



Articles - Year 1998 - Volume 13 -
Evaluation of Lips Growth Repaired by the Double Breasted Approach of the Orbicularis Oris Muscle
Avaliação do Crescimento do Lábio Reparado pela Sutura Entrecruzada do Músculo Orbicular
ABSTRACT
The authors evaluated the lip growth of l0 newborn babies bearing complete unilateral incisive pre, trans and post-foramen cleft. The double breasted approach, attained in each side of the cleft, promoted the realignment of the muscle fibers at the cleft level and restored the morphology of the lip, promoting the functional and anatomical repair of the fissured lip. The muscle fibers realignment restored the lip muscular girdle, recovering the muscular tonus and activity. This kind of functional and anatomical repair has enabled an equilibrated growth of the repaired lip. The lip growth evaluation has been performed comparing its length and height, in each side of the cleft, before the repair and during the first five years after the cleft correction.
Keywords: crossed suture; orbicularis oris muscle; transverse measurement; vertical measurement; lip growth.
RESUMO
Os autores avaliaram o crescimento do lábio em 10 récem-nascidos, portadores de fissura pré, trans e pós-forame incisivo unilateral completa. A sutura entrecruzada dos retalhos do músculo orbicular do lábio, obtidos em cada lado da fissura, promoveu o realinhamento das fibras musculares ao nível da fissura e restaurou a morfologia do lábio, proporcionando uma reparação anatômica e funcional para o lábio fissurado. O realinhamento das fibras musculares restaurou a cinta muscular do lábio, recuperando a atividade e o tônus muscular. Este tipo de reparação anatômica e funcional permitiu o crescimento equilibrado do lábio reparado. A avaliação do crescimento do lábio foi realizada comparando o comprimento e a altura do mesmo, em cada lado da fissura, antes da reparação e durante os cinco primeiros anos após a correção da fissura.
Palavras-chave: sutura entrecruzada; músculo orbicular do lábio; medida transversal; medida vertical; crescimento do lábio
With the purpose of reaching a better anatomical correction for fissured lips, many proposals have been written, firstly directed to the tracing of incisions(1,8). However, the functional and aesthetic changes of repaired lips were frequent, being related to incorrect repair of the orbicularis oris muscle(10). The muscle anatomical deformity has deserved more attention since the Fara(5) reports. Precise concepts about the anatomical changes of the orbicularis oris muscle have been acquired by means of histological studies, attained by means of longitudinal cuts of the fissured lip. Tridimensional histological studies of lips on unilateral clefts showed muscle fibers disarrangements close to the cleft margins, as well as numerous dermal insertions of the muscle close to them(7). With a better knowledge of the orbicularis oris muscle anatomical alterations in unilateral clefts, many proposals have been presented for its correction, with the purpose of recovering me lip functionally and aesthetically(2,9). The growth of the repaired lip has been evaluated comparing its length and height in each side of the cleft(6).
The presented study is intended to evaluate me growth of the repaired lip by means of a crossed suture of the orbicularis oris muscle(2), and in unilateral lips clefts, comparing its transverse and vertical measures in each of the cleft sides.
MATERIAL & METHODS
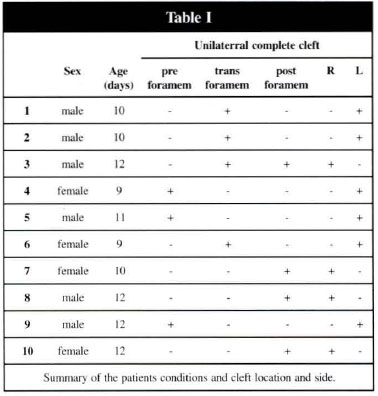
Patients carrying complete unilateral incisive pre, trans and post-foramen cleft underwent a lip correction by the double breasted approach. Ten newborns were evaluated, 4 females and 6 males, submitted to lips repair 9 to 12 days after birth, according to weight recover presented upon birth. Table I generally demonstrates me patients who have been evaluated.
The lips repair has been carried out by means of a transfixing incision reaching all the skin and muscle thickness up to the mucous membrane, all along the margin of me cleft, in each of the fissured slopes, widely exposing me orbicularis oris muscle. The muscular repair started by the orbicular muscle dissection, both of skin as of the mucous membrane, along all vertical extension of the lip originating, in me middle cleft slope, a fibrous-muscle flap with length of 0.5 em and width corresponding to the height of the lip (fig. l). The flap formed in the side fissured slope was constintted only by muscular tissue, with measures identical to the median fissured slop flap (fig. 1). The muscle fibers of the orbicularis oris muscle were horizontally realigned in the cleft spot through rotation and advancement of muscular flaps, in each fissured slope. The muscular repair continued with the crossed suture of muscular flaps, with the fibrous-muscle flap sutured wlder the muscular flap, and being fixed 0,25 cm inside its distal extremity. The muscular repair has been finished by fixing the muscular flap over the fibrous-muscle flap (fig. 2b). The skin suture has been defined by a broken line together with the nasal floor, followed by a straight line all along the lips height (fig. 3).
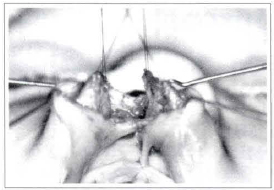
Fig. 1 - Muscular flaps formed after complete liberation of skin and mucous membrane, in the fissured side and in the non-fissured side.

Fig. 2a - Fibrous-muscle flap of the non-fissured side sutured under the muscular flap of the fissured side.
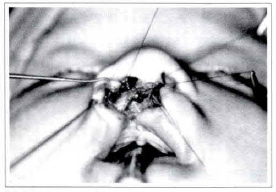
Fig. 2b - Muscular repair concluded with the muscular flap fixation of the fissured side over the flap of the non-fissured side. The arrow shows the fibrous-muscular flap under the muscular flap.
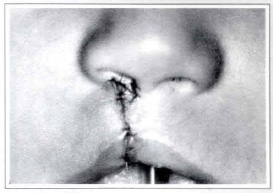
Fig. 3a - Skin suture showing the broken line with the nose floor, followed by the straight line all along the reconstructed filter crests (frontal view).
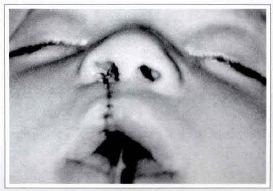
Fig. 3b - Skin suture showing the broken line with the nose floor, followed by the straight line all along the reconstructed filter crests (mentonasal view).
The length and height of the lip were considered as parameters to evaluate the repaired unilateral fissured lip growth. The length of the lip has been determined by the distance, measured in millimeters between the oral commisure of the non-fissured side and the oral comissure of the fissured side, all along the mucous-cutaneous line. The height of the lip has been taken by means of two measures, the first one corresponding to the distance between the cupid bowl extremity and the implant of the nasal wing of the lip. The second measure has been determined by the distance between the cupid bowl extremity and the implant of the columella in the lip, for each side of the cleft. All measurements have been taken with a surgical compass and its opening has been transferred to a millimetric ruler (fig. 4).
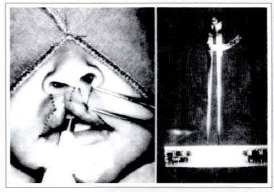
Fig 4 - (A) Measurements of the lip made with surgical compass. (B) Opening made by surgical compass transferred to millimetric rule.
RESULTS
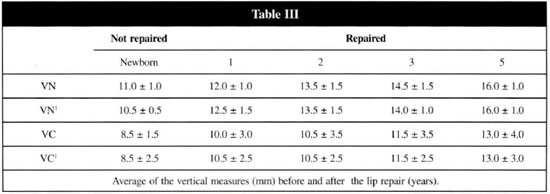
The lip repaired by the double breasted approach recovered the morphology of the lip restoring the filter depression, projecting the filter crest, reconstructing the cupid bowl and aligning the vermillion's margin (fig. 5). The lip growth has been evaluated measuring its length and height in each side of the cleft. The transverse measure has been considered as lip length, identified as "T", corresponding to the distance of the lip comissure up to the cupid bowl in the non-fissured side, and as "T1", the same distance in the fissured side. The cupid bowl length has been represented by "P" (fig. 6). The lip height has been deterolined by its vertical measures, identifying as "VN" the distance between the cupid bowl extremity and the nasal wing of the non-fissured side, and "VN1" the same distance in the fissured side. "VC" represented the distance between the extremity of the cupid bowl and the columella in the non-fissured side, corresponding to "VCl" the same distance in the fissured side (fig. 6).
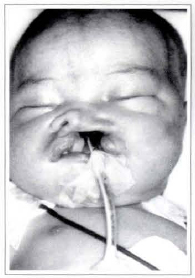
Fig. 5a - Preoperative view.
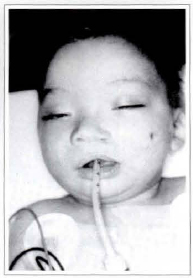
Fig. 5b - Recovering of the lip morphology, 1 year after the intercrossed suture of the flaps of the lip orbicular muscle.

Fig. 6 - The growth of the lip has been evaluated and compared to its length and height, before and after the repair, in both sides of the fissure.
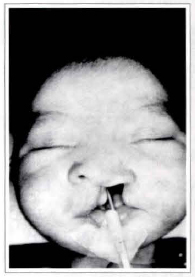
Fig. 7a - Complete unilateral incisive pre, trans and post foramen c1eft with 9 days evolution.
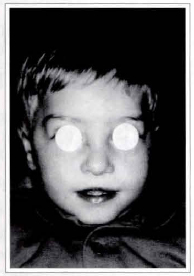
Fig. 7b - Result after 1 year of the lip repair, showing the symmerry of rhe repaired lip.
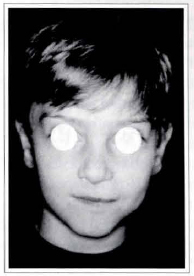
Fig. 7c - The same patient 5 years after repair, keeping the lip symmetry.
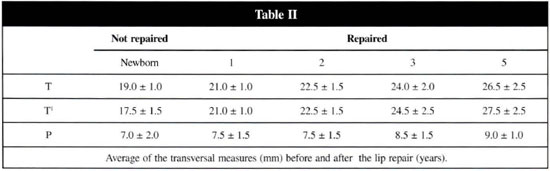
Measurements have been taken on lips of 10 newborns bearing the complete unilateral incisive pre, trans and post-foramen cleft before repair. The same measurements have been taken again after 1 year from the repair and repeated every year during 5 years. Tables II and III demonstrate the measures taken during the patients observation period. The growth of the lip has been evaluated by comparing the measures taken in the fissured side against the measures of the non-fissured side. The growth of the lip did not present significant differences between the female patients and the male ones. Also, the kind and the side of the clen did not interfere in the growth of the lip. In the same way, the growth of the lip did not present significant differences concerning the pre, trans or post-foramen placement of the cleft. Table II shows the transverse measures of the lip during the evaluation period. It has been observed that the growth of the lip in the fissured side was meaningfully greater than the growth of the non-fissured side, during the fist year after repair. In the rest of the evaluation period, the transverse growth of the lip was proportional to both sides of the cleft. Table III presents the lip vertical measures, taken during the evaluation period, both to the height close to the nasal wing and to the height close to the columella. The prolabium represented by the cupid bowl, filter and filter crests/peaks, has also presented a proportional growth during all the evaluation period.
COMMENTS
When Schendel(ll) analyzed the unilateral lip clefts, it was observed that a muscular atrophy non-neurogenical, with muscular fibers disarrangenlents extending over 4 mm beyond the cleft margins. Based on these information, it has been delimitated as 0.5 cm the length for the flaps of the orbicularis oris muscle. The length determined to the flaps, associated to their movement of advancement and rotation, allowed the realignment of the orbicular muscle fibers with the cleft margins, recovering the muscular girdle of the lip. The traction of the restored muscular girdle, added to the redirectioning of the muscle fibers, has estimulated the muscle development, having the natural growth of the lip as a consequence. The transverse growth was more emphasized in the fissured side during the first year after the repair and it has occurred due to the intensified pressure presented by the muscular fibers repaired with the cleft, motivated by the tissue gap at this level. Kaplan(6) also observed that the muscular tissue, when under strong traction in the fissured side, promoted a more intense growth of the lip in this side than in the non-fissured side. When he evaluated the growth of the lip, he described transverse measures equivalent to the ones of the present smdy. The vertical measures presented some meaningless disagreements. The double breasted approach, by means of superposing of muscular flaps, provided an additional volume of tissue at the cleft level, and reconstructed the filter crests, the lip filter, the cupid bowl and the mucous-cutaneous line(3), allowing the harmonical growth of the prolabium. It was concluded that the double breasted approach restored the morphology and the lip muscular girdle, recovered the functional-aesthetic equilibrium, allowing the harmonical growth of the lip.
REFERENCES
1. ABRAMO, AC. Tratamento Cirúrgico para Correlação das Fissuras Labiais Unilaterais. An. Paul. Med. Cir. 1983; 110:25-30.
2. ____. Orbicularis Oris Muscle: A Double-Breasted Suture for its Repair in the Unilateral Cleft Lip. Ann. Plast. Surg. 1991; 27:398-403.
3. ____. The Double-Breasted Suture of Orbicularis Oris Muscle to Treatment of Unilateral Cleft Lip. In: PLASTIC SURGERY V. 2. Excerpta Medica. International Congress. 1992; 185-6.
4. DADO DV, KERNAHANM, DA - Anatomy of the Orbicularis Oris Muscle Based on Histological Examination. Ann. Plast. Surg. 1985; 15:90-8.
5. FARA, M. Anatomy and Arteriography of Cleft Lips in Stillborn Children. Plast. Reconstr. Surg. 1968; 42:29-36.
6. KAPLAN, EN. Growth Unilateral Cleft Lip. Cleft Pal. J. 1978; 15:202-8.
7. KERNAHAN, DA, DADO, DV, BAUER, BS. Anatomy of the Orbicularis Oris Muscle in Unilateral Cleft Lip Based on a Tree Dimensional Histological Reconstruction. Plast. Reconstr. Surg. 1984; 73:875-81.
8. MILLARD, DR Jr. Refinements in Rotation-Advancement Cleft Lip Technique. Plast. Reconstr. Surg. 1964; 33:26-38.
9. NICOLAU, PJ. The Orbicularis Oris Muscle: functional approach to its repair in cleft lip. Br. J. Plast. Surg. 1969; 36:141-53.
10. RANDALL, P, WHITAKER, LA, LA ROSSA, D. Muscle Reconstrucrion in Primary and Secondary Cleft Lip. Plast. Reconstr. Surg. 1974; 54:316-23
11. SCHENDEL, SA; PEARL, RM; DE'ARMOND, SJ. Pathophysiology of Cleft Lip Muscle. Plast. Reconstr. Surg. 1989; 83:777-84.
I - MD in Plastic Surgery by Escola Paulista de Medicina, Universidade Federal de São Paulo - UNIFESP, Medical Chief of A.C.A. - Grupo Integrado de Assistência em Cirurgia Plástica.
II - Residellt Doctor of A.C.A. - Grupo Integrado de Assistência em Cirurgia Plástica.
Work performed at A.C.A. - Grupo Integrado de Assistência em Cirurgia Plástica, residency service for training in plastic surgery of Hospital Beneficência Portuguesa de São Paulo, Brazil.
Address for Correspondence:
Antonio Carlo Abramo, MD
Rua Afonso de Freitas, 641
04006-052 - São Paulo - SP
Brazil
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket