



Case Report - Year 2017 - Volume 32 -
Earlobe hypertrophy correction
Correção da hipertrofia do lóbulo auricular
ABSTRACT
INTRODUCTION: The ear is a structure of the face with important aesthetic value. The dimensions of the ear and the appearance of its anatomical components change with age, disease and cultural practices which can result in an aesthetically unpleasant form over time. The earlobe is an important anatomical part of the ear and is considerably influenced by the factors above. It is made of fatty tissue and skin and can undergo changes in its proportion and flaccidity, which may be improved by surgical procedures to make it more aesthetically pleasing, providing a more proportional or younger appearance. This article reports the case of a 30-year-old patient who considered his earlobes disproportionate in relation to the rest of his ears and underwent surgery to have them reduced.
METHODS: A simple and fast recovery surgical procedure was carried out delineating and resecting a part of each of the patient's earlobes.
RESULTS: The results proved to be satisfactory as the patient had more proportional earlobes in relation to the rest of his ears achieving aesthetic improvement.
CONCLUSION: The technique described in this article to reduce hypertrophied earlobes proved to be efficient.
Keywords: Ear/anatomy & histology; Hypertrophy; Ear/surgery; Rhytidoplasty; Cicatrix; Reconstructive surgical procedures.
RESUMO
INTRODUÇÃO: A orelha é uma estrutura da face que tem valor estético. As dimensões da orelha e aparência dos seus componentes anatômicos são modificados com a idade, doenças e práticas culturais que podem resultar em uma estética desagradável com o tempo. O lóbulo é um componente anatômico importante da orelha que é bastante influenciado esteticamente por estes fatores. Ele é composto por tecido adiposo e pele e pode sofrer mudanças na sua proporção e flacidez, as quais podem ser melhoradas, por meio procedimentos cirúrgicos, para ficarem esteticamente mais agradáveis, com o intuito de oferecer uma aparência mais proporcional ou jovem. Este trabalho descreve um caso de um paciente de 30 anos que considerou os lóbulos das suas orelhas desproporcionais ao resto da orelha e fez cirurgia para reduzi-los.
MÉTODOS: Foi realizado um procedimento cirúrgico simples, de recuperação rápida para reduzir o tamanho dos lóbulos do paciente por marcação e resseção de uma parte de cada lóbulo do paciente.
RESULTADOS: Os resultados se mostraram satisfatórios com lóbulos mais proporcionais ao resto das orelhas e melhora da estética do paciente.
CONCLUSÃO: A técnica descrita neste trabalho para a redução de lóbulos auriculares hipertrofiados se mostrou eficaz.
Palavras-chave: Orelha/anatomia & histologia; Hipertrofia; Orelha/cirurgia; Ritidoplastia; Cicatriz; Procedimentos cirúrgicos reconstrutivos.
The ear plays an important role in hearing, but it also has an aesthetic function on the human face. It embryologically originates from six mesenchymal proliferations from the first two pharyngeal arches, with the earlobe being the last part to develop1.
The orientation and appearance of the ear reveal information on the age and gender of an individual and contribute for facial beauty. The ear, even though barely noticed most of the time, gives a certain proportionality and symmetry to the face and thus has aesthetic value. It is because of this aesthetic value that any abnormality or damage to the ear draws attention to the individual and causes psychosocial discomfort2.
The external ear consists of an elastic sheet of cartilage unevenly covered by a thin layer of skin. The ear has a series of depressions and elevations that are important for its hearing function (Figure 1). It consists of the following major anatomical regions: the helix, crus of antihelix, scapha, antihelix, crura of antihelix, triangular fossa, concha of auricle, tragus, antitragus, and earlobe3.
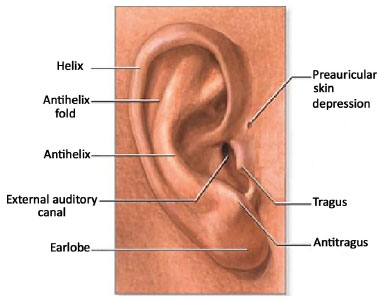
Figure 1. Anatomy of the human ear. Available at:<http://minhavida-symnav.adam.com/content.aspx?productId=125&pid=70&gid=1126>
The helix is the ear's highest anatomical border whereas the scapha is a long depression located below the helix. The elevation below the scapha is called the antihelix which ends cranially in two branches. The cavity between these two branches is called triangular fossa. The largest depression in the ear is located just before the entrance of the ear canal and is called the concha of auricle. The tragus, the antitragus and intertragic notch are located near the ear canal. The earlobe is located on the lower portion of the ear.
The earlobe is a skin and fatty tissue fold without cartilage tissue that has a good blood supply4,5. It has many nerve endings and in some individuals it is an erogenous zone. The ear lobe has no specific function, however it has aesthetic value and any disproportion or deformity is easily perceived.
The earlobe is classified according to its adherence to the face on the jaw border. There are three types of ear lobes: the free type that is not joined to the jaw border, the attached type which is joined to the jaw border and the adherent type which is an accentuated type of attached earlobe2.
The ear lobe has great historical value, especially in the tradition of its piercing for the use of various ornaments and jewelry. Depending on the culture it is mandatory or optional, according to the status or gender of the individual. In some cultures, it is customary to pierce the earlobe and place ornaments within the opening to stretch it, in others both the earlobe and the helix are embellished while in others only the lobe is adorned. Even today in the modern world this practice still exists and is used by both females as males.
The earlobe's proportions and appearance may become an aesthetic problem as a result of phenomena such as earlobe hypertrophy, torn earlobe, keloids, and aging. Hypertrophy occurs in both genders and in all races. It is notable that the earlobe size varies in relation to the individual's race.
Earlobe hypertrophy becomes more pronounced with aging and is related to the individual's race. This aesthetic deterioration may be seen as soon as the age of 40 in the case of Caucasians2. This is due to the natural loss of collagen fibers and elastic fibers that render the earlobe more flaccid. Sagging increases the size of the ear turning hypertrophy more obvious.
This article reports the case of a male patient who sought out plastic surgery to reduce his earlobes due to the psychosocial discomfort caused by their size.
OBJECTIVE
The objective of this article is to discuss a simple technique that is commonly employed to reduce the size of hypertrophied earlobes.
METHODS
A thirty-year-old male patient arrived at a plastic surgery practice with a complaint of hypertrophied earlobes (Figures 2 and 3). The patient reported his discomfort due to the size of his earlobes and the desire to reduce them to a more aesthetically appropriate size.
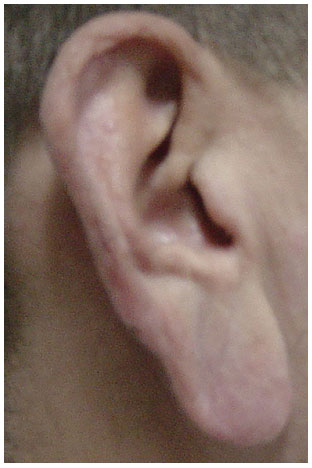
Figure 2. Right ear - preoperative.

Figure 3. Preoperative image of patient's ears.
First the patient underwent a pre-surgical analysis and tests were performed to determine surgical indication. After the surgical indication and evaluation of the tests, patient's consent was formally obtained and the surgery was scheduled at private hospital in Belém.
One of the most crucial procedures in the preoperative period was the earlobe marking. During marking three points were established, points X, Y and Z. This technique establishes three points that delineate an angle which may have different proportions depending on the proportion of the ear to be resected.
Point X is the earlobe insertion point on the face and point Y is determined by the midpoint of the patient's earlobe. Point Z was marked in such a way to maintain the pedicle of the free earlobe with a reasonable size. In this case the angle established by points X, Y and Z was 25 degrees. After marking of the earlobe, the patient was anesthetized with local anesthesia.
The main incision on the earlobe was made at the earlobe's insertion point on the face, a line below the antitragus- line XY. The demarcated area was resected using a scalpel blade 11. The result was the resection of a triangular portion of the patient's earlobe.
After resection, hemostasis was achieved with electrocoagulation and the remainder of the lobe was sutured. Suture was performed with a needle holder and nylon 6.0 using simple stitches. The dressing was made later. In the post-surgical stage the patient was warned of the importance of keeping the ear clean and that the dressing was to be changed daily. Stitches were removed on postoperative day 14. The procedure was carried out in December 2014 in Belem, PA, Brazil in accordance with the principles of the Declaration of Helsinki 2000.
RESULTS
The technique used in this case is very simple, commonly used and does not pose any challenges or complications. In this case, there were no post-surgical complications such as dehiscent points, badly-positioned scar, scar extension or scar infection.
Since the position of the scar on the ear after the procedure is very important, the resection and suture were performed in such a way to ensure that the position of the scar would be the least visible possible. The resection of a part of the earlobe not only adjusted its size and contour, but also had a psychological effect on the patient, as the procedure improved the physiognomic appearance of the patient which in turn increased his self-esteem in relation to his appearance.
The surgery was a success and the wound healed without complications. The result was considered satisfactory by the surgeon and the patient (Figures 4 and 5).

Figure 4. Left ear - postoperative - oblique angle.

Figure 5. Right ear - postoperative - oblique angle.
DISCUSSION
According to a survey carried out by Azaria et al.6 on the morphology of the human ear lobe, the mean length of the earlobe is between 1.97 cm and 2.01 cm. In general, the earlobe's length is 28-30% of the total length of the ear. Factors that contribute to the size of the earlobe are ethnicity, gender and age. Hypertrophy of the earlobe may be genetic or macrotia associated with skin conditions such as leprosy and cancer5,7. With aging, auricular hypertrophy becomes more pronounced as the earlobe naturally sags with age. Earlobe correction procedures are recommended when the lobe exceeds 33% of the total length of the ear8.
Over the years many techniques have been developed by various authors to resect portions of the earlobe1,9. These techniques have been modified and new ones have been developed and used to correct earlobe hypertrophy. These techniques are not exclusive to earlobe hypertrophy correction and may be used in other procedures such as the correction of fallen earlobes associated with the use of heavy earrings and aged earlobes. The reduction of the earlobe can be performed as an isolated procedure or may be associated with the cervical-facial aesthetic treatments such as facelifts.
The aesthetic appearance of the hypertrophied earlobe can be worsened by the use of heavy earrings and aging and cosmetic procedures are required to improve its appearance. This is due to the fact that with age the amount of collagen and skin elasticity decrease, giving the lobe to have an elongated and wrinkled appearance.
The use of heavy earrings can make the problem worse because the skin becomes weak and stretched with their use. The earlobe of a young man is on average 1.8 cm long and 2 cm wide at the midpoint10. Being familiar with these basic measurements and the anatomical features of the earlobe and the ear in general, enables the surgeon to reconstruct the earlobe so that it becomes aesthetically acceptable.
An important aspect during this procedure is the correct placement of the surgical scar4,7,10. If adequate care is not taken during the suturing of the earlobe or in post-surgical dressings this can produce an undesirable scar. It important to take tension and contraction of the scar into account to guarantee satisfactory results7,10.
Patients should not touch the dressing and/or the wound excessively to favor a good scar and decrease the probability of infection. Another important factor is that patients should not attempt to pierce the operated earlobe before at least 6-8 weeks after the surgery and it is recommended that the new piercing be placed off the scar line, because the scar tissue is weaker than intact tissue.
The technique used in this case may resect the patient's earring hole requiring to redo the piercing in an area away from the scar, avoiding dehiscence. It is also recommended that if a patient wishes to gauge his/her earlobe that it should be small, as large ones increase the risk of the reopening of the scar.
This procedure not only reduces the size of the earlobe to normal limits but it also gives the patient a younger appearance. The ear is an important part of the face and may reveal the age of an individual although other aesthetic procedures excluding the ears may have been performed in an effort to conceal patient's age. Therefore, the appearance of the ears must be taken into account in procedures aiming at rejuvenating the patient's face.
CONCLUSION
This article reported a simple technique used to reduce hypertrophied earlobes to normal limits. The procedure was considered successful due to the lack of complications in its performance, satisfactory healing and the resulting aesthetic improvement.
COLLABORATIONS
MMGF Analysis and/or interpretation of data; final approval of the manuscript; conception and design of the study; completion of surgeries and/or experiments; writing the manuscript or critical review of its contents.
DDP Conception and design of the study; completion of surgeries and/or experiments; writing the manuscript or critical review of its contents.
REFERENCES
1. Moore KL, Persaud TVN. Embriologia Clínica. 9ª ed. Rio de Janeiro: Elsevier; 2012.
2. Pitanguy I, Muller P, Kauk LK, Freitas LFP. Incisões remodelantes no lóbulo da orelha. Rev Bras Cir Plást. 1998:78(2):155-62.
3. Netter FH. Atlas de Anatomia Humana. 4ª ed. Rio de Janeiro: Elsevier; 2008.
4. Bisaccia E, Patel P, Scarbough D. Treatments for earlobe ptosis. Dermatologist. 2012;20(4):35-7.
5. Cabral AR, Brinca A, Figueiredo A, Alfonso N, Vieira R. Reconstrução do lóbulo auricular pela técnica de Gavello e retalho bilobado. An Bras Dermatol. 2013;88(2):272-5. DOI: http://dx.doi.org/10.1590/S0365-05962013000200018
6. Azaria R, Adler N, Silfen R, Regev D, Hauben DJ. Morphometry of the adult human earlobe: a study of 547 subjects and clinical application. Plast Reconstr Surg. 2003;111(7):2398-402. DOI: http://dx.doi.org/10.1097/01.PRS.0000060995.99380.DE
7. Silveira IM. Correção cirúrgica das hipertrofias do lóbulo da orelha [acesso 2017 Maio 2]. Disponível em: http://hansen.bvs.ilsl.br/textoc/revistas/brasleprol/1940/pdf/v8n1/v8n1a01.pdf
8. Mowlavi A, Meldrum DG, Wilhelmi BJ, Ghavami A, Zook EG. The aesthetic earlobe: classification of lobule ptosis on the basis of a survey of North American Caucasians. Plast Reconstr Surg. 2003;112(1):266-72. DOI: http://dx.doi.org/10.1097/01.PRS.0000066368.07829.9B
9. Pitanguy I. Aesthetic Plastic Surgery of Head and Body. Berlin: Springer; 1981.
10. Colombo LRC, Guimarães PMS, Motta IA, Cunha MTR, Silva Neto MP. Rejuvenescimento de lóbulo de orelha: descrição da técnica de indicações. Rev Bras Cir Plást. 2013:28(2):289-93.
1. Sociedade Brasileira de Cirurgia Plástica, São Paulo, SP, Brazil
2. Instituto Gomes Faial, Belém, PA, Brazil
3. Universidade Federal do Pará, Belém, PA, Brazil
Institution: Instituto Gomes Faial, Belém, PA, Brazil.
Corresponding author:
Manuel Mário Gomes Faial
Rua Tiradentes, 62 - Reduto
Belém, PA, Brazil Zip Code 66053-330
E-mail: clinicamariofaial@yahoo.com.br
Article received: July 9, 2015.
Article accepted: April 23, 2017.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket