



Case Reports - Year 2000 - Volume 15 -
Pectoralis Major Myocutaneous Flap Associated with Tongue Flap on Cheek Reconstruction - An Alternative to the Microsurgery Flaps - Case Report
Retalho Musculocutâneo de Peitoral Maior Associado ao Retalho de Língua na Reconstrução da Bochecha - Uma Alternativa aos Retalhos Microcirúrgicos - Relato de Caso
ABSTRACT
Patients with face and oral cavity deformities due to tumor excisions may benefit from the association of pectoralis major myocutaneous flap with other flaps, including microsurgical free flaps. We report a case of squamous cell carcinoma on the right jugal reqion; the carcinoma ulcerated on the cheek skin, lips and lipjunction. After the surgery the area was reconstructed using a pectoralis major myocutaneous flap associated with a tongue flap. There were no complications and a postoperative radiotherapy was performed between December 14, 1997 and January 09, 1998. On March 20, 1998 the patient was asymptomatic and a follow-up, as an out patient, was suggested. The purpose of this report is to present an alternative option, using a pectoralis major myocutaneous flap associated with a tongue flap for total thiekness cheel: deformity reconstruction. The head and neck surgery and the plastic surgery reconstructive techniques developed concomitantly. The c ombination of the flaps mentioned herein ispart of this evolution. It is a simple technique with few complications and good functional and esthetic results.
Keywords: Surgical flaps; chest muscles - surgery; mouth - surgery; tongue; cheeks
RESUMO
Em pacientes com deformidades de face associadas a deformidades de cavidade oral decorrentes de ressecções tumorais, o retalho musculocutâneo de peitoral maior pode ser usado associado a outros tipos de retalhos, inclusive transplantes livres microcirúrgicos.
O caso apresentado é de um paciente portador de carcinoma espinocelular em região jugal direita, ulcerado na pele da bochecha, lábios e comissura labial, que, após ressecção cirúrgica, teve essa área reconstruída com o retalho musculocutâneo de peitoral maior (RMCPM) associado ao retalho de língua.
O paciente evoluiu bem, e foi realizada radioterapia pós-operatória no período de 14/12/97 a 9/01/98. Em vinte de março daquele ano apresentava-se assintomático, tendo sido orientado controle mensal para 1998.
O objetivo é apresentar uma opção alternativa, utilizando o RMCPM associado ao retalho de língua para reconstrução de deformidade de bochecha de espessura total.
A evolução histórica da cirurgia de cabeça e pescoço corre paralela ao desenvolvimento das técnicas de reconstrução da cirurgia plástica. Neste contexto insere-se a utilização combinada dos retalhos aqui citados, técnica simples de ser realizada, com baixo índice de complicações, além de apresentar bons resultados estéticos e funcionais.
Palavras-chave: Retalhos cirúrgicos; músculos peitorais - cirurgia; boca - cirurgia; língua; bochecha
For the last 35 years, head and neck surgery reconstructive techniques have improved substantially. Among the wide range of cantributions, the pectoralis major myocutaneolls flap(1,2) (PMMF) can be considered a very important one. lt is technically easy to perform, presents low morbidity and mortality, and is very versatile. The functional and esthetic final results are highly satisfactory. PMMF's versatility includes the possibility of cambination with other flaps, including free flaps(3,4). It should be noted that microsurgical free flaps and microsurgery sutures brought about new options and good results to wide reconstruction in head and neck surgery(5). However, the microsurgical free flapstechniques present a higher morbidity compared to PMMF. They also require a specialized plastic surgeon, a well-equipped hospital capable of providing appropriate support, and other specialized professionals.
Total thickness cheek resections comprehend the skin, the soft tissues, and the oral mucosa, and create a great deformity. Thus, several reconstruction options must be considered. An alternative option, using a PMMF(1,2) associated with a tongue flap, is presented here(6,7).
CASE REPORT
A 35 years old patient, male, Caucasian, Brazilian, from São Paulo, was assisted by the Neck and Head Surgery Division. He referred to have a protuberance at the right jugal region for approximately 4 months. He smoked less than 20 cigarettes a day for many years, but denied alcoholism.
The local examination revealed a right jugal ulcer infiltrating the oral mucosa, of 6 x 5 cm in its largest diameters, compromising the soft tissues and the facial skin. A biopsy of the ulcerated lesion on the cheek skin was performed, and a squamous cell carcinoma diagnosis was confirmed. The patient presented a high cervical lymph node on the right side with 0.8 cm diameter, fibroelastic, mobile, not adhering to deep layers. There was also a one-cm-diameter submandibular lymph node on the left, fibroelastic, mobile, and non adherent. The International Union Against Cancer (UICC) TNM classification was: T4N2bM0, clinical stage IV (Figs. 1 and 2).
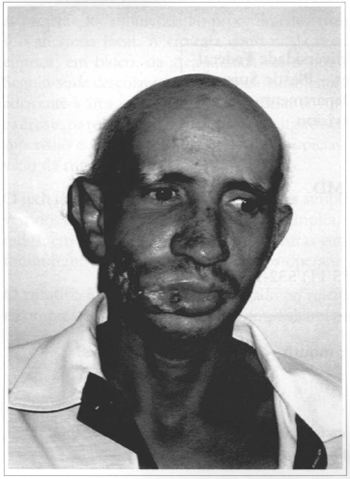
Fig. 1 - Ulcerated tumor on the cheek skin, upper lip, lower lip and right labial junction.
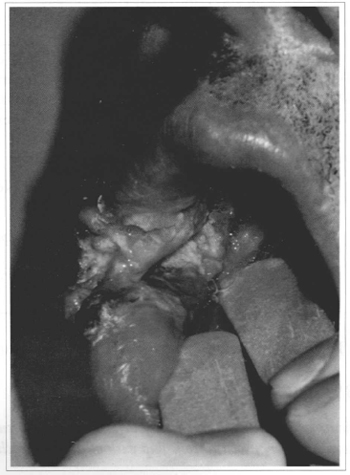
Fig. 2 - Ulcerared tumor on the mucosa - jugal region.
The surgery was performed on April 29, 1997. It consisted sisted of a large excision that removed the total cheek thickness on the right, the lip junction, part of the upper and lower lips, and the mouth floor. In addition, a superficial parotidectomy was performed, preserving the facial nerve temporal branch; an extended cervical lymphadenectomy on the right, preserving the spinal nerve, and a left supraomohyoid extended lymph node resection were also performed.
The reconstructive technique was a combination of a right PMMF and a right hemitongue flap . The PMMF was made according to the standardized technique(4,5).
The muscle and mucous membrane for me inner cheek was made from a full thickness ipsilateral hemitongue flap with posterior pedicle. A longitudinal incision was performed on me hemitongue midline and me tongue was opened "as a book page". The flap was laterally ratated and sutured to form me internal aspect of the cheek (Figs. 3 and 4). The homolateral hypoglossus nerve was identified at me common carotid artery level, and was cut and tied to avoid flap movement and suture tensioning. The left hemitongue was sutured marginally, creating "a new tongue". The PMMF was transferred and sutured over me tongue flap to reconstruct me facial outline. A nasoenteric feeding tube was placed for nutritional support, and a tracheostomy was performed to assure breathing. The drainage was carried out by continuous suction of me neck and thorax.
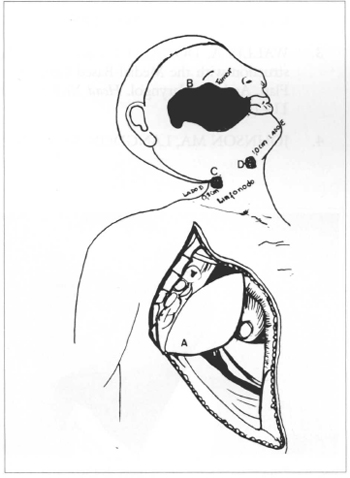
Fig. 3 - A: Larger Pectoral Musculocutaneous flap. B: Tumor. C: Ipsilateral lymph node. D: Controlateral
lymph node.
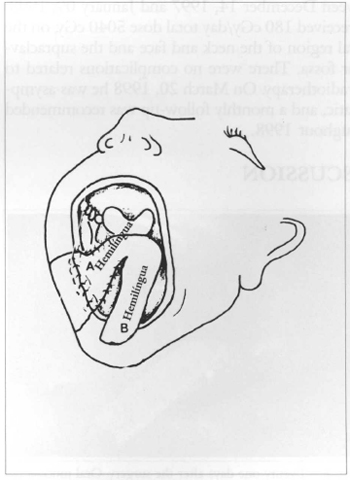
Fig. 4 - A: Ipsilateral hemitongue. B: Controlateral hemitongue.
The patient recovered well fram me surgery and had no complications. He was discharged on May 10, 1997. The nasoenteric feeding tube and me tracheal cannula were removed on May 23, 1997. When me patient was referred to me Radiotherapy Service, he presented good phonation and swallowing (Figs. 5 and 6). The postoperative radiotherapy was made between December 14, 1997 and January 09, 1998.
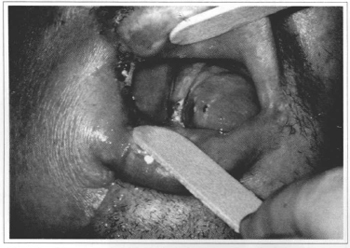
Fig. 5 - Twenty-one days after the surgery. Oral mucosa reconstructed by the rongue flap.
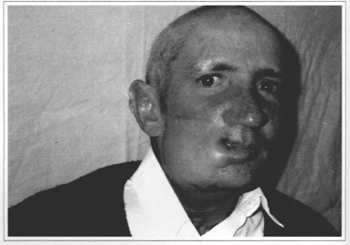
Fig. 6 - Ninety days after the surgery. Esthetic result of the pecroralis major myocutaneous flap on the cheek.
He received 180 cGy/day total dose 5040 cGy, on the lateral region of me neck and face and the supradavicular fossa. There were no complications related to me radiotherapy On March 20, 1998 he was asymptomatic, and a monthly follow-up was recommended throughout 1998.
DISCUSSION
The head and neck surgery and reconstructive technigues developed concomitantly(1,8) The first usually results in significant deformities and the latter has allowed me head and neck surgeons to make progressively larger surgeries with low mortality and morbidity, and good functional and esthetic results.
CONCLUSION
The combination of flaps mentioned herein is a simple technigue, and represents an alternative and a contribution to me current technigues supported by the literarure(1,8).
REFERENCES
1. ARIYAN S. The pectoralis major myocutaneous flap for reconstruction in the head and neck. Plast. Reconstr. Surg. 1979;63:73-81.
2. MEHTA S, SARKAR S, KAVARANA N, BHATHENA H, MEHTA A. Complications of the Pectoralis Major Myocutaneous Flap in the Oral Cavity: A Prospective Evaluation of 220 Cases. Plastic. Reconstr. Surg. 1996;98(1):31-37.
3. WALLIS A, DONALD P. Lateral Face Reconstruction with the Medial-Based Cervicopectoral Flap. Arch. Otolaryngol. Head Neck Surg. 1988;114(7):729-733.
4. JOHNSON MA, LANGDON JD. Is skin necessary for intraoral reconstruction with myocutaneous flaps? Br. J. Oral Maxillofac. Surg. 1990;28(5):299-301.
5. JACOBSON Mc, FRASSEN E, FLIS DM, BIRT BD, GILBERT BW. Free Forearm Flap in Oral Reconstruction. Functional Outcome. Arch. Otolaryngol. Head and Neck Surg. 1995;121(9):959-964.
6. DIAZ FJ, DEAN A, ALAMILLOS FJ, NAVAL L, FERNÁNDEZ J, MONJE F. Tongue Flaps for Reconstruction of the Oral Cavity. Head Neck. 1994;16:550-554.
7. ROBBEN C, SCHOENAERS J, BOSSUYT M. The use of tongue flaps for oral tissue repair. Acta Stomatol. Belg. 1995;92(4):171-184.
8. IOANNIDES C, FOSSION E. Nasolabial flap for the reconstruction of defects of the floor of the mouth. Int. J. Oral Maxillofac. Surg. 1991;20(1):40-43.
I. Mestre em Cirurgia Plástica Reparadora pela UNIFESP-EPM, Cirurgião Plástico do Hospital Infantil Menino Jesus, São Paulo.
II. Doutor em Medicina pela UNIFESP-EPM.
III. Mestre em Cirurgia Plástica Reparadora pela UNIFESP-EPM.
IV. Profª. Titular da Disciplina de Cirurgia Plástica do Depto. de Cirurgia da UNIFESP-EPM.
V. Prof. Dr. da Disciplina de Otorrinolaringologia da UNIFESP-EPM.
Endereço para correspondência:
R. Manoel da Nóbrega, 277
São Paulo - SP - 04614-000
Fone: (11) 543-9451 - Fax: (11) 532-1677
e-mail: gaibu@uol.com.br
Escola Paulista de Medicina da Universidade Federal de São Paulo - Depto de Cirurgia - Disciplina de Cirurgia Plástica e Depto de Otorrinolaringologia - Setor de Cirurgia de Cabeça e Pescoço
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket