



Original Article - Year 2019 - Volume 34 -
Epidemiological profile of patients with cleft lip and palate in a reference service in the Federal District
Perfil epidemiológico de pacientes portadores de fissuras labiopalatinas em serviço de referência no Distrito Federal
ABSTRACT
Introduction: Cleft lip and palate, the most common congenital malformations of the head and neck, result from fusion failure of embryonic facial processes during the first 12 weeks of pregnancy. Their phenotypic presentation varies and involves different levels of complexity. The objective is to determine the epidemiological profile of patients with cleft lip and palate treated at the Hospital Regional da Asa Norte regarding sex, cleft type, laterality, age, presence of associated syndromes, and corrective surgical procedures.
Methods: This was a retrospective descriptive study of 322 medical records of patients treated by the HRAN team from August 2013 to July 2017. The data collected were entered into an Excel spreadsheet and submitted to statistical analysis. The study received ethical approval.
Results: Of the 322 patients enrolled in the service, 169 were male (52.48%). The most frequent type of cleft was the trans-foramen (65.25%). With regard to laterality, a higher prevalence of cleft was observed on the left (20.50%). Only 19% of the patients had associated malformations. Cheiloplasty was the most frequent surgical correction performed by service (54%). The age of the patients was 1-53 years (median, 1.87 years).
Conclusion: The study contributes information important to society, government, and treatment professionals. In line with the literature, the more prevalent cleft was unilateral left trans-foramen and the most frequent surgery was cheiloplasty.
Keywords: Cleft palate; Cleft lip; Descriptive epidemiology; Reconstructive surgical procedures; Congenital abnormalities
RESUMO
Introdução: As fissuras labiopalatinas são as malformações congênitas mais comuns dentre as que ocorrem na cabeça e pescoço, e se devem à falha de fusão dos processos faciais embrionários durante as primeiras 12 semanas de gestação. Sua apresentação fenotípica é variada e com diferentes níveis de complexidade. O objetivo é determinar o perfil epidemiológico dos pacientes portadores de fissuras labiopalatinas atendidos no Hospital Regional da Asa Norte (HRAN) quanto a sexo, tipo de fissura, lateralidade, idade, presença de síndromes associadas e procedimentos cirúrgicos corretivos.
Métodos: Trata-se de um estudo descritivo retrospectivo no qual foram analisados 322 prontuários de pacientes atendidos pela equipe do HRAN no período de agosto de 2013 a julho de 2017. Os dados colhidos foram lançados em planilha Excel e submetidos à análise estatística. O trabalho foi aprovado pelo Comitê de Ética e Pesquisa.
Resultados: Dos 322 pacientes atendidos no serviço, 169 eram do sexo masculino (52,48%). O tipo de fissura mais frequente foi a transforâmica (65,25%). Com relação à lateralidade, observou-se maior predomínio da fissura à esquerda (20,50%). Apenas 19% dos pacientes possuem malformações associadas. A queiloplastia foi a correção cirúrgica mais realizada pelo serviço (54%). A idade dos pacientes variou de 1 ano até 53 anos, com mediana de 1,87 anos.
Conclusão: O estudo contribuiu com informações importantes para a sociedade, governo e profissionais envolvidos no tratamento. Em consonância com a literatura, observou-se que a fissura mais prevalente foi a transforâmica unilateral esquerda e a cirurgia mais realizada foi a queiloplastia.
Palavras-chave: Fissura palatina; Fenda labial; Epidemiologia descritiva; Procedimentos cirúrgicos reconstrutivos; Anormalidades congênitas
INTRODUCTION
Cleft lip and palate, the most common congenital malformations that affect the head and neck, occur due to lip and palate fusion failure in intrauterine life1-3. They can be divided into isolated cleft lip, cleft palate, and cleft palate3-6. The prevalence of this disease is uncertain, but it affects approximately 1 in every 700 live births depending on factors such as ethnicity, geographical origin, and socioeconomic level4. It may occur in isolation or associated with syndromes. It is estimated that 50–70% of clefts occur in isolation or in a non-syndromic form1,4.
The frequency of cleft lip and palate differs between the sexes. While cleft lip with or without cleft palate affects more males, the presentation is inverted with isolated cleft palate, which affects more females at a ratio of 2:1. As for laterality, unilateral cleft lip is more prevalent on the left side than the right, also by a ratio of 2:12,4,7-9.
The etiology is diverse and uncertain due to embryological error, being influenced by genetic, environmental, and socioeconomic factors1,4. Studies indicate that smoking, drugs, parents’ age, social class, consanguinity, and ethnicity are involved in the onset of this malformation, relating in different ways to the occurrence of fissures1,4,5,10,11. Gestational history, drug use, and family history are essential to possible associated genetic factors. Folic acid is a protective factor7.
Based on embryological origin, Spina proposed a classification of clefts considering their position in relation to the incisive foramen. In group I, complete pre-incisive foramen cleft, which affects the lip, dental alveolus, and nasal floor, and incomplete, which affects only the lip. Group II includes trans-incisive foramen clefts. Group III refers to clefts that only affect the palate, which can be complete or incomplete. Cleft lip and palate can be unilateral or bilateral5,7.
The diagnosis of oral clefts can be done during prenatal monitoring with ultrasound. Hard palate clefts are difficult to visualize and can only be diagnosed after the 28th week. Thus, in general, only cleft lip is diagnosed in the early prenatal period during the first trimester7,12,13. Surgical correction of oral clefts can occur according to the cleft type presented and the treatment protocol established by each service7,14,15.
OBJECTIVE
Few studies have assessed the epidemiological profile of patients with oral clefts, especially in Brazilian territories. Given the need to better understand this profile, the present study aims to describe the frequency of cleft types and the prevalence of surgical procedures in patients with cleft lip and palate who attended and underwent surgery at the Multidisciplinary Service of Care for Patients with Cleft Lip and Palate of the Hospital Regional da Asa Norte (HRAN), Brasília, Federal District (DF).
METHODS
This retrospective descriptive study was performed at the Multidisciplinary Service of Care for Patients with Cleft Lip and Palate of the HRAN located in the city of Brasília, DF. This is a medium-sized hospital and a reference center for the care of patients with cleft lip and palate in the Midwest region. The present study was approved by the Ethics and Research Committee of the Health Sciences Teaching and Research Foundation (FEPECS) (protocol 53767715.4.0000.5553) and conducted in accordance with Resolution No. 196/96, which oversees research involving human beings.
The study population comprised all patients undergoing surgical procedures of the Multidisciplinary Service of Care for Patients with Cleft Lip and Palate between August 2013 and July 2017. Patients for whom information was missing from their medical records were excluded from the study.
The researchers collected data from the medical records of patients diagnosed with cleft lip and palate in an Excel spreadsheet. The variables analyzed included date of surgery, patient sex, patient age at surgery, surgery performed, diagnosis according to Spina classification, laterality of clefts, and family history of clefts and associated anomalies. Subsequently, a statistical analysis was performed with the proportions tests and Chi-square test using R software for Windows.
RESULTS
Between August 2013 and June 2017, 586 patients were surgically treated in this service, but only 322 met the study’s inclusion criteria. Of the 322 patients enrolled in the service, 169 were male (52.48%). Patient age ranged from less than 1 year to 53 years, with a median of 1.87 years.
Patient origin was variable. The reference service assists the Federal District and surrounding areas. However, some patients are from the North and Northeast regions of Brazil.
Patient Diagnosis
For both sexes, the left and bilateral foramen clefts were the most prevalent (20.50% and 18.94%, respectively). The proportions test yielded a p value of 0.6098. As observed in Table 1, in males, the most common clefts were bilateral trans-foramen (21.30%), left trans-foramen (18.93%), and right trans-foramen clefts (15.38%). The proportions test yielded a p value of 0.2974. In females, the more frequent clefts were left trans-foramen (22.22%), bilateral trans-foramen (16.34%), and incomplete post-foramen clefts (16.34%) (p = 0.2354).
| Diagnosis (cleft) | Male | Percentage | Female | Percentage | Total | Percentage |
|---|---|---|---|---|---|---|
| Incomplete left pre-foramen | 14 | 8.28% | 11 | 7.19% | 25 | 7.76% |
| Incomplete right pre-foramen | 6 | 3.55% | 9 | 5.88% | 15 | 4.66% |
| Bilateral incomplete pre-foramen | 3 | 1.78% | 0 | 0.00% | 3 | 0.93% |
| Complete left pre-foramen | 9 | 5.33% | 7 | 4.58% | 16 | 4.97% |
| Complete right pre-foramen | 14 | 8.28% | 11 | 7.19% | 25 | 7.76% |
| Bilateral complete pre-foramen | 3 | 1.78% | 3 | 1.96% | 6 | 1.86% |
| Left trans-foramen | 32 | 18.93% | 34 | 22.22% | 66 | 20.50% |
| Right trans-foramen | 26 | 15.38% | 16 | 10.46% | 42 | 13.04% |
| Bilateral trans-foramen | 36 | 21.30% | 25 | 16.34% | 61 | 18.94% |
| Complete post-foramen | 11 | 6.51% | 12 | 7.84% | 23 | 7.14% |
| Incomplete post-foramen | 15 | 8.88% | 25 | 16.34% | 40 | 12.42% |
| Total | 169 | 100.00% | 153 | 100.00% | 322 | 100.00% |

Cleft Laterality
Initially, the frequency of laterality (uni- and bilateral) of the most common clefts, pre-foramen and trans-foramen clefts of patients, in general and by sex (Table 2) were analyzed. In the study population, a left unilateral cleft was the most common in both sexes. Thereafter, the prevalence of pre- and trans-foramen clefts was analyzed by sex and in general (Table 3) since they were the most common in both sexes. As the proportion test revealed a p value less than 0.001, the trans-foramen clefts are more prevalent.
| Laterality | Male | Percentage | Female | Percentage | Total | Percentage |
|---|---|---|---|---|---|---|
| Right unilateral | 46 | 32.17% | 36 | 31.03% | 82 | 31.66% |
| Left unilateral | 55 | 38.46% | 52 | 44.83% | 107 | 41.31% |
| Bilateral | 42 | 29.37% | 28 | 24.14% | 70 | 27.03% |
| Total | 143 | 100.00% | 116 | 100.00% | 259 | 100.00% |

| Diagnosis (cleft) | Male | Percentage | Female | Percentage | Total | Percentage |
|---|---|---|---|---|---|---|
| Pre-foramen | 49 | 34.27% | 41 | 35.34% | 90 | 34.75% |
| Trans-foramen | 94 | 65.73% | 75 | 64.66% | 169 | 65.25% |
| Total | 143 | 100.00% | 116 | 100.00% | 259 | 100.00% |

Statistical tests were performed to analyze whether the clefts (pre- and trans-foramen) were related to sex among patients treated in this service. Tests were also performed to identify if the cleft laterality (uni- or bilateral) had a predilection to either sex. According to the Chi-squared test (Table 4), in the population studied, both the diagnosis of laterality and the clefts themselves are independent of patient sex.
| Test | Sex | N (%) | Chi-square test | Ratio (F/M) |
|---|---|---|---|---|
| Laterality | Female | 116 (44.8%) | x2 = 1.301 | 1 : 1.23 |
| Male | 143 (55.2%) | p = 0.52 | ||
| Pre-foramen x trans-foramen | Female | 116 (44.8%) | x2 = 0.03 | 1 : 1.23 |
| Male | 143 (55.2%) | p = 0.85 |

Kinship
The heredity of the clefts by sex from 2015 to 2017 was subjectively analyzed. Most of the patients had no relatives with this diagnosis. Among males, 77.78% had no relatives with oral cleft, whereas in females, 83.05% had no affected relatives.
Associated Malformations
When analyzing the presence of malformations associated with oral cleft of patients by sex, one can observe that 90.46% of the cleft patients do not have this diagnosis. In males, only 9.36% of the patients presented with this diagnosis compared to 9.74% of females.
Among the 9.56% syndromic cleft patients, 5 had cardiac malformations; 1 had thoracic malformation; 1 had cranial malformation; 2 had intellectual disability; and 6 had two or more associated malformations, the most prevalent being cardiac, ocular, limbs, and urinary system.
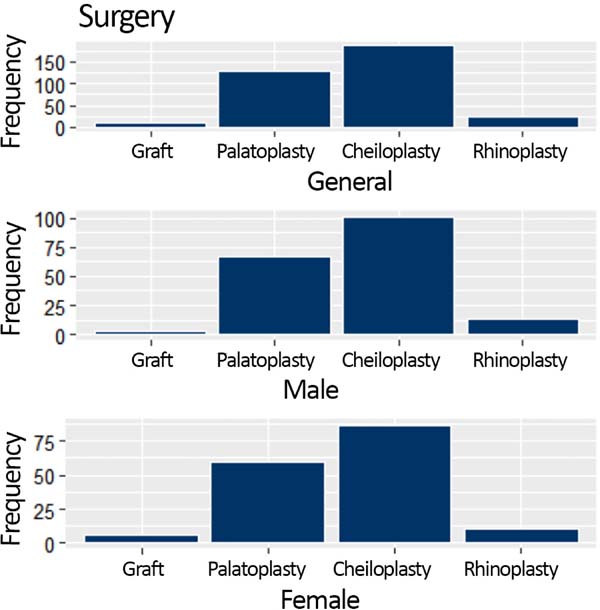
Type of surgery
As shown in Figure 1, at HRAN Cleft Center, the most frequent surgery is cheiloplasty, followed by palatoplasty.

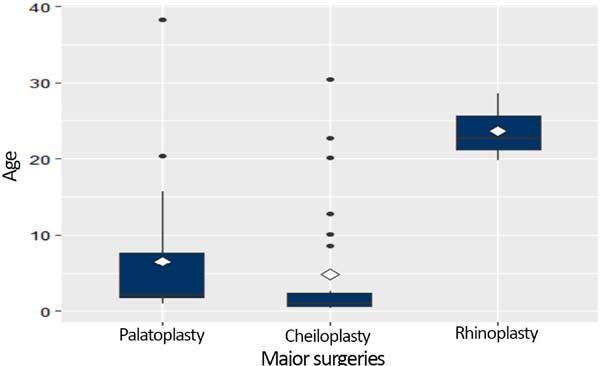
Age
Figure 2 shows the relationship between patient age at surgery, type of surgery performed (palatoplasty, cheiloplasty, or rhinoplasty), and sex. For palatoplasty, the median age for both sexes was 3 years (mean age of females, 9 years; mean age of males, 6 years). For cheiloplasty, the mean age was 4 years for males and 8 years for females. The median age was before the first year of life and 1.42 years, respectively, in males and females. For rhinoplasty, the mean age was 20.54 years (median, 17 years) for males and mean was 19.2 years (median, 22.71 years) for females.

DISCUSSION
A referral center requires the services of several professionals to offer a complete and qualified treatment for cleft patients. However, Paranaíba et al.15 reported that 75% of the treatment units in Brazil have only the following specialists in their services: plastic surgeon, dental surgeon, and speech therapist. At the HRAS, the following professionals are recommended in the interdisciplinary team: plastic surgeon, otorhinolaryngologist, craniofacial surgeon, dentist, odontopediatrician, orthodontist, nutritionist, speech therapist, psychologist, pediatrician, nurse, social worker, and geneticist.
The exact prevalence of cleft lip and palate in Brazil is not known. Studies performed in other centers reported a prevalence of malformation at 0.49 in Rio Grande do Norte; 0.88 in Porto Alegre, RS; and 1.54 in Bauru, SP, for every 1000 live births3,6,16. As cleft lip and palate became a notifiable disease in the DF in September 2017 (Law 5.958/2017), it was not possible to determine its prevalence in the analyzed period (August 2013 to June 2017) in the literature or by using data from the government. Thus, there is a possibility of underreporting, which would have hindered the determination of its prevalence in the local population.
Regarding sex, published reports indicate an increased frequency of oral clefts in males2,8,9,16-22. Although 169 of the 322 children studied (52.48%) were boys, it was not possible to affirm this in the population studied, as there was no statistical relevance.
Of the total of 322 records of oral clefts of patients of HRAN, there is a greater proportion of labial clefts and trans-foramen clefts (80.4%) when compared to isolated cleft palate (19.6%). This finding is in agreement with the literature, in which there are reports of predominance of cleft lip and palate ranging between 69.1% and 81%, taking pre-foramen clefts and trans-foramen clefts as a joint entity 10,19.
As for the diagnosis by the Spina classification, the most prevalent types of clefts were left trans-foramen (20.50%) and bilateral cleft (18.94%), followed by right trans-foramen clefts (13.04%) and incomplete post-foramen clefts (12. 42%). As the p value was greater than 0.05 (p-value of 0.6098), it is not possible to state the prevalence of any type of cleft in this study. However, the literature reports a predominance of left trans-foramen clefts followed by incomplete post-foramen clefts18. Studies that do not discriminate laterality also reported higher frequencies of trans-foramen clefts (24.89 - 37.1%) and post- foramen clefts (26.9 - 31.7%) 17,20.
Regarding the distribution of cleft type by sex, left trans-foramen clefts were more common in females (22.22%), while bilateral trans-foramen clefts were more common in males (21.30%). However, the p valuefor both sexes was greater than 0.05, so it is not possible to determine the prevalence of cleft type in this sample, although studies in Eslováquia, Rio Grande do Sul (BR), Minas Gerais (BR), and Pernambuco (BR) reported the prevalence of cleft lip with or without involvement of the palate was higher in boys and the incidence of isolated cleft palate was higher in females4,7-9,18-22. Regarding laterality, there was a greater prevalence of unilateral left clefts (41.31%), which were 1.3-fold more common than right unilateral clefts (31.66%). Similarly, in the medical literature, left clefts are more commonly described2,8,9,13,16-18,20-22.
Although the etiology is multifactorial, inheritability is reported in the scientific community as the most important factor of oral cleft involvement. The risk of a child being born with a cleft is increased by 40-fold when the parents have this malformation2,5. In this study, 19.85% of patients had a family history of oral clefts, a value close to that observed in the literature (23%)5.
According to the literature, trans-foramen clefts are the most prevalent and there is a higher incidence in males (1.5:1.0)23. In line with the literature, in the present study, trans-foramen clefts were also the most common (65.25%). However, there was no statistically significant influence of sex in the diagnosis of trans-foramen cleft in the sample studied.
In Brazil, few studies have analyzed the frequency and type of congenital malformations associated with patients with cleft lip and palate5. A study conducted in 2014 in the state of Paraíba and one in 2005 in São Paulo reported that 7% and 9.18% of the clefts were syndromic, respectively5,24. Of the patients treated at the HRAN, only 9.54% have associated malformations. This underscores the importance of patients with cleft lip and palate being examined in detail to detect other associated malformations5.
According to the literature, malformations of the lower and upper limbs are the most common (33%), followed by malformations of the cardiovascular system (24%)7. Among the cleft patients treated at the HRAN, cardiac malformations were the most prevalent (25.8%).
The treatment of oral clefts is surgical and each reference center has its own treatment protocol. In accordance with the protocol established by the Cleft Service of the HRAN, cheiloplasty is the first procedure performed in patients with cleft lip and palate; just the lip is corrected in infants under 3 months of life once they reach the minimum organic condition required to undergo general anesthesia7,14.
The fact that 80% of the patients treated at the HRAN had pre-foramen and trans-foramen clefts explains why cheiloplasty is the most common surgical procedure performed by the service. The results of this study show that the mean age of males is 4 years while that of females is 8 years, while the median is before the first year of life and 1.42 years in males and females. Nevertheless, some patients underwent cheiloplasty belatedly, thus changing the mean. This could occur because the HRAN cleft service treats patients regardless of age at presentation; or difficulty accessing the health service; or after a late diagnosis. Consequently, treatment is not always performed at the age recommended by the protocol. However, it is interesting to note that, as the results reveal, most of the patients treated at this service receive surgical treatment in the first year of life.
According to the HRAN protocol, palatoplasty is performed in patients with cleft lip and palate at the age of at least 18 months and when their weight is appropriate. In this study, 36.08% of patients underwent this surgical procedure. The median age in both sexes was 3 years, while the mean age of females was 9 years and that of males was 6 years. Thus, as with cheiloplasty, this surgery is also performed in older ages in this service, likely for similar reasons.
Rhinoplasty is also part of the treatment protocol in cases of nasal deformity. Thus, it is less common and performed only after correction of the cleft lip and palate or when the patient is at least 16 years old14. At the HRAN, in agreement with the literature, only 6.82% of patients underwent this surgical procedure. The mean age was 20.54 years and the median age was 17 years, in line with published recommendations.
According to Paranaíba et al.15, the techniques of Veau and Van Langenbeck are the most commonly used in palatoplasties in international reports. In cheiloplasties, a review of Brazilian surgical protocols showed a preference for the Millard technique for unilateral cheiloplasty and of the Spina and Millard techniques for bilateral cases. In the cleft department of HRAN, the majority of surgeries are performed using the Fisher or Millard techniques for cheiloplasties and the Van Langenbeck and Sommerlad techniques for palatoplasty.
CONCLUSION
The epidemiological profile of patients with cleft lip and palate treated at the HRAS indicates that the majority of patients are male with non-syndromic diagnoses and no family history of this diagnosis. It was not possible to determine a prevalence between the sexes. Trans-foramen clefts were most common, mainly left sided. The most frequent surgery was cheiloplasty, since pre-foramen and trans-foramen clefts were the most common. However, the exact prevalence of this malformation in the DF could not be found in the period analyzed using the local literature and governmental data.
COLLABORATIONS
|
EVR |
Analysis and/or data interpretation, data curation, formal analysis, writing - original draft preparation. |
|
TOP |
Analysis and/or data interpretation, formal analysis. |
|
GNM |
Formal analysis. |
|
LRR |
Conception and design study. |
|
LGM |
Conception and design study, supervision. |
|
MDS |
Supervision. |
|
DRP |
Final manuscript approval, writing - review & editing. |
REFERENCES
1. Aquino SN, Paranaíba LM, Martelli DR, Swerts MS, Barros LM, Bonan PR, et al. Study of patients with cleft lip and palate with consanguineous parents. Braz J Otorhinolaryngol. 2011;77(1):19-23. PMID: 21340184 DOI: https://doi.org/10.1590/S1808-86942011000100004
2. Gardenal M, Bastos PRHO, Pontes ERJC, Bogo D. Prevalent Diagnosis of Orofacial Fissures in a Reference Service with Resident Cases in the State of Mato Grosso do Sul. Int Arch Otorrinolaringol. 2011;15(2):133-41. DOI: https://doi.org/10.1590/S1809-48722011000200003
3. Cunha ECM, Fontana R, Fontana T, Silva WR, Moreira QVP, Garcias GL, et al. Anthropometry and risk factors in newborns with facial clefts. Rev Bras Epidemiol. 2004;7(4):417-22.
4. Dixon MJ, Marazita ML, Beaty TH, Murray JC. Cleft lip and palate: synthesizing genetic and environmental influences. Nat Rev Genet. 2011;12(3):167-78.
5. Baptista EVP. Malformações congênitas associadas à fissura labial e/ou palatal em pacientes atendidos em um serviço de referência para tratamento de defeitos da face: um estudo de série de casos [dissertação]. Recife: Instituto Materno Infantil Professor Fernando Figueira; 2007.
6. Bruner G, Montagnana M, Correa AC, Degan VV, Tubel CAM. Prevalence of lip and palate cleft in Rio Claro - SP, from 2006 to 2009. Odontol Clín Cient. 2012;11(2):117-9.
7. Watson ACH, Sell DA, Grunwell P. Tratamento de Fissura Labial e Fenda Palatina. São Paulo: Santos; 2005.
8. Pacáková D, Zábavníková M, Miklošová M, Kúkel'ová D, Dankovčík R. Epidemiological Study of Orofacial Clefts among Population of Eastern Slovakia during the Period 1996-2013. Cent Eur J Public Health. 2016;24(2):128-32.
9. Martelli DR, Coletta RD, Oliveira EA, Oliveira MC, Swerts MS, Rodrigues LA, et al. Association between maternal smoking, gender, and cleft lip and palate. Braz J Otorhinolaryngol. 2015;81(5):514-9.
10. Loffredo LCM, Freitas JAS, Grigolli AAG. Prevalence of oral clefts from 1975 to 1994, Brazil. Rev Saúde Pública. 2001;35(6):571-5.
11. Dolovich LR, Addis A, Vaillancourt JM, Power JD, Koren G, Einarson TR. Benzodiazepine use in pregnancy and major malformations or oral cleft: meta-analysis of cohort and case-control studies. BMJ. 1998;317(7162):839-43. PMID: 9748174
12. Vaccari-Mazzetti MP, Kobata CT, Brock RS. Antenatal ultrasonography diagnosis of cleft lip and palate. Arq Catarin Med. 2009;38(Suppl 1):130-2.
13. Bunduki V, Ruano R, Sapienza AD, Hanaoka BY, Zugaib M. Prenatal Diagnosis of Lip and Palate Cleft: Experience of 40 Cases. Rev Bras Ginecol Obstet. 2001;23(9):561-6.
14. Trindade IEK, Silva Filho OM. Fissuras labiopalatinas: uma abordagem interdisciplinar. São Paulo: Santos; 2007.
15. Paranaíba LMR, Almeida H, Barros LM, Martelli DRB, Orsi Júnior JD, Marteli Júnior H. Técnicas cirúrgicas correntes para fissuras lábio-palatinas, em Minas Gerais, Brasil. Braz J Otorhinolaryngol. 2009;75(6):839-43.
16. Figueirêdo CJR, Vasconcelos WKS, Maciel SSSV, Maciel WV, Gondim LAM, Tassitano RM. Prevalência de fissuras orais no Estado do Rio Grande do Norte, Brasil, entre 2000 e 2005. Rev Paul Pediatr. 2011;29(1):29-34.
17. Freitas JAS, Dalben GS, Santamaria Júnior M, Freitas PZ. Current data on the characterization of oral clefts in Brazil. Braz Oral Res. 2004;8(2):128-33.
18. Vasconcelos BCE, Oliveira e Silva ED, Porto GG, Pimentel FC, Melo PHNB. The incidence of the lip and palate malformations. Rev Cir Traumat Buco-Maxilo-Fac. 2002;2(2):41-6.
19. Paranaíba LMR, Miranda RT, Ribeiro LA, Barros LM, Martelli-Júnior H. Frequency of congenital craniofacial malformations in a Brazilian Reference Center. Rev Bras Epidemiol. 2011;14(1):151-60.
20. Di Ninno CQMS, Fonseca LFN, Pimenta MVE, Vieira ZG, Fonseca JA, Miranda ICC, et al. Epidemiological survey of patients with cleft lip and/or palate at a specialized center in Belo Horizonte, Brazil. Rev CEFAC. 2011;13(6):1002-8.
21. Coutinho ALF, Lima MC, Kitamura MAP, Ferreira Neto J, Pereira RM. Epidemiological characteristics of patients with orofacial clefts attending a Referral Center in Northeast Brazil. Rev Bras Saúde Matern Infant. 2009;9(2):149-56.
22. Gundlach KK, Maus C. Epidemiological studies on the frequency of clefts in Europe and world-wide. J Craniomaxillofac Surg. 2006;34 Suppl 2:1-2.
23. Kuhn VD, Miranda C, Dalpian DM, Moraes CMB, Backes DS, Martins JS, et al. Fissuras labiopalatais: revisão da literatura. Disciplinarum Sci. 2012;13(2):237-45.
24. Sousa ALB. Incidência e caracterização de fendas orofaciais em nascidos vivos registrados em dados do SINASC (DATASUS) - Paraíba - de 2002 a 2010 [Trabalho de Conclusão de Curso]. João Pessoa: Universidade Estadual da Paraíba; 2014.
1. Hospital Regional da Asa Norte, Brasília, DF,
Brazil.
Corresponding author: Tayane Oliveira Pires SMHS - Área Especial, Q. 101, Asa Sul - Brasília, DF, Brazil Zip Code 70330-150 E-mail: tayaneoliveirap@gmail.com
Article received: December 18, 2018.
Article accepted: February 10, 2019.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket