; writing of the manuscript; review and approval of the final text.
DS Study design; participation in some surgeries; analyzing the results; photographic documentation; writing of the manuscript; review and approval of the final text.
JBS Study design; participation in some surgeries; analyzing the results; photographic documentation; writing of the manuscript; review and approval of the final text.
MVMC Study design; participation in some surgeries; analyzing the results; photographic documentation; writing of the manuscript; review and approval of the final text.
NTH Study design; participation in some surgeries; analyzing the results; photographic documentation; writing of the manuscript; review and approval of the final text.
REFERENCES
1. Wechselberger G, Gurunluoglu R, Bauer T, Piza-Katzer H, Schoeller T. Functional lower lip reconstruction with bilateral cheek advancement flaps: revisitation of Webster method with a minor modification in the technique. Aesthetic Plast Surg. 2002;26(6):423-8. PMID: 12621564 DOI: http://dx.doi.org/10.1007/s00266-002-2051-5
2. Konstantinović VS. Refinement of the Fries and Webster modifications of the Bernard repair of the lower lip. Br J Plast Surg. 1996;49(7):462-5. PMID: 8983548
3. Webster RC, Coffey RJ, Kelleher RE. Total and partial reconstruction of the lower lip with innervated musclebearing flaps. Plast Reconstr Surg Transplant Bull. 1960;25:360-71. PMID: 13843351
4. Zilinsky I, Winkler E, Weiss G, Haik J, Tamir J, Orenstein A. Total lower lip reconstruction with innervated muscle-bearing flaps: a modification of the Webster flap. Dermatol Surg. 2001;27(7):687-91.
5. López AC, Ruiz PC, Campo FJ, Gonzalez FD. Reconstruction of lower lip defects after tumor excision: an aesthetic and functional evaluation. Otolaryngol Head Neck Surg. 2000;123(3):317-23. PMID: 10964314
6. Rudkin GH, Carlsen BT, Miller TA. Nasolabial flap reconstruction of large defects of the lower lip. Plast Reconstr Surg. 2003;111(2):810-7. PMID: 12560704
7. Orsi VV, Pinto Oliveira AC. Lower lip reconstruction: Rudkin technique and Bernard-Webster technique. Plast Reconstr Surg. 2004;113(4):1296. PMID: 15083053
8. Favalli P, Bergonsi TO, Pavanello DP, Orsi V, Pase P, Schmidt M, et al. Carcinoma epidermóide de pele: aspectos clínico-patológicos e sociais. Rev AMRIGS. 2007;51(4):301-5.
9. Al-Hoqail RA, Abdel Meguid EM. An anatomical and analytical study of the modiolus: enlightening its relevance to plastic surgery. Aesthetic Plast Surg. 2009;33(2):147-52. PMID: 18551340
10. Shim KS, Hu KS, Kwak HH, Youn KH, Koh KS, Fontaine C, et al. An anatomical study of the insertion of the zygomaticus major muscle in humans focused on the muscle arrangement at the corner of the mouth. Plast Reconstr Surg. 2008;121(2):466-73.
11. Pélissier P, Pistre V, Bustamante K, Martin D, Baudet J. The modiolus. Comparative anatomy, embryological and physiological review, surgical importance. Ann Chir Plast Esthet. 2000;45(1):41-7. PMID: 10783511
1. Sociedade Brasileira de Cirurgia Plástica, Rio Grande do Sul, Porto Alegre, RS, Brazil
2. Universidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
3. Hospital Cristo Redentor, Porto Alegre, RS, Brazil
4. Hospital de Clínicas de Porto Alegre, Porto Alegre, RS, Brazil
5. Santa Casa de Porto Alegre, Porto Alegre, RS, Brazil
6. Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, RS, Brazil
7. Universidade Federal de São Paulo, São Paulo, SP, Brazil
8. Hospital São Lucas, Porto Alegre, RS, Brazil
9. Universidade Federal de Ciências da Saúde de Porto Alegre, Porto Alegre, RS, Brazil
10. Hospital Santa Rita, Porto Alegre, RS, Brazil
Institution: Hospital de Clínicas de Porto Alegre, Porto Alegre, RS, Brazil.
Corresponding author:
Victor Vieira Orsi
Rua Itaboraí, 840/703 - Jardim Botânico
Porto Alegre, RS, Brazil Zip Code 90670-030
E-mail: victorvorsi@gmail.com
Article received: May 13, 2013.
Article accepted: May 12, 2016.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket