



Case Report - Year 2017 - Volume 32 -
Management of Stahl's ear: a case report
Manejo da deformidade auricular de Stahl: um relato de caso
ABSTRACT
Stahl's ear deformity was first described in the 19th century and it consists of a rare auricular deformity characterized by hypoplasia of the antihelix crus with enlargement of its base and a third crus of the antihelix connected to posterior portion of helix crus, which deforms the posterolateral wall of the external auditory canal. Reconstructive surgery is the definitive treatment, however, because of the diversity of clinical presentations, no standard technique exist for all cases. The method described in this report is another treatment option and entails the resection of the third crus and reconstruction of superior crus of the antihelix.
Keywords: Ear deformities acquired; Ear; Reconstructive surgical procedures.
RESUMO
Descrita no século XIX, a deformidade auricular de Stahl consiste em uma má formação auricular rara, caracterizada por hipoplasia da raiz da anti-hélice com o alargamento de sua base e uma terceira raiz da anti-hélice conectando-a à parte posterior da hélice, deformando a porção posterossuperior do pavilhão auditivo. A correção cirúrgica é o tratamento definitivo, porém, pela diversidade de apresentações clínicas, não há uma técnica padrão para todos os casos. O método descrito neste relato é mais uma opção de tratamento e consiste na ressecção da terceira cruz e confecção da raiz superior da anti-hélice.
Palavras-chave: Deformidades adquiridas da orelha; Orelha; Procedimentos cirúrgicos reconstrutivos.
In the 19th century, Stahl described and classified different auricular malformations into three types: "helix transversus spleniformis", "crus antihelics trifurcata" and "crus superium turgidum". Currently, the term Stahl's ear refers to the second type, a hypoplasia of the antihelix crus, with enlarged base and a third crus of the antihelix extending from the antihelix to the helix crus, deforming the posterolateral wall of the external auditory canal.
This anomaly has aesthetic and social consequences, but it does not affect hearing. It is more common among eastern people and rarely seen in white people, however, its real incidence has not been established1 so far. The deformity is most commonly unilateral, and it can be bilateral in 20% of cases. In general, other anomalies are also present, such as narrowing of the helix, hypoplasia or absence of the superior crus of antihelix and enlargement of the triangular fossa2.
Stahl's ear would be the consequence of dysgenesis of the intrinsic atrial muscle during the third month of embryogenesis3. Embryonic muscular dysgenesis leads to hypoplasia of the superior crus of antihelix, and development of a third crus of the antihelix. The third crus that connects the antihelix to the posterolateral wall of the helix is responsible for causing the defect on the curvature of the auditory canal4. The solution for the deformity is reconstructive surgery, but there is no consensus regarding the technique to be used.
CASE REPORT
We report a case of an 18-year-old white man with Stahl's ears deformity (Figure 1) who underwent reconstructive surgery under general anesthesia. An infiltration of the incisions was performed using 0.75% ropivacaine with epinephrine in a 1: 100,000 proportion. A retroauricular access was performed in the concha-Antihelix transition with detachment to anterior portion, enabling degloving of the ear and exposure of the third crus (Figure 2).

Figure 1. Antihelix third root found in Stahl's ear. A: Right ear, B: Left ear.
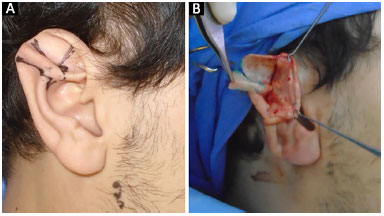
Figure 2. Transoperatory exposition of third crus. A: Preoperative marking of third crus; B: Third crus resected in transoperative.
A resection of the third crus was performed with primary approximation of the defect. To reconstruct the superior crus of the antihelix, prior cartilage weakening was done with metal scraping and Mustarde 4-0 polyglactin suture. To reconstruct a uniform curvature of the helix, a subsequent cartilage weakening was carried out with a scalpel blade no.15 and x-suture for eversion with 4-0 polyglactin.
Closing of the posterior incision was performed using a Greek bar suture with 4-0 polyglactin. Ear dressings were made with sterile bandages and maintained for 48 hours. The same procedure was performed in both ears. The result after the surgery is shown in the late postoperative period (Figure 3) in which little changes in size of the ear is observed associated with absence of third crus, and presence of helix and superior crus.
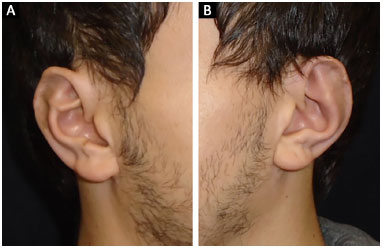
Figure 3. Late postoperative period. A: Right ear; B: Left ear.
DISCUSSION
Congenital auricular deformities are defined as malformations (microtia, cryptotia). Deformities are characterized as a normal chondrocutaneous component, but with an abnormal architecture categorized as constricted, prominent, and Stahl deformity, as described in this study5.
A number of techniques for surgical reconstruction of Stahl's ear have been described. These techniques range from simple procedures as zetaplasty, which is a realignment of the third crus, the wedge resection of cartilage, the local grafting after its reversion6,7 to more complex procedures such as temporal periosteal flap for auricular support described by Nakayama et al8.
There are reports of non-operative treatment using splints, which are used to shape the auricle, however more satisfactory results are seen if this treatment is performed in the neonatal period9. However, there are different degrees of clinical presentation of the syndrome, therefore it is difficult to achieve consistent results using a standard surgical technique.
Currently, the modified Chongchet technique are the most commonly used for the treatment of this anomaly10. There is a trend to use Mustarde sutures in mild deformities associated with cartilage weakening maneuvers. Severe cases require the use of previous technique associated with excision of cartilage and skin.
CONCLUSION
Stahl's ear is a rare auricular malformation that can bring social stigma to the patient. The method described constitutes another alternative for treating this disease, especially in cases where the deformity is more significant, and may produce satisfactory aesthetic results.
COLLABORATIONS
JM Statistical analysis: final approval of the manuscript to be published, conception and design of the study, operations and/or experiments, drafting the manuscript or critical review of the content.
ACPO Final approval of the manuscript to be published, conception and design of the study, operations and experiments.
LMP Analysis and/or interpretation of data, conception and design of the study, drafting the manuscript or critical review of the content.
JB Analysis and/or interpretation of data, drafting the manuscript or critical review of the content.
MVMC Final approval of the manuscript to be published, operations and/or experiments.
REFERENCES
1. Fischl RA. The third crus of the anthelix and another minor anomaly of the external ear. Plast Reconstr Surg. 1976;58(2):192-5. PMID: 940872 DOI: http://dx.doi.org/10.1097/00006534-197608000-00009
2. Ferraro GA, Perrotta A, Rossano F, D'Andrea F. Stahl syndrome in clinical practice. Aesthetic Plast Surg. 2006;30(3):348-9. DOI: http://dx.doi.org/10.1007/s00266-005-0139-4
3. Yotsuyanagi T, Nihei Y, Shinmyo Y, Sawada Y. Stahl's ear caused by an abnormal intrinsic auricular muscle. Plast Reconstr Surg. 1999;103(1):171-4. PMID: 9915179 DOI: http://dx.doi.org/10.1097/00006534-199901000-00027
4. Gleizal A, Bachelet JT. Aetiology, pathogenesis, and specific management of Stahl's ear: role of the transverse muscle insertion. Br J Oral Maxillofac Surg. 2013;51(8):e230-3. DOI: http://dx.doi.org/10.1016/j.bjoms.2013.01.018
5. Porter CJ, Tan ST. Congenital auricular anomalies: topographic anatomy, embryology, classification, and treatment strategies. Plast Reconstr Surg. 2005;115(6):1701-12. PMID: 15861078 DOI: http://dx.doi.org/10.1097/01.PRS.0000161454.08384.0A
6. Nakajima T, Yoshimura Y, Kami T. Surgical and conservative repair of Stahl's ear. Aesthetic Plast Surg. 1984;8(2):101-7. DOI: http://dx.doi.org/10.1007/BF01575252
7. Kaplan HM, Hudson DA. A novel surgical method of repair for Stahl's ear: a case report and review of current treatment modalities. Plast Reconstr Surg. 1999;103(2):566-9. PMID: 9950546 DOI: http://dx.doi.org/10.1097/00006534-199902000-00031
8. Nakayama Y, Soeda S. Surgical treatment of Stahl's ear using the periosteal string. Plast Reconstr Surg. 1986;77(2):222-6. PMID: 3945685 DOI: http://dx.doi.org/10.1097/00006534-198602000-00008
9. Lindford AJ, Hettiaratchy S, Schonauer F. Postpartum splinting of ear deformities. BMJ. 2007;334(7589):366-8. PMID: 17303887 DOI: http://dx.doi.org/10.1136/bmj.39063.501377.BE
10. Chongchet V. A method of antihelix reconstruction. Br J Plast Surg. 1963;16:268-72. PMID: 14042756 DOI: http://dx.doi.org/10.1016/S0007-1226(63)80120-4
1. Hospital de Clínicas de Porto Alegre, RS, Brazil
2. Universidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
3. Faculdade de Medicina da Universidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil
4. Universidade de Barcelona, Barcelona, Spain
Institution: Hospital de Clínicas de Porto Alegre, RS, Brazil.
Corresponding author:
João Maximiliano
Rua Ramiro Barcelos, 2350 - Santa Cecilia
Porto Alegre, RS, Brazil Zip Code 90035-903
E-mail: jmaximilianopm@gmail.com
rticle received: August 24, 2016.
Article accepted: February 21, 2017.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket