



Articles - Year 2003 - Volume 18 -
Standardization of the Medical Record in Plastic Surgery
Padronização da Ficha Clínica em Cirurgia Plástica
ABSTRACT
The objective of the present study is to propose a standardization of the medical record for Plastic Surqery. The record model proposed would work for most plastic surgeons, and could befilled out in an automated and oriented manner by the physician and also allow adaptations according to individual needs. Data on Identification, Chief Complaints, History of Present Illness, Systems Investiqation, Personal Background and Family Background could also befilled out alternatively by the patient him/herself by using language and expressions accessible to the lay public, and in order to support the physician more effictively in the case of legal disputes. The record can be viewed quickly and objectively due to the use of figures and diagrams. It has a simple cataloguing and filing system for photographic documents and registered data are numbered in orden so that they may be computcrized, making scientific research easier and minimizing data collecting errors. The record model may be used in hospitais, outpatient clinics and individual medical offices. The resolutions of the medical entities that regulate the utilization of Medical Records or Medical Files are also discussed.
Keywords: Medical record; medical files; automated medical recording systems; medical legislation; informed consent
RESUMO
O objetivo deste trabalho é propor uma padronização de ficha clínica para ser utilizada na especialidade de Cirurgia Plástica. O modelo de ficha proposto atenderia a maioria dos cirurgiões plásticos, podendo ser preenchida pelo médico de forma dirigida e automatizada e apresentando a possibilidade de adaptações pessoais conforme a necessidade. Os dados de Identificação, Queixa e Duração, História Pregressa da Moléstia Atual, Interrogatório Sobre os Diversos Aparelhos, Antecedentes Pessoais e Antecedentes Familiares podem também ser preenchidos alternativamente pelo próprio paciente, com a utilização de linguagem e expressões acessíveis ao público leigo, respaldando de forma mais eficaz o médico em eventuais ações legais. Apresenta uma visualização rápida e objetiva pelo uso de figuras e esquemas. Contém um simples sistema de catalogação e arquivamento de documentação fotográfica e os dados registrados são numerados para serem passíveis de informatização, com a finalidade de facilitar pesquisas científicas e minimizar erros na coleta de informações. Esse modelo de ficha pode ser utilizado em hospitais, ambulatórios e consultórios. Também são abordadas as resoluções das entidades médicas que legislam sobre a utilização do Registro Clínico ou Prontuário Médico.
Palavras-chave: Ficha clínica; registros médicos; sistemas automatizados de registros médicos; legislação médica; consentimento esclarecido
Another specificity of the specialty is that a result that may be considered satisfactory by the surgeon may not be so considered by the patient, or vice-versa.
The result of a surgery may also depend on factors that are not significant in other specialties. There are variables that may influence the quality of results, such as previous prolonged exposure to the sun, obesity, exaggerated and repeated changes in weight, post diet malnutrition in order to undergo plastic surgery, utilization of contraceptives, smoking, racial and age factors that interfere in scarring, and major psychological personality conditions, generally related to selfesteem and self-image.
Plastic Surgery, and more specifically aesthetic surgery, among the various medical specialties, is one that most frequently leaves the professional vulnerable to legal dispute. All these specificities of the specialty make it interesting to have a comprehensive and standardized "Medical Record" or "Medical Observation" that meets the needs of most plastic surgeons.
Integrating a medical record with standardized photographic documents benefits the plastic surgeon who could take better advantage of his routine work. The medical Record for the Plastic Surgery patient is unique in the association of the Medical Record and photographic documents, therefore being called Clinical- Photographic Record or Photo-Document Set. "The medical record should comprise clearly the identification of the patient; daily medical follow-up (if inpatient); follow-up of nurses and other professionals; laboratory, radiological and other tests; medical reasoning, diagnostic assumptions and definite diagnosis; treatment, medical prescriptions, descriptions of surgeries, anesthetic records, discharge summary, outpatient appointments and/or urgencies, medical observation chart and physician follow-up."(l) The Federal Medical Council enacted Resolution 1639 on July 10, 2002, approving the "Technical Standards for Using Computerized Systems for Keeping and Handling Medical Records "(2).It established a minimum of 20 (twenty) years, as of the last recording, for keeping medical records in hard copies. Afterwards, the record may be stored in any magnetic or optical electronic medium and microfilmed, as long as it can be recovered, according to the standards of the Brazilian Society of Information Technology in Health (Sociedade Brasileira de Informática em Saúde - SBIS), in a specific association with the Federal Medical Council, and anticipated in the Brazilian Filing Legislation (2).
"The data that comprise the record belong to the patient and should be available on a permanent basis, so that whenever requested by the patient or proxy,they should allow for authentic copies of the pertinent information"(2) The Regional medical Council stresses the rights of the patient: "To have access, at any time, to his/her medical record and receive in writing the diagnosis and treatment recommended, bearing identification with the name of the professional and registration number at the agency responsible for regulating and controlling the profession"(1). Moreover, "The physician can not disclose the content of the medical record or file without the patient's consent, except for legal obligations. If the request is submitted by the family, the patient must give authorization"(1).
The quality of medical care depends on the quality of the information in the record (3). A standard Clinical Chart should order the parts that refer to history, general and special physical exam and subsidiary tests. Registered data should be easy to see in a simple, fast and objective manner. The follow-up of the chart would assist scientific research, because of the possibility of computerization due to the numeric fields for registering data(4,5,6). The record could be adapted for use in offices, outpatient clinics and hospitals. Using the record in a hospital with a busy surgery schedule would minimize the high possibility of errors whenever statistical studies are performed (7,8).
The model for the standardized Medical Record herein proposed allows consistent utilization among plastic surgeons, responding to the needs of most professionals and is flexible enough to allow for individual adaptations. The fields were ordered aiming at following clinical reasoning and the distribution of space is adequate to the content of each item to be filled out. It allows a quick and global view of information due to the utilization of figures and diagrams, and also allows for an easy and oriented way of writing information (Figs. 1-6).
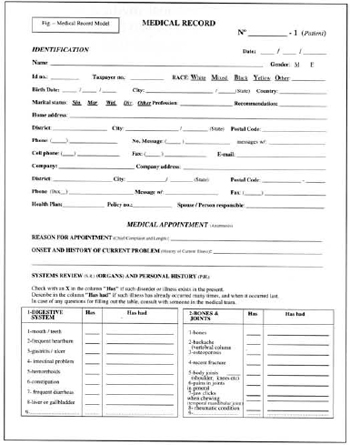
Fig. 1 - Medical record (page 1).
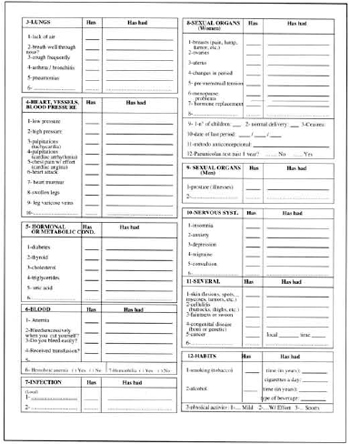
Fig. 2 - Medical record (page 2).
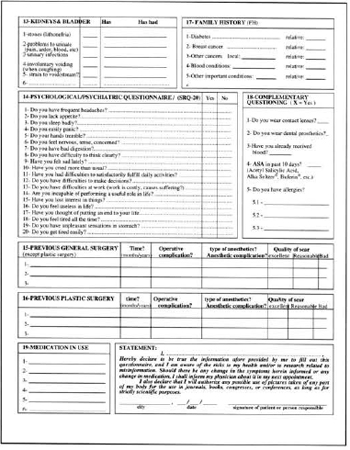
Fig. 3 - Medical record (page 3).
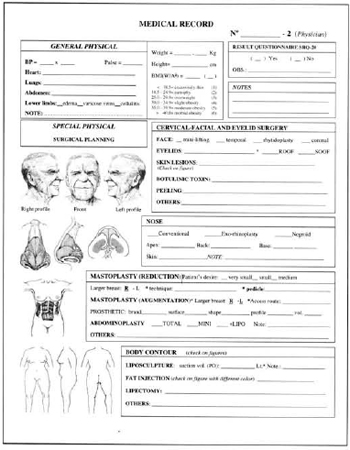
Fig. 4 - Medical record (page 4).
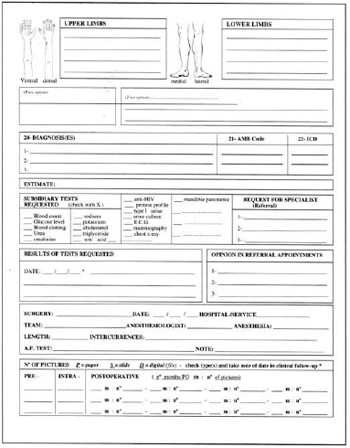
Fig. 5 - Medical record (page 5).
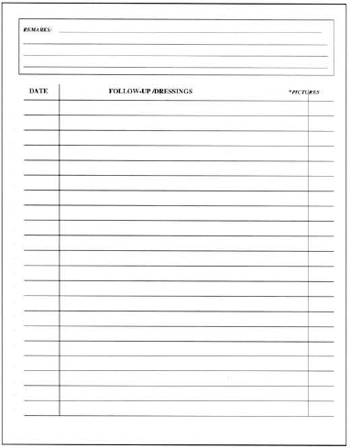
Fig. 6 - Medical record (page 6).
As the item "Chief Complaints" is characteristically short and objective for most Plastic Surgery patients and because it was intended to optimize questions on the record, the items "History of Present Illness" (HPI) and "Family Background" (FB) were emphasized less, and "Systems Investigation" (SI) and" Personal Background" (PB)(9) were emphasized more.
Bearing in mind a still incipient anthroposophical approach in Plastic Surgery, but with a growing demand due to the needs the specialty requires, a psychiatric SRQ-20 (Self Report Questionnaire) questionnaire was included(10,11). It is a tool for assessing nonpsychotic psycho-emotional disorders (12). Eight or more positive affirmative answers in the assessment ("Yes") indicate that the patient has a significant depression and anxiety profile.
There is a tendency to automate care in centers with high patient loads. The Medical Record model described also allows it to be filled out by the patient in the waiting roam for the fields referring to information the individual him/herself would give. In this case, the patient receives only the first part of the record ["Record N_- 1 (Patient)"], with a questionnaire written in terms and expressions he/she is able to understand.
The information and personal medical background should be dated and acknowledged by the patient with his/her signature on the Medical Record, bearing in mind that many patients, due to their anxiety to undergo plastic surgery, may deliberately or accidentally distort or hide important information. Having the fields filled out in the patients own handwriting presents the advantage of comprising in the future a tool for the physician in case of a lawsuit. Obviously, each item of the questionnaire needs to be checked by the physician, who should correct and take the notes he/she deems necessary in the open optional fields.
The Informed Consent can currendy be considered as a part of the Medical Record or Medical File (13). This is why a standardized Medical Record and Informed Consent are necessary in order to guarantee a healthy physician-patient relationship.
REFERENCES
1. Conselho Regional de Medicina do Estado de São Paulo. Guia da relação médico--paciente. [on line] 2002 [18 telas]. Disponível em: URL: http:// www.cremesp.org.br/revistasermedico/medicopaciente.htm.
2. Resolução do Conselho Federal de Medicina N° 1639/02. Aprovação das "Normas Técnicas para o Uso de Sistemas Informatizados para a Guarda e Manuseio do Prontuário Médico". [on line] 2002; [citado 2002 Ago 25]; [1 tela]. Disponível em URL:http://www.cremesp.org.br/clippings/legislacao_anteriores. php#35
3. Araújo TBC, Malaspina D Jr., Lisbôa AMJ, Pacheco NC, Campos LG, Córdoba JCM. Prontuário Orientado para o Problema. Jornal Pediatria. 1986; 61(4):277-86.
4. Eimerl TS. Curiosidad Organizada: método práctico de resolución del problema del mantenimiento de registros con fines de investigación en el ejercicio general de la Medicina. In: Investigaciones sobre Servicios de Salud: uma antologia. OPS: Oficina Sanitaria Panamericana. Publicación Científica na 534; 1992. p.207-11.
5. Flowers RS, Flowers SS. Precision planning in blepharoplasty Clin Plast Surg. 1993; 20(2):303-10.
6. Souza MSL, Nehmy RMQ, Mendonça, MCLG, Santos AF, Postali VH. Modelo de prontuário ambulatorial pediátrico para informatização - Hospital das Clínicas da Universidade Federal de Minas Gerais. Rev Méd Minas Gerais. 1992; 2(1): 11-4.
7. Gibson N, Bridgman SA. A novel method for the assessment of the accuracy of diagnostic codes in general surgery. Ann R Col Surg Engl. 1998; 80:293-6.
8. Segarra MM, Solano AC. Registros de Salud y Historia Clínica. In: Registros Médicos y de Salud. Módulos de Aprendizaje - Módulo N° 1 Unidad IV Normas generales para la historia clínica. OPS: Oficina Sanitaria Panamericana. Publicación Científica Serie PALTEX na 17; 1991. p.86-90.
9. Sustovich DR, Elias WH, Gebara MS. Observação Clínica. In: Clínica Médica - Propedêutica e Fisiopatologia. 2. ed. Rio de Janeiro: Guanabara- Koogan; 1979. p.3-6.
10. Harding TW, Arango MV, Baltazar J, Climent CE, Ibrahim HHA, Ignácio LL, Murthy RS, Wig NN. Mental disorders in primary health care: a study of their frequency and diagnosis in four developing countries. Psychol Med. 1980; 10:231-41.
11. Mari JJ, Williams P. A comparison of the validity of two psychiatric screening questionnaires (GH Q- 12 and SRQ-20) in Brazil, using relative operating characteristic (ROC) analysis. Psychol Med.5;15:615-59.
12. Mari JJ, Williams P. A validity study of a psychiatric screening questionnaire (SRQ-20) in primary care in the city of São Paulo. Br J Psychiatry. 1986; 148:23-6.
13. Parecer-Consulta do Conselho Federal de Medicina N° 24/97. [on line] 1997; [citado 2002 Jan 25]; [1 tela]. Disponível em URL: http:// www.cfm.org.br/Parecereslnt/1997/24-1997.htm
I - Member of the Brazilian Society of Plastic Surgery, Head Professor of Plastic Surgery of Escola Paulista de Medicina (EPM), Department of Surgery of Universidade Federal de São Paulo (UNIFESP).
II - Member of the Brazilian Society of Plastic Surgery and Post-Graduate Student of the Post-Graduate Plastic Surgery Repair Course of UNIFESP / EPM.
Study performed at the Plastic Surgery Discipline of the Department of Surgery of Universidade Federal de São Paulo (UNIFESP / EPM)
Address for correspondence:
Lydia Masako Ferreira, MD
R. Napoleão de Barros, 715 - 4° andar
04024-900 - São Paulo - SP Brazil
Phone: (55 11) 5576-4118
e-mail: lydia.dcir@epm.br
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket