



Original Article - Year 2016 - Volume 31 -
Analysis of the anatomical lines of the medial nasal dorsum after use of spreader grafts in open rhinoplasty
Análise das linhas anatômicas do dorso médio nasal após utilização de spreader grafts em rinoplastia aberta
ABSTRACT
INTRODUCTION: First described by Sheen in 1984, the use of spreader grafts has become increasingly routine. Spreader grafts are indicated for recovery or maintenance of the internal nasal valve and correction of septum deviation with improvement in the anatomical lines of the nasal dorsum. This study avaluated the anatomical lines of the middle nasal third (MNT) of the nasal dorsum after the use of spreader grafts in open rhinoplasty.
METHODS: A series of 17 patients who underwent rhinoplasty with the inclusion of spreader grafts between March 2013 and November 2014 were analyzed. Spreader grafts were removed from the septum or costal cartilage based on an anthropometric comparison between the medial intercanthal distance and the caudal width of the MNT.
RESULTS: Spreader grafts were effective for septum correction without causing excessive enlargement in 12 patients (70.6%). Three patients (17.6%) had undesirable results with local bulging and 2 patients (11.8%) retained their pre-surgery non-standard measures. In the majority of cases (41.2%), there was a local increase of 3 mm, with a mean of increase of 2.67 mm.
CONCLUSION: In the author's point of view, even in cases where there was bulging of the anatomical lines of the nasal dorsum, spreader grafts promoted long-lasting satisfactory results, and prevented open-roof deformities and stigmas inherent to the surgery itself.
Keywords: Rhinoplasty; Nasal septum; Costal cartilage; Nose/abnormalities.
RESUMO
INTRODUÇÃO: Descritos por Sheen em 1984, os spreader grafts vêm sendo utilizados em rinoplastias de maneira cada vez mais rotineira. São indicados para recuperação ou manutenção da válvula nasal interna e correção do desvio de septo com aprimoramento das linhas anatômicas do dorso nasal. O estudo analisa o comportamento das linhas do terço médio do dorso nasal após o uso de spreader grafts em rinoplastias abertas.
MÉTODOS: Foi avaliada uma série de 17 pacientes, operados entre março de 2013 e novembro de 2014, submetidos à exorrinoplastia com inclusão de spreader grafts, retirados do septo ou cartilagem costal, baseando-se em uma comparação antropométrica entre distância intercantal medial e largura caudal do terço médio nasal.
RESULTADOS: Os enxertos expansores se mostraram eficazes na retificação do septo, sem causar alargamento excessivo em 12 pacientes (70,6%), sendo que três pacientes (17,6%) obtiveram resultados indesejáveis com abaulamento do local e dois pacientes (11,8%) mantiveram suas medidas fora do padrão. Na maior parte dos casos (41,2%) houve aumento de 3 milímetros locais, sendo a média padrão de 2,67 mm por procedimento.
CONCLUSÃO: Constatou-se, no ponto de vista do autor, que os spreader grafts, mesmo nos casos em que houve abaulamento das linhas anatômicas do dorso nasal, promoveram resultados satisfatórios e duradouros, prevenindo deformidades do teto aberto e estigmas inerentes à própria cirurgia.
Palavras-chave: Rinoplastia; Septo nasal; Cartilagem costal; Nariz/ anormalidades.
First described by Sheen in 1984¹, spreader grafts, also called expander grafts, are increasingly indicated and used in rhinoplasty. They are used in open access as in endorhinoplasty, in order to preserve or restore the function of the internal nasal valve and correct deviation of the nasal septum, and also to improve the lines of the middle nasal third (MNT).
Initially, its use was indicated only as an adjuvant procedure in the correction of nasal deformities, such as open-roof or inverted-V, which occur in secondary rhinoplasties. Today, this new technique is also used in primary rhinoplasties, and routinely included in the correction, maintenance, and prevention of both functional and aesthetic alterations of the nasal structure2.
Taking into consideration that nasal hump is one of the most frequent complaints of rhinoplasty patients, the surgeon must pay attention to the characteristics of each patient, including their anatomical properties, sex, and ethnicity. If the technique is poorly indicated or inadequately performed, it can result in both aesthetic and functional complications, such as dorsal enlargement or malfunction of the internal nasal valve3.
Consequently, we still frequently observe some reluctance regarding the use of this technique. However, once the proportionalities and individualities of each patient and the procedure to be adopted are justified, the fear of the alterations that these cartilage grafts could cause, such as excessive irregularities and enlargements of the dorsal lines of the MNT with loss of proportion of the nasal scaffold, should be allayed.
This fear has led surgeons to opt for alternative and less aggressive techniques, such as spreader flaps4, even when expander grafts are contraindicated on the grounds that they may result in supra-tip deformities, third-degree depressions, or mid third depressions, such as inverted-V, after regression of all local residual edema.
The surgeon must always be prepared to use the most modern and refined techniques, such as the use of nasal spreader grafts, to be prepared for future challenges in the areas of aesthetic or reconstructive rhinoplasty.
OBJECTIVE
The objective of this study was to analyze the anatomical lines of the MNT of the nasal dorsum after the use of spreader grafts in open rhinoplasty, based on an anthropometric comparison between the medial intercanthal distance (MID) and the caudal width of the MNT.
METHODS
A series of 17 private clinic and Sistema Unico de Saude (SUS) patients who had been operated on from March 2013 to November 2014 at the Santa Casa de São José do Rio Preto Hospital, SP, Brazil were analyzed. The age of patients ranged from 18 to 45 years. Patients presented with a variety of aesthetic complaints, including dorsal hump, and had agreed to undergo rhinoplasty to rectify the deviations, improve the contour of the MNT, and prevent deformity of the inverted-V and open-roof. The analysis followed the principles of Helsinki with all patients providing informed consent with a Free and Informed Consent Form.
In all cases, spreader grafts were placed after release of the upper lateral cartilage of the septum and correction of the deformities specific to each patient. Most of the autogenous spreader grafts were made of the septal quadrangular cartilage itself, except for two cases (11.8%), which were made from the sternocostal synchondrosis of the fifth arch due to the anatomic incompatibility of the septum as a graft source5.
The length of these grafts was scaled according to the distance between the rhinion and the caudal end of the septum of each patient5,6. The target thickness and width of grafts were approximately 1.5 and 3 mm, respectively. The graft was placed unilaterally in one patient (5.9%) due to the specific degree of laterorhinia of that patient. The contralateral side to the deviation was chosen (Figure 1).
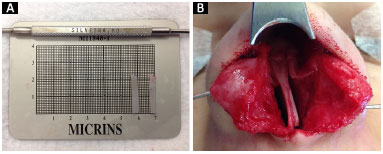
Figure 1. A and B: Preparation of the spreader grafts and their unilateral positioning.
In all cases, the spreader grafts were fixed with three to five transfixing mattress sutures7 with mononylon 5.0. According to the length of the grafts, they were always positioned 1 mm below the upper border of the septal cartilage to provide a more natural triangular shape to the nasal dorsum, rather than a flattened appearance (Figure 2).
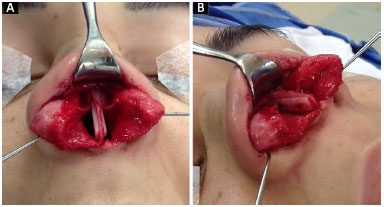
Figures 2. A and B: Fixing of spreader grafts and their bilateral positioning.
Upon completion of their fixation, the superior lateral cartilages were fitted in size with trimming at their upper part and re-attached to the roof, together with the spreader grafts, thus regaining the competence of the internal nasal valve.
These patients were monitored from 6 months to 1 year, and results were catalogued and archived in photo sessions held every 90 days for correlation and future comparison of surgical results8,9. There were no complications inherent to the procedure, such as hematomas, synechiae, necrosis of the septal mucosa, or exposure of cartilage/grafts.
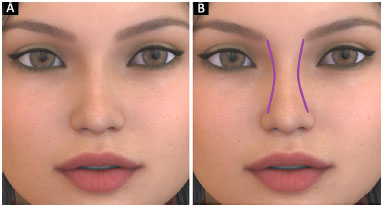
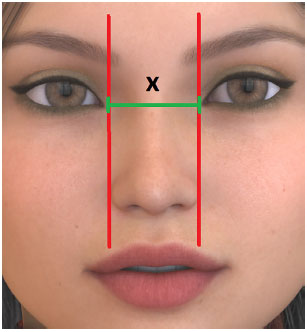
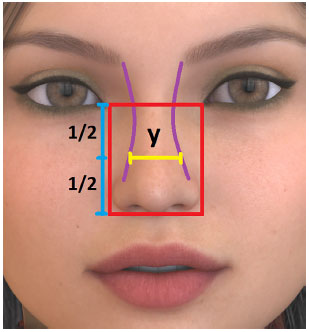
To evaluate the results, from the anatomical lines of the nasal dorsum (Figure 3), a comparison between the MID (Figure 4) and the width of the MNT was used as a reference. The latter was calculated taking into account a horizontal line between the medial corners and another horizontal line drawn at the base of the nose next to the columella. This distance was then divided into two equal parts where the caudal width of the MNT was at the center (Figure 5).
Source: Available online: https://pixabay.com/
Figure 3. A and B: Anatomic lines of the nasal dorsum.
Source: Available online: https://pixabay.com/
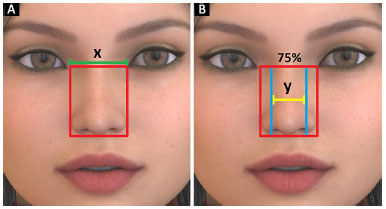
Figure 4. MID (X).
Source: Available online: https://pixabay.com/
Figure 5. MNT (Y).
Considering that the thickness of the alar base (the distance between the two lateral ends of the nasal wings) should be approximately the same as the MID (Figure 6A), the current literature suggests that the caudal width of the MNT should not exceed 75%-80% of the MID10 (Figure 6B).
Source: Available online: https://pixabay.com/
Figures 6. A and B: Normal Y between 75% and 80% of X.
RESULTS
The patients selected for this study were then analyzed and their measures compared in the pre- and post-operative period, specifically in terms of how they compared to normal MNT (between 75 and 80% of the MID) values. Based on the photographic results of the cases exemplified below, the actual increase in millimeters of the width of the MNT with the use of this technique, and the implications of this increase in the aesthetic results achieved are also evident.
Case 1
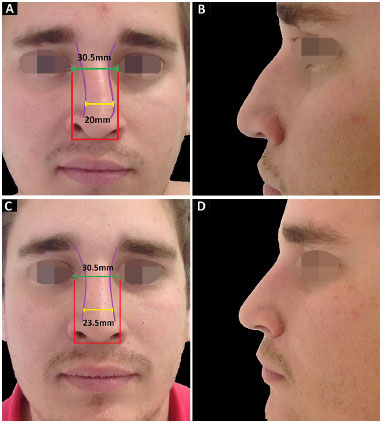
An 18-year-old patient complained of a prominent dorsum and an enlarged tip, with MNT measurements below standard in the pre-operative period (Figure 7A and 7B). A satisfactory aesthetic result was observed in the 6 months post-operative period, with an increase of 3 mm in the width of the MNT after placement of spreader grafts derived from the septum itself, and an MNT measurement within the expected aesthetic standard of between 75% and 80% of the MID (Figure 7C and 7D).
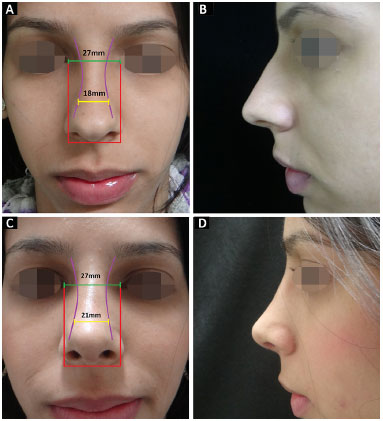
Figures 7. A and B: MNT measure in pre-operative period; C and D: MNT measure in the post-operative period.
Case 2
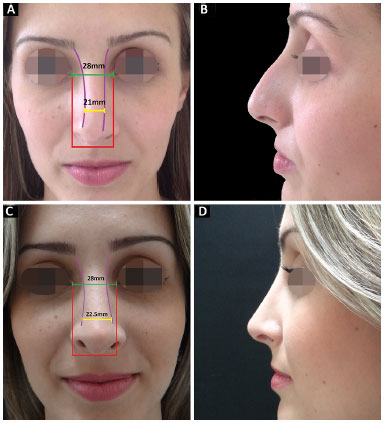
A 32-year-old patient complained of a prominent dorsum and an enlarged and falling tip (Figure 8A and 8B). After insertion of a spreader graft derived from the septum, measurements were within the normal limits with an actual increase of 2 mm in the width of the MNT in the 12-month post-operative period (Figure 8C and 8D).

Figures 8. A and B: MNT measure in pre-operative period; C and D: MNT measure in the post-operative period.
Case 3
A 25-year-old patient complained of a prominent dorsum and drooping tip. Middle nasal third measurements were within the normal range and laterorhinia was present with a rightward deviation (Figure 9A and 9B). We chose to make a septal spreader graft which was positioned unilaterally, contralateral to the deviation. A good aesthetic evolution was observed in the 12-month post-operative period with an actual increase of 1.5 mm of the MNT (Figure 9C and 9D).
Figures 9. A and B: MNT measure in pre-operative period; C and D: MNT measure in the post-operative period.
Case 4
A 22-year-old patient reported previous surgery to correct a deviated septum and laterorhinia. The patient had a prominent dorsum associated with open-roof irregularities and right-sided clamping. Non-standard MNT measurements were present pre-operatively (Figure 10A and 10B), which were corrected and demonstrated in the 6-month post-operative period. Spreader grafts were prepared from sternocostal synchondrosis cartilage of the fifth arch in the secondary open rhinoplasty and an MNT increase of 3.5 mm was achieved (Figure 10C and 10D).
Figures 10. A and B: MNT measure in pre-operative period; C and D: MNT measure in the post-operative period.
The results of MNT anatomical lines after the use of the spreader grafts are presented in Table 1. We compared the results of measurements of the base of the MNT before surgery with the reference values, and in 35.3% of cases, the values were within the expected standard, while 11.8% were above normal and 52.9% were below normal.
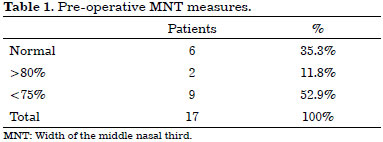
Table 2 shows the results of the measurements after the inclusion of the spreader grafts. Of the 6 patients considered normal before the procedure, the MNT increased to outside of the normal standards in 3 patients (17.6%) and the other 3 patients maintained normal MNT measures. Of the 2 patients with larger than normal MNT pre-surgery, both (11.8%) maintained their larger than normal MNT measurements postoperatively. These were the only 5 unsatisfactory results from an aesthetic point of view (Figure 11).
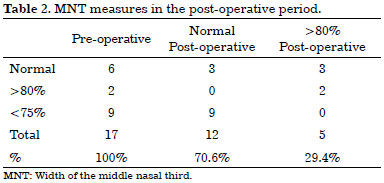
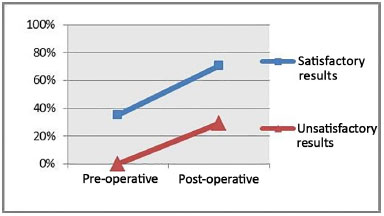
Figure 11. Analysis of pre- and post-operative results.
On the other hand, MNT improvements or maintenance of normal MNT standards was achieved in the majority of patients (12 patients (70.6%).
There was an actual increase in the MNT with the use of spreader grafts in all procedures, varying between 1.5 mm and 3.5 mm (Figure 12). For most patients (7 patients (41.2%)), this increase was 3 mm or less and congruent with the 1.5 mm thickness of each graft.
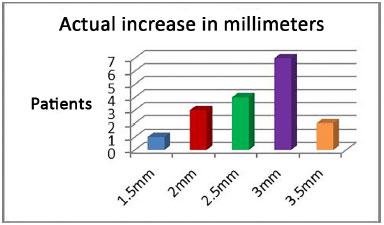
Figure 12. Analysis of the width of the MNT in millimeters.
On the other hand, increases larger than 3 mm occurred in cases where the spreader grafts were made from costal cartilage, and graft thicknesses were close to 2 mm. Interestingly, the case with the smallest increase (only 1.5 mm) was the one in which the expander cartilage graft was used unilaterally.
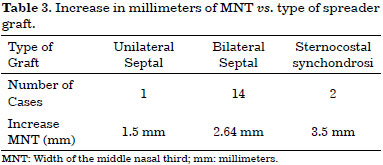
It is interesting that when comparing the increase in millimeters of MNT with the type of graft used, the results are different with an average of 2.64 mm for the bilateral septum grafts and 3.5 mm for costal cartilage grafts (Table 3).
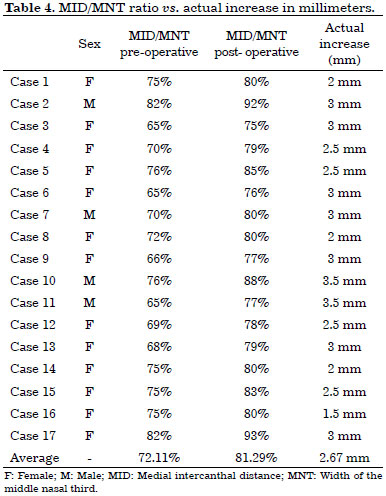
Finally, the average enlargement of the MNT in the total cohort was 2.67 mm with the use of spreader grafts (Table 4). The average degree of variation between the MID and MNT was 72.11% pre-surgery and 81.29% post-surgery. This positive result correlated with the actual increase in millimeters of the MNT per patient.
The database was stored in an Excel table and evaluated statistically with the use of the IBM-SPSS Statistics Viewer 20.0 program.
DISCUSSION
The MNT is an anatomical area where the architecture depends on soft-tissue components for its structure. Problems with this structure can change both respiratory function and dorsal aesthetic lines and as such, the MNT has become increasingly relevant in the study of modern rhinology.
Once the MNT is accessed, consequent disarticulation of its strictly cartilaginous framework may result in the occurrence of local deformities, such as pinching, irregularities, and asymmetries11,12. However, with the advent of spreader grafts in the early 1980s, aesthetic rhinoplasty has become more predictable and safer and may even prevent future adversities related to a breach of this area. Since then, its indication and use have expanded widely in both open and closed access rhinoplasties.
Some authors have reported the drawbacks of this technique including the time taken to perform the procedure, the challenges associated with choice of donor area or type of graft, and last, but not least, the excessive and undesired enlargement caused by the inclusion of these structures along the MNT13,14.
These adverse factors have led several surgeons to avoid this technique for fear of poor aesthetic results and patient dissatisfaction. Many patients seek to obtain a thinner and more delicate nose, and sometimes prefer to run the risk of some irregularities inherent to openroof, such as inverted-V, or even valve deficiency in order to achieve an aesthetically pleasing nose.
However, it is noteworthy that in the three decades that have passed since the advent of spreader grafts, much has been achieved in improving already established techniques, and together with advances in medical technology, more efficient functional and visually smooth results can be achieved.
In 2000, Stal & Hollier15 attempted to mitigate the risks of excessive enlargement of the MNT after the inclusion of spreader grafts and search for an alternative source for making the grafts. They analyzed 10 cases in which polyglycolic acid, a resorbable halogen material, was used and good aesthetic and functional results were obtained twelve months after resorption and fibrosis at the site.
In the analysis performed by Dini et al.16 in 2011, 50 patients had bone grafts taken from the perpendicular plate of the ethmoid, vomer, and nasal floor in an attempt to correct deviations of the septum. The authors achieved satisfactory and long-lasting results, in the correction of both the dorsal and caudal parts of the septum.
Additionally, in a study performed by Almeida17 in 2013, 26 patients underwent treatment of nasal valves, and only one case (3.8%) had excessive bulging of the MNT after using a costal graft of inadequate thickness, which caused not only the bulging of the region but obstruction of the nasal valve. This author warned that "costal cartilage grafts should be carefully sculpted so as not to cause bulging of the MNT and nasal tip, solving the functional problem, but creating a non-aesthetic nose".
Regarding the prevention of functional and aesthetic alterations during a rhinoplasty, Rohrich et al.3 highlighted the importance of nasal remodeling associated with minor resections and de-structuring of the nasal tip cartilage. Gradual reduction of the dorsum is also important for adequate preservation of the upper lateral cartilages by means of minimal modification of the architecture of the nasal scaffold to achieve less aggressive and more harmonious results.
Therefore, the anatomical line results obtained with the use of spreader grafts are more greatly affected by the personal subjective views of the surgeon than the very technique itself, as is the case with many other surgical techniques with advantages and disadvantages in the context of cosmetic and reparative surgery.
Since the subjectivity of aesthetic values and aptitudes compose an immeasurable range of expected results, they cannot always please two experts at the same time. One surgeon may seek to increase the midthird width with the use of spreader grafts, and another may not.
Thus, the importance subjective opinions and variables is extremely important, to the detriment of the insurmountable mathematical objectivity, with regards to plastic surgery of the nose in order to reach the expectations and the desired satisfaction of the patient. As the Scottish philosopher and historian David Hume said, "the beauty of things exists in the spirit of those who contemplate them".
CONCLUSION
Based on the correlation of the anthropometric measures analyzed in this case study, the authors conclude that spreader grafts (even in cases where there was bulging of the anatomical lines of the nasal dorsum), promoted satisfactory and long-lasting results, prevented open-roof deformities, and future stigmas inherent to the surgery itself.
COLLABORATIONS
FGLS Analysis and/or interpretation of data; statistical analysis; final approval of the manuscript; conception and design of the study; completion of operations and/or experiments; drafting the manuscript or critical review of its contents.
REFERENCES
1. Sheen JH. Spreader graft: a method of reconstructing the roof of the middle nasal vault following rhinoplasty. Plast Reconstr Surg. 1984;73(2):230-9.
2. Sheen JH. Rhinoplasty: personal evolution and milestones. Plast Reconstr Surg. 2000;105(5):1820-52.
3. Rohrich RJ, Muzaffar AR, Janis JE. Component dorsal hump reduction: the importance of maintaining dorsal aesthetic lines in rhinoplasty. Plast Reconstr Surg. 2004;114(5):1298-308.
4. Gruber RP, Park E, Newman J, Berkowitz L, Oneal R. The spreader flap in primary rhinoplasty. Plast Reconstr Surg. 2007;119(6):1903-10.
5. Toriumi DM. Discussion: Use of autologous costal cartilage in Asian rhinoplasty. Plast Reconstr Surg. 2012;130(6):1349-50.
6. Gunter JP, Rohrich RJ, Adams WP Jr. Dallas rhinoplasty: nasal surgery by the masters. 2nd ed. St. Louis: Quality Medical Publishing; 2007.
7. Gruber RP, Nahai F, Bogdan MA, Friedman GD. Changing the convexity and concavity of nasal cartilages and cartilage grafts with horizontal mattress sutures: part II. Clinical results. Plast Reconstr Surg. 2005;115(2):595-606.
8. Guyuron B. Precision rhinoplasty. Part I: The role of life-size photographs and soft-tissue cephalometric analysis. Plas Recontr Surg 1988;81(4):489-99.
9. Martins ALM, Pretto Neto AS, Milani AR, Silveira DPM, Steffen N, Ely PB. Sistematização da fotografia para planejamento cirúrgico em rinoplastia. Rev Bras Cir Plást. 2013;28(3):30.
10. Ercan I, Ozdemir ST, Etoz A, Sigirli D, Tubbs RS, Loukas M, et al. Facial asymmetry in young healthy subjects evaluated by statistical shape analysis. J Anat. 2008;213(6):663-9.
11. Byrd HS, Hobar PC. Rhinoplasty: a practical guide for surgical planning. Plast Reconstr Surg. 1993;91(4):642-54.
12. Almeida GS, Pessoa BBGP, Oliveira NGS, Gomes AAR, Crisóstomo MR, Pessoa SGP. Reconstrução do terço médio nasal em rinoplastia primária. Rev Bras Cir Plást. 2008;23(2):124-7.
13. Pochat VD, Alonso N, Meneses JVL. Avaliação funcional e estética da rinoplastia com enxertos cartilaginosos. Rev Bras Cir Plást. 2010;25(2):260-70.
14. Pochat VD, Alonso N. Avaliação da permeabilidade das vias aéreas com a utilização dos enxertos expansores (spreader grafts) em rinoplastia: estudo preliminar. Rev Bras Cir Plást. 2010;25(1):59-63.
15. Stal S, Hollier L. The use of resortable spacers for nasal spreader grafts. Plast Reconstr Surg. 2000;106(4):922-8.
16. Dini GM, Iurk LK, Ferreira MC, Ferreira LM. Grafts for straightening deviated noses. Plast Reconstr Surg. 2011;128(5):529e-537e.
17. Almeida GS. Tratamento das válvulas nasais em rinoplastia secundária. Rev Bras Cir Plást. 2013;28(3):422-7.
1. Santa Casa de Misericórdia de São Jose do Rio Preto, SP, Brazil
2. Sociedade Brasileira de Cirurgia Plástica, São Paulo, SP, Brazil
Institution: Santa Casa de Misericórdia de São Jose do Rio Preto/Clínica Privada, São José do Rio Preto, SP, Brazil.
Corresponding author:
Frederico Guilherme Lopes Silveira
Rua Silva Jardim, 1890 - Centro
São Jose do Rio Preto, SP, Brazil Zip Code 15025-065
E-mail: contato@drfredericosilveira.com.br
Article received: July 15, 2015.
Article accepted: September 29, 2015.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket