



Original Article - Year 2018 - Volume 33 -
Tattooing associated with C-V flap placement in one-stage reconstruction of the nipple-areola complex
Tatuagem associada ao retalho em C-V para reconstrução do complexo areolopapilar em tempo único
ABSTRACT
INTRODUCTION: Reconstruction of the nipple-areola complex (NAC) is a fundamental step in the treatment of breast cancer. It is usually performed in two distinct stages. Tattooing is performed only after reconstruction and complete scarring of the nipple.
METHODS: This retrospective study was conducted from 2015 to 2016 at the Hospital São Lucas of the Pontifical Catholic University of Rio Grande do Sul. Twenty-one patients with a single NAC were included. One-stage reconstruction of the nipple using a local C-V flap associated with tattooing for pigmentation of the NAC is described. Data on the type of breast reconstruction performed, associated complications, and presence of previous breast radiotherapy were presented.
RESULTS: Most patients (48%) underwent reconstruction with an implant. Three complications (14%) were observed in the nipple, including one case of partial necrosis and two cases of small dehiscence. None of the patients had complications due to tattooing. Eleven patients (52%) underwent breast radiotherapy previously.
CONCLUSION: Tattooing combined with one-stage reconstruction using a C-V flap is a simple technique with a low rate of complication.
Keywords: Tattooing; Nipples; Breast; Reconstructive surgical procedure; Surgical flap.
RESUMO
INTRODUÇÃO: A reconstrução do complexo areolopapilar (CAP) é etapa fundamental no tratamento do câncer de mama. Tipicamente, é realizada em dois tempos distintos, sendo primeiro a papila reconstruída e somente após sua completa cicatrização que a tatuagem é realizada.
MÉTODOS: Estudo retrospectivo realizado no período de 2015 a 2016 no Hospital São Lucas da PUCRS. Foram incluídas 21 pacientes com ausência do CAP unilateral. É descrita a técnica de reconstrução da papila com retalho local em C-V associado à tatuagem para pigmentação do CAP em tempo único. Foram apresentados os dados referentes ao tipo de reconstrução mamária realizada, às complicações e à presença de radioterapia prévia.
RESULTADOS: A maioria das pacientes foi reconstruída com implante (48%). Houve três complicações relacionadas à papila (14%), uma necrose parcial e duas deiscências pequenas. Não houve complicação relacionada à tatuagem. Onze pacientes (52%) haviam realizado radioterapia prévia na mama.
CONCLUSÃO: A tatuagem associada ao retalho em C-V em tempo único é uma técnica simples e com baixo índice de complicações.
Palavras-chave: Tatuagem; Mamilos; Mama; Procedimentos cirúrgicos reconstrutivos; Retalhos cirúrgicos.
The nipple-areola complex (NAC) is an important structure in breast aesthetics, and NAC reconstruction after mastectomy is essential. It is the last stage of breast cancer treatment.
The breast areola ideally should have the same location, color, and symmetry as the areola on the contralateral side. In addition to these characteristics, the nipple should have an adequate projection. The two known types of areolar reconstruction are skin grafting and tattooing. Grafts and different types of local surgical flaps can be used for nipple reconstruction1-8.
NAC reconstruction is usually performed in two distinct stages, and tattooing is performed only after reconstruction and complete scarring of the nipple9.
OBJECTIVE
To describe the technique and present cases of one-stage reconstruction of the nipple-areola complex by using a local C-V flap associated with tattooing for pigmentation of the NAC.
METHODS
This retrospective study evaluated 21 NAC reconstructions performed using a C-V flap and tattooing between 2015 and 2016 at the São Lucas Hospital of the Pontifical Catholic University of Rio Grande do Sul (Pontifícia Universidade Católica do Rio Grande do Sul-PUCRS), in Porto Alegre, Rio Grande do Sul, Brazil. Data on the type of breast reconstruction performed, associated complications, and presence of previous breast radiotherapy were collected.
For tattooing, a professional tattooing machine with disposable 13-needle tips was used.
Surgical technique
Surgery was performed in the operating room in an outpatient basis, usually 3 to 6 months after completing breast reconstruction.
First, marking was performed with the patient in the orthostatic position, and the location of the NAC was determined using an electrode, with the patient in front of the mirror. The desired circumferences of the areola and nipple were drawn, and then the size of the parts of the C-V flap was marked. The projection of the new nipple was based on the width of the V flaps, and its diameter was based on the diameter of the C flap (Figure 1). These measurements should be larger than initially estimated because of the potential loss of projection postoperatively.

Figure 1. Preoperative marking using the contralateral nipple-areola complex as a reference.
The color of the pigment was also chosen together with the patient, and pigments were mixed until the color obtained was similar to the color of the contralateral side. The chosen color should ideally be a little darker than desired because some degree of bleaching is expected postoperatively.
After local anesthesia with 1% lidocaine and antisepsis with aqueous chlorhexidine, tattooing was initiated with pigmentation of the entire circumference of the NAC, taking care to reach the full depth of the dermis with the needles to ensure that the pigments were absorbed by the body. Then, an incision was made in the previously marked area of the nipple, and the flaps were raised such that the V flaps embraced each other, and the C flap served as a cover.
The donor area was sutured with a few simple subdermal sutures by using vicryl 4.0 followed by mononylon 5.0 for joining the skin. The next step was marking of the circumference of the areola and tattooing the contralateral NAC with pigmentation of its entire circumference (Figure 2). Pigmentation of the contralateral NAC is always performed to ensure that the final color of the two areolas is similar (Figure 3).
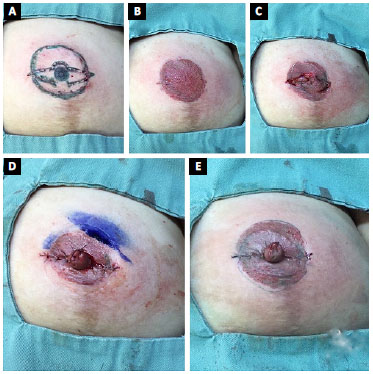
Figure 2. A: Skin marking; B: Tattooing of the entire circumference of the areola, including the skin used to create the C-V flap; C: Incision and assembly of the flaps; D: New marking of the circumference of the areola; E: Tattooing of the new circumference of the areola and immediate final result.

Figure 3. A: Preoperative marking in a patient with a previous reconstruction using a transverse myocutaneous flap of the rectus abdominis; B: Immediate postoperative result. Note the tattooing of the original nipple-areola complex to ensure that the color was similar to that of the contralateral side.
The dressing was performed using petroleum gauze and neomycin ointment, taking care to keep a cushion of punctured gauze in the center to prevent compressing the flap. The dressing remained closed for 4 days, and the patient was instructed to make new dressings using gauze and liquid vaseline for at least 1 month. The stitches were removed after 10 to 14 days.
RESULTS
From 2015 to 2016, the procedure was performed in 21 patients. A single NAC was absent in all the cases. Ten patients (48%) had a previous breast reconstruction with implants, 5 (24%) with a myocutaneous flap from the rectus abdominis, 3 (14%) with a myocutaneous flap from the latissimus dorsi, and one (5%) with a fat graft. Two patients (9%) had a previous conservative breast surgery (a sector with NAC resection). Eleven patients (52%) had a previous breast radiotherapy.
Three complications occurred in the nipple (14%), including one case of partial necrosis and two cases of small dehiscence. None of the patients had any complications related to tattooing (Table 1). None of the evaluated patients needed retouch of the tattooing of the reconstructed NAC in the 2-year follow-up period (Figure 4). One patient needed to increase the size of the contralateral areola by tattooing to maintain diameter symmetry.
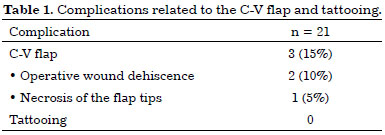
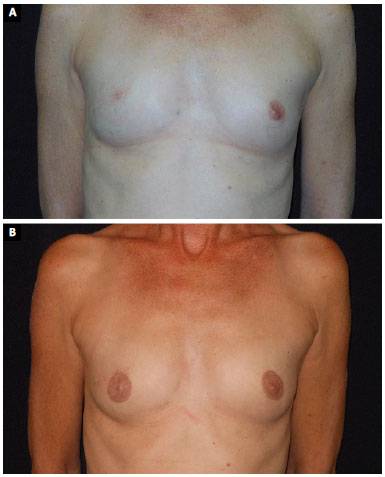
Figure 4. A: Patient with small breasts treated with right skin-sparing mastectomy and late two-stage reconstruction with a fat graft; B: Result 1 year after reconstruction of the right nipple-areola complex and bilateral tattooing with an increase in the circumference of the original areola.
DISCUSSION
Several surgeries are performed during breast reconstruction, and NAC reconstruction is usually the last step. The projection, size, color, and shape of the NAC have been emphasized in the literature as determinants of patient satisfaction10-12.
The ideal technique for NAC reconstruction should be simple, reproducible, and free from complications, and the final result should be aesthetically pleasing. We believe that the described technique meets all these criteria. The C-V flap used ensures that the nipple has an adequate shape and projection. Tattooing allows pigmentation of the areola and nipple with a color similar to that on the contralateral side and does not have the morbidity associated with skin grafts. The wide variety of pigment colors available in the market allows for a simple and reliable choice, and the results are consistent over time. When tattooing is bleached, skin darkening can be performed in the medical clinic.
Rees13 was the first author to report the use of tattooing for NAC pigmentation. Although teaching tattooing to plastic surgeons is still limited, we believe that the learning curve is low. Medical tattooing is a simple procedure with a high level of patient satisfaction9. The procedure is safe, and the rate of complication is low. Moreover, no complications such as infections, allergies, or delayed healing were observed.
Liliav et al.9 described a similar technique for NAC reconstruction and found that all 18 patients were satisfied and only 17% presented complications (14% with inadequate pigment integration and 3% with dehiscence). The rate of complication in our study was 14%. However, in contrast to the above study, none of the cases had inadequate pigment integration, and the most common complication was dehiscence, with two cases. The objective of this study was not to report the degree of patient satisfaction with the proposed technique. However, we are conducting a study on this subject, which is fundamental when analyzing a surgical technique.
Valdatta et al.14 described a similar technique in two distinct stages and observed that the degree of patient satisfaction was high, and the loss of projection of the reconstructed nipples was 29% as compared with the original nipples. This result indicates the importance of using flaps that are a little larger than desired. In the above study, surgical planning was performed in two stages (first the reconstruction of the nipple and then tattooing), in contrast to our study, whereby tattooing and nipple flap placement were performed at the same time. This one-stage strategy is one of the main advantages of this technique. Therefore, as reported by Valdatta, most of the authors first perform nipple reconstruction, although the techniques used are highly variable14-19. In a second stage, usually 3 months after, tattooing is performed for NAC pigmentation. Reducing the number of surgeries was believed to have provided improved value and comfort to patients who underwent breast reconstruction.
Three-dimensional tattooing of the NAC is possible for most patients, with excellent results20. We believe that maintaining the shape of the nipple is essential during reconstruction; for this reason, we have not practiced this technique. A nipple with a defined shape is desired by most patients.
Spear and Arias21 retrospectively evaluated 151 patients for 6 years, with a mean follow-up of 2 years, and found that retouching because of pigment bleaching was necessary in only 10% of the cases and the degree of patient satisfaction was high. In our experience, retouching to enhance pigmentation was not necessary, although the short follow-up period did not allow a more accurate analysis.
CONCLUSION
NAC reconstruction is an essential step in breast reconstruction for restoring the self-esteem of women affected by breast cancer. Tattooing associated with one-stage reconstruction using a C-V flap is simple, has a low complication rate, and can be performed by any trained plastic surgeon who intends to perform breast reconstruction.
COLLABORATIONS
FFL Analysis and/or interpretation of data; final approval of the manuscript; conception and design of the study; completion of surgeries and/or experiments; writing the manuscript or critical review of its contents.
FLN Conception and design of the study; writing the manuscript or critical review of its contents.
MPO Analysis and/or interpretation of data; conception and design of the study; writing the manuscript or critical review of its contents.
REFERENCES
1. Farhadi J, Maksvytyte GK, Schaefer DJ, Pierer G, Scheufler O. Reconstruction of the nipple-areola complex: an update. J Plast Reconstr Aesthet Surg. 2006;59(1):40-53. PMID: 16482789 DOI: http://dx.doi.org/10.1016/j.bjps.2005.08.006
2. Kroll SS, Hamilton S. Nipple reconstruction with the double-opposing-tab flap. Plast Reconstr Surg. 1989;84(3):520-5. PMID: 2762412 DOI: http://dx.doi.org/10.1016/j.bjps.2005.08.006
3. Weiss J, Herman O, Rosenberg L, Shafir R. The S nipple-areola reconstruction. Plast Reconstr Surg. 1989;83(5):904-6. DOI: http://dx.doi.org/10.1097/00006534-198905000-00026
4. Chang WH. Nipple reconstruction with a T flap. Plast Reconstr Surg. 1984;73(1):140-3. DOI: http://dx.doi.org/10.1097/00006534-198401000-00035
5. Thomas SV, Gellis MB, Pool R. Nipple reconstruction with a new local tissue flap. Plast Reconstr Surg. 1996;97(5):1053-6. DOI: http://dx.doi.org/10.1097/00006534-199604001-00027
6. Schoeller T, Schubert HM, Pülzl P, Wechselberger G. Nipple reconstruction using a modified arrow flap technique. Breast. 2006;15(6):762-8. DOI: http://dx.doi.org/10.1016/j.breast.2006.03.010
7. Little JW 3rd, Munasifi T, McCulloch DT. One-stage reconstruction of a projecting nipple: the quadrapod flap. Plast Reconstr Surg. 1983;71(1):126-33. PMID: 6336842 DOI: http://dx.doi.org/10.1097/00006534-198301000-00029
8. Hartrampf CR Jr, Culbertson JH. A dermal-fat flap for nipple reconstruction. Plast Reconstr Surg. 1984;73(6):982-6. PMID: 6728951 DOI: http://dx.doi.org/10.1097/00006534-198406000-00027
9. Liliav B, Loeb J, Hassid VJ, Antony AK. Single-stage nipple-areolar complex reconstruction technique, outcomes, and patient satisfaction. Ann Plast Surg. 2014;73(5):492-7. PMID: 24135688 DOI: http://dx.doi.org/10.1097/SAP.0b013e318276dac0
10. Wellisch DK, Schain WS, Noone RB, Little JW 3rd. The psychological contribution of nipple addition in breast reconstruction. Plast Reconstr Surg. 1987;80(5):699-704. DOI: http://dx.doi.org/10.1097/00006534-198711000-00007
11. Goh SC, Martin NA, Pandya AN, Cutress RI. Patient satisfaction following nipple-areolar complex reconstruction and tattooing. J Plast Reconstr Aesthet Surg. 2011;64(3):360-3. PMID: 20570584 DOI: http://dx.doi.org/10.1016/j.bjps.2010.05.010
12. Buck DW 2nd, Shenaq D, Heyer K, Kato C, Kim JY. Patient-subjective cosmetic outcomes following the varying stages of tissue expander breast reconstruction: the importance of completion. Breast. 2010;19(6):521-6. DOI: http://dx.doi.org/10.1016/j.breast.2010.05.017
13. Rees TD. Reconstruction of the breast areola by intradermal tattooing and transfer. Case report. Plast Reconstr Surg. 1975;55(5):620-1. PMID: 1144541 DOI: http://dx.doi.org/10.1097/00006534-197505000-00019
14. Valdatta L, Montemurro P, Tamborini F, Fidanza C, Gottardi A, Scamoni S. Our experience of nipple reconstruction using the C-V flap technique: 1 year evaluation. J Plast Reconstr Aesthet Surg. 2009;62(10):1293-8. PMID: 18691957 DOI: http://dx.doi.org/10.1016/j.bjps.2008.03.064
15. Eo S, Kim SS, Da Lio AL. Nipple reconstruction with C-v flap using dermofat graft. Ann Plast Surg. 2007;58(2):137-40. PMID: 17245138 DOI: http://dx.doi.org/10.1097/01.sap.0000235445.86570.80
16. Delay E, Mojallal A, Vasseur C, Delaporte T. Immediate nipple reconstruction during immediate autologous latissimus breast reconstruction. Plast Reconstr Surg. 2006;118(6):1303-12. PMID: 17051099 DOI: http://dx.doi.org/10.1097/01.prs.0000244013.11974.ec
17. Nahabedian MY. Nipple reconstruction. Clin Plast Surg. 2007;34(1):131-7. DOI: http://dx.doi.org/10.1016/j.cps.2006.11.009
18. Anton MA, Eskenazi LB, Hartrampf CR Jr. Nipple reconstruction with local flaps: star and wrap flaps. Perspect Plast Surg. 1991;5(1):67-78. DOI: http://dx.doi.org/10.1055/s-2008-1080415
19. Jones G, Bostwick J III. Nipple-areolar reconstruction. Oper Technol Plast Reconstr Surg. 1994:1(1):35-38. DOI: http://dx.doi.org/10.1016/S1071-0949(10)80017-4
20. Halvorson EG, Cormican M, West ME, Myers V. Three-dimensional nipple-areola tattooing: a new technique with superior results. Plast Reconstr Surg. 2014;133(5):1073-5. PMID: 24776543 DOI: http://dx.doi.org/10.1097/PRS.0000000000000144
21. Spear SL, Arias J. Long-term experience with nipple-areola tattooing. Ann Plast Surg. 1995;35(3):232-6. PMID: 7503514 DOI: http://dx.doi.org/10.1097/00000637-199509000-00002
1. Sociedade Brasileira de Cirurgia Plástica, São Paulo, SP, Brazil
2. Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, RS, Brazil
3. Hospital São Lucas, Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, RS, Brazil
4. Instituto do Câncer, Hospital Mãe de Deus, Porto Alegre, RS, Brazil
Institution: Hospital São Lucas, Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, RS, Brazil.
Corresponding author:
Francisco Felipe Laitano
Avenida Ipiranga, 6690, conjunto 520 - Jardim Botânico
Porto Alegre, RS, Brazil - Zip Code 90160-090
E-mail: fflpoa@hotmail.com
Article received: August 28, 2017.
Article accepted: October 19, 2017.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket