



Articles - Year 2002 - Volume 17 -
Indication of CO2 and Erbium Lasers
Indicações do Uso dos Lasers de CO2 e Erbium
ABSTRACT
The exact indications of CO2 and Erbium laser are discussed with the objective of attaining better esthetic results and decreasing morbidity. Indications are based on the knowledge of tissue interaction of each laser; and technical details of the procedure based on 6-year experience in laser resurfacing.
Keywords: Laser; resurfacing; erbium versus CO2
RESUMO
As indicações precisas do laser dos tipos CO2 e Erbium são discutidas no intuito de apresentar um melhor resultado estético e diminuir a morbidade.
As indicações são baseadas no conhecimento da interação tecidual de cada laser, apresentando detalhes técnicos de execução resultante de uma experiência de 6 anos em resurfacing laser.
Palavras-chave: Laser; resurfacing; erbium versus CO2
As of 1991, the pursuit of youth found one more ally it could rely on, that is to say, UltraPulse technology, which made it possible to use CO2 laser on the face (resurfacing) through the accurate control of thermal damage.
Since then, facial resurfacing has gone through a phase of maturing and seeking new technology in order to overcome the failures inherent to the procedure, fill out gaps and even avoid complications, thus leading to a new phase of indications and its current scenario.
Resurfacing, contrary to what some advocate, has come to stay. It has exact indications and handling requirements. Knowledge of tissue interaction is important in order to obtain increasingly better results and avoid complications.
We will analyze the best indications for each laser - CO2 and Erbium -, based on their specific tissue interactions.
MATERIALS AND METHODS
From March 1996 to April 2001, 649 patients underwent surgery, utilizing the CO2 Ultrapulse (Coherent, Inc. Palo Alto, Cal) and Erbium YAG Ultrafine (Coherent, Inc. Palo Alto, Cal) lasers. Total and partial resurfacing procedures were performed, using each type of laser separately and together (both side by side, as well as one over the other).
Initially, we had only the CO2 laser, but given the difficulties involved in using only one kind of laser, we decided on a new strategy, which led to the use of Erbium.
C02 LASER
The CO2 laser has a 10.6 mm wavelength and operates on the invisible portion of the electromagnetic spectrum; its chromophore is water.
This kind of laser has been used for a long time, which made it possible to observe its advantages as well as its disadvantages in some sectors.
Based on these observations, new studies have been performed in order to look for other options to supplement possibilities of utilization, according to the demand for different indications.
ERBIUM LASER
Erbium laser, used since 1989 in dermatology, has a 2.94 mm wavelength. Its chromophore is also water. Based on its properties, it has contributed to some indications in which the C02 laser is restricted.
TISSUE INTERACTION
Both CO2 and Erbium lasers have water as a chromophore. Water, however, absorbs the latter, (Erbium), 10 times more than the former (C02).
CO2 ablation is between 50-100 um (at 7.6 J/cm2) per application, while Erbium promotes 10-20 um ablation (at 5-10 J/cm2). Thermal damage for CO2 is between 50-150 um, and roughly 10-20 um for Erbium.
As a result of the greater absorption of Erbium by water, more energy is consumed on the surface, resulting in transmission of less energy to surrounding tissues, which results in a smaller thermal damage zone.
Whenever C02 laser is used, there is significant shrinking of collagen in the thermal damage zone, which stimulates the formation of new collagen. However, with Erbium, new collagen with a flowing above 20 J/cm2 (20 HZ-300/0 overlap) has been observed.
Greater hemostasia power also results from CO2's greater thermal effect, a fact not observed with Erbium. Therefore, once the comparative information on tissue interaction with both lasers is obtained, the features of each one may be better understood.
CHARACTERISTICS OF THE C02 LASER
• The first application removes the epidermis.
• The second and third applications make collagen shrink; a controlled thermal effect is produced.
• Subsequent applications will have little ablative effect due to the lack of the chromophore (water), resulting in cumulative thermal effects, impossible to anticipate or control.
• Smaller ablative effect and greater thermal effect.
• Haemostatic effect that may be used for cutting.
• Stimulates pigment formation.
• Has a cumulative thermal effect.
CHARACTERISTICS OF ERBIUM LASER
• Each application will remove the same amount of tissue, although the removal capability is 10 times less than that of CO2.
• Ablates collagen and may continue throughout the entire depth of the skin. As it does not have a major thermal effect, as it has a chromophore, ablation may be continuous. That is the reason why Erbium laser is called ablative.
• Less of a thermal effect and greater ablative effect. The advantage of Erbium laser is that it allows for the possibility of eliminating pigment without a large stimulus for yielding new pigment.
• May remove thermal damage of CO2, praviding tissue epithelialization based on vascularized cells.
• Succesive ablative effect.
• More superficial ablation, demanding therefore, a larger number of applications.
• Deeper ablation from the papilar dermis leads to bleeding.
• Does not shrink collagen with fluence below 20 J/cm2(2).
INDICATIONS
After acquiring information on the basic physical data, tissue interaction and background of both kinds of laser, the best indications for each type of laser may be pointed out (Table I).

SKIN BLEMISHES (MELASMA, ASIANS, NECK, HANDS, EYELID HYPERPIGMENTATION AREAS)
Erbium is indicated in these cases because it removes superficial cells that contain excess melanin, and it also removes melanocytes. As it does not have a rebound effect as to hyper-pigmentation because of the minimal residual thermal effect, it does not stimulate new hyper-pigmentation.
These situations should be handled in the preoperative period with clarifiers for 2 to 3 months with at least pigmentation reduction. We associate glycolic acid and kojic acid in one product or tretinoin and hydroquinone in another, in progressive percentages.
The postoperative use of clarifiers and sun block, and non-exposure to the sun are very important. There may be recurrence if postoperative care in not followed, specifically for melasma.
In the eyelid hyper-pigmentation areas, the results have proven to be definite in a 3-year observation period, without the requirement of clarifiers in the long term (Figs. 1a-b and 2a-b).
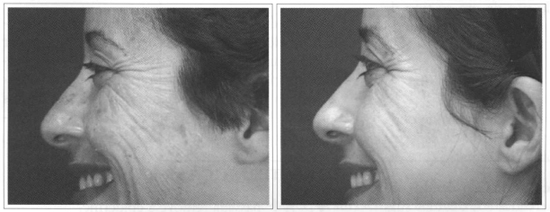
Fig. 1 - Face blemishes. Total face resurfacing with Erbium laser. A) Preoperative. B) 6 months
postoperative.
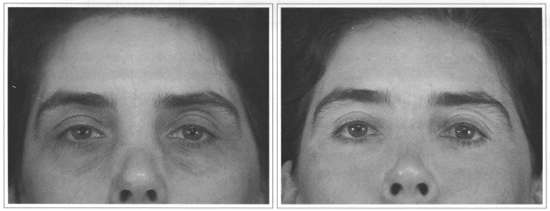
Fig. 2 - Eyelid hyper-pigmentation. Partial resurfacing with Erbiurn laser. A) Preoperative. B) 13 months postoperative.
WRINKLES
Fine wrinkles are treated well with Erbium, although moderate and deep, fine ones are treated well with CO2. Whenever skin shrinkage and greater collagen remodeling is called for, such as in more photo-aged skins or with deeper or widespread wrinkles, Ultrapulse CO2 is indicated, while Erbium Ultrafinee may be used for refining wrinkle borders of transition areas. Erbium alone is indicated for young patients with localized wrinkles such as perioral ones, for example. If wrinkles are deep and invade the vermillion, a sole application of CO2 on the vermillion may be performed (Figs. 3a-b and 4a-b).
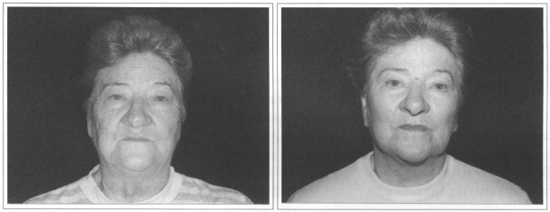
Fig. 3 - Widespread wrinkles (photo-aging Grade III). Total resurfacing with C02 laser. A) Preoperative. B) Postoperative.
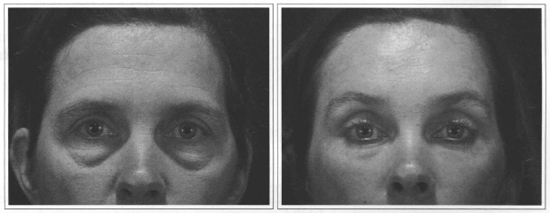
Fig. 4 - Lower eyelid laxity. Lower eyelid resurfacing with CO2 laser + diminished Energy with Erbium laser. A) Preoperative. B) Nine months postoperative.
SKIN LESIONS
Epidermal or dermal superficial skin lesions such as epidermal nevus, keratosis, syringoma, xanthelasma, etc. are laser treatable. They may be submitted to biopsy for diagnosis and have the advantage of not leaving a scar.
As many applications are necessary for total ablation of the lesion, the best indication is Erbium, because it is an ablative laser in each application. The smaller thermal effect allows the preservation of a greater amount of chromophore, that is to say water, which continues the ablation (Figs. 5a-b).

Fig. 5 - Epidermal face Nevus verrucoso. Erbium Laser. A) Preoperative. B) Four months postoperative.
SCARS
Scars, per se, have poor blood flow and this situation should not be worsened by larger thermal effects. Since many applications are necessary for treating hypertrophic or unleveled scars, the best indication would be Erbium.
SHRINKAGE OF LOWER EYELID SKIN
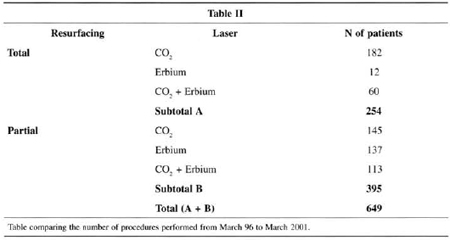
Table II compares the number of procedures performed from March/96 to March/2001, and shows a change in the standards for indicating total or partial resurfacing.
CO2 is best indicated for total face resurfacing due to the risk of delimitation between the treated and non -treated area. It is wise to use Erbium at the transition between the area treated with CO2 and the untreated area (tine of the mandible).
Partial resurfacing is more freguently indicated for the lower eyelid and peri-oral region(5).
CO2 is fundamental for the lower eyelid region, in most cases, in order to treat eyelid laxity by skin shrinkage, replacing lower transcutaneous blepharoplasty. CO2 is used in the orbital portion of the lower eyelid, and Erbium is used in the peri-orbital region, where only treating fine wrinkles and the transition with untreated skin is desired.
Likewise, the area with deeper wrinkles in the perioral region may be treated with CO2, and Erbium applied on the remaining region and transition.
In patients with fine wrinkles on the eyelid or perioral regions, only Erbium, which is more superficial and yields less thermal damage, and does not change skin texture, should be used.
Indication also takes into account other important factors, such as blemishes and vessels. CO2 should be indicated for total face primarily due to the greater texture and structural changes in skin, leaving Erbium for partial areas with fewer changes due to aging.
ACNE SEQUELA
It comprises the precise circumstances for joint use, because we need shrinkage and ablation to maximize results.
We maximize our results by using CO2 twice (E-300mJ - Density 7), we sculpture lesions with Erbium 2 or 3 times (E-8 mJ/cm2- - Ultrafine - Cohrerent) and on the borders of atrophic lesions, and use CO2 once or twice (E -250 mJ - Density 5 or 6).
We therefore perform resurfacing on thick skins, type 3, 4 and 5 and consider, in these cases, resurfacing more elaborate and challenging. Aggressive resurfacing (deep) is not recommended for type 1 or 2 skins due to the risk of hypo-pigmentation. This management (aggressive) should be left for after a long learning and experience curve with post-laser follow-up (Figs. 6a-b).
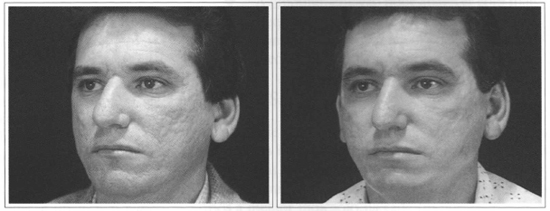
Fig. 6 - Acne Sequelae. Total Resurfacing with CO2 and Erbium laser. A) Preoperative. B) Three months postoperative.
FACE TELANGIECTASIAS
An important factor to be considered when indicating resurfacing is the presence of face telangiectasias, because, under CO2, there may be occlusion of capillaries, leaving a hipovascularization area bordering the treated region.
Erbium alone should be considered for patients with this type of condition, mainly for partial resurfacing. If CO2 is necessary for skin shrinkage (lower eyelid, for example), it is better to treat telangiectasias, in a single stage, with a vascular laser.
A particularly relevant situation to be assessed and diagnosed during the preoperative period is Civatte's poikiloderma. Resurfacing with CO2 may lead to a delimitation area on the mandible line.
CO2 resurfacing would only be an adjuvant treatment for face telangiectasias. However, the presence of telangiectasias also in the central region, leading to a delimitation line, should be considered.
In the cases described above, less energy should always be used in peripheral areas, mainly near the mandible line, and resurfacing finished with Erbium on the transition area.
HANDS AND NECK DYSCHROMIA
Erbium may be used once or twice at low-fluence in patients with hands or neck dyschromia.
POSTOPERATIVE EVOLUTION: COMPARISON BETWEEN CO2 AND ERBIUM
Eritema and Healing Time: will be directly proportional to the depth of resurfacing (Figs. 7a-b).

Fig. 7 - A) Light resurfacing with Erbium. B)Deep resurfacing with Erbium.
The level of penetration with identical depths results in the same duration of eritema, and demands the same recovery period.
Hyper-pigmentation: Erbium has fewer cases of hyper-pigmentation and, when it occurs, it lasts 2 to 4 weeks on average. With CO2 Laser, on the other hand, hyper-pigmentation remains for up to 8 weeks.
Hypo-pigmentation: Late occurrence (after 1 year), hypo-pigmentation is related to various factors, such as:
• Depth of resurfacing.
• Removal of more external skin layers, where aged melanin is deposited.
• Destruction of melanocytes.
• Fibrosis network that prevents visualization of melanin, higher incidence in light skin because they are more translucid, showing the white color.
• Hypo-pigmentation may appear more frequently in C02 laser resurfacing, although it may also occur with Erbium, due to the melanocyte ablation mechanism.
DISCUSSION
Based on the drawbacks and complications found during the initial utilization of CO2 and the applicability of new technologies, we have pursued safer resurfacing. Better results may be obtained when the best indication for each laser is followed.
Knowledge of tissue interaction and the concept of the best indication for each are the main reasons for using the adequate laser in esthetic and reconstruction surgery.
CONCLUSION
The scenario for laser surgery has changed in relation to indication. A trend for using laser surgery as a supplement to conventional surgery has been observed. Greater utilization has been seen for partial resurfacing or joint use of CO2 and Erbium, one supplementing the other, taking advantage of the best indications of each one.
The major issue, however, is the prevention of complications. In cases of area delimitation, non-total removal of wrinkles, or poor result for acne sequelae, these approaches produced improved results. For complications such as hypo-pigmentation and scars, nonetheless, preventive work and respecting the correct indication for both kinds of lasers, CO2 and Erbium, is fundamental.
REFERENCES
1. Apfeliberg DB. A Critical appraisal of high-energy pulsed carbon dioxide laser facial resurfacing for acne scars. Ann Plast Surg. 1997; 38(2):95-100.
2. Weinstein C. Computerized scanning Erbium:YAG laser for skin resurfacing. Dermatol Surg. 1998; 24(1):83-9.
3. Weinstein C. Endoscopic forehead lift. Face-lifting procedures. 1997; 27:421-7.
4. Ramirez OM, Pozner JN. Subperiosteal minimally invasive laser endoscopic rhytidectomy: the SMILE facelift. Aesth Plast Surg. 1996; 20(6) :463-70.
5. Alster TS. Manual of Cutaneous Laser Techniques. New York: Raven; 1997. p.145-9.
6. Treikemeier G, Goldberg DI. Skin resurfacing with the Erbium: YAG laser Dermatol Surg. 1997; 23:685-7.
7. Kaufmann R, Hibst R. Pulsed Erbiwn: YAG laser ablation in cutaneous surgery. Lasers Surg Med. 1996; 19:324-30.
8. Dmovsek-Olup B, Vedlin B. Use ofEr: YAG laser for benign skin disorders. Lasers Surg Med. 1997; 21(1):13-9.
9. Kye YC. Resurfacing of pitted facial scars with a pulsed Erbiwn: YAG laser. Dermatol Surg. 1997; 23:880-3.
10. Adrian RM. A Clinical and histologic comparison of Erbiwn: YAG laser and pulse CO2 laser in the treatment of rhytids. In: 18th Annual Meeting American Society for Laser Medicine and Surgery; 1998 Apr 5; San Diego, California.
11. Tanghetti EA, Adrian RM. Long pulse 532 nm laser treatment of facial telangiectasias. In: 18th Annual Meeting American Society for Laser Medicine and Surgery; 1998 Apr 6; San Diego, California.
12. Badin AZD, Moraes LM, Roberts TRIII. Rejuvenescimento facial a laser. Rio de Janeiro: Revinter; 1998. p. 472.
13. Badin AZD, Casagrande C, Roberts TIIII, Saltz R, Moraes LM, Santiago M, Chiaratti M. Minimally invasive facial rejuvenation endolaser midface lift. 2001; 25(6):447-53
14. Badin AZ, Moraes L, d'Almeida NM. Um raio de luz: rejuvenescimento facial a laser.São Paulo:CLR Balieiro; 1997. p.llO.
15. Badin AZ, Moraes L. Laser CO2 In: Horibe EK. Estética clínica e cirúrgica. Rio de Janeiro; 2000.p.93-104.
I - Senior Member of SBCP
Address for correspondence:
Ana Zulmira Diniz Badin, MD
R. Des. Vieira Cavalcanti, 590
80510-090 - Curitiba - PR Brazil
Phone: (5541) 223-8886 - Fax: (5541) 323-1392
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket