



Articles - Year 2002 - Volume 17 -
Laserlipolysis: Liposuction Using Nd-YAG Laser
Laserlipólise: Lipoaspiração com Nd-YAG Laser
ABSTRACT
The authors report their experience with laserlipolysis, a surgical procedure that uses a Nd-YAG type laser with a 1064nm wavelength to treat localized adiposity, as an isolated or associated method to other traditional procedures. The physical principles of laser action on the adipocyte, anesthetic details, application technique, cases, advantaqes, limitations, disadvantages, complications and long-term results are analyzed. Moreover, the principle of action of laserlipolysis - photo-hyperthermia - on fat and adjacent tissue is demonstrated and analyzed by histological studies.
Keywords: Laserlipolysis; laser liposuction; Nd-Yag laser; peristaltic pump; photo-hyperthermia
RESUMO
Os autores relatam sua experiência com a laserlipólise, procedimento cirúrgico que utiliza um laser do tipo Nd-YAG com comprimento de onda de 1064nm no tratamento da adiposidade localizada, seja como método isolado ou associado a outros procedimentos tradicionais. São analisados os princípios físicos de ação do laser sobre o adipócito, detalhes anestésicos, a técnica de aplicação, casuística, vantagens, limitações, desvantagens, complicações e resultados a longo prazo. Além disso, é demonstrado e analisado, através de estudos histológicos, o princípio de ação da laserlipólise - foto-hipertermia - sobre a célula gordurosa e tecidos adjacentes.
Palavras-chave: Laserlipólise; lipoaspiração a laser; Nd-Yag laser; bomba peristáltica; foto-hipertermia
Liposuction and its variants are currently among the most frequent surgical procedures in cosmetic surgery. The techniques for removing and remodeling body fat have evolved since the advent of liposuction(1). The main resources developed were syringe aspiration, dry and humid liposuction, using a tumescent solution, internal ultra-sound, external ultra-sound, superficial liposuction, associating the technique that uses compressed air or electrical motors, as in vibroliposuction, and infusion and suction pumps. Despire the evident progress, the major concern in relation to liposuction is still the total volume suctioned and its clinical and hemodynamic effects, as well as the quality of postoperative recovery.
Blood loss has been partially controlled with the advent of tumescence infiltration anesthesia. Larger amounts of fat can be removed more safely, regardless of the anesthetic modality used, by injecting a large amount of liquid into fat, using a solution consisting mainly of saline, adrenaline, bicarbonate and lidocaine. Despite ultra-sonic liposuction being a safe method and having some advantages in relation to the traditional fat suction technique, it is not universally accepted not is it free of undesirable effects.
Laser as an adjuvant to liposuction was described for the first time by Apfelberg in 1994(2), who showed results of a multi-center study approved by the FDA in five different centers for cosmetic surgery. In the study, the liposuction cannula had an optic fiber inside responsible for conducting and emitting a 40W laser (Nd-YAG laser) ray. The laser would only work on fat that had already been suctioned through the cannula orifice, coagulating blood vessels. In 1996, the same author(3) updated and broadened the study and despite not completely conclusive results, smalier blood loss, shorter recovery period, less edema, pain, ecchymosis and discomfort in the post-treatment period were evident. The study was interrupted however. In 1997 and 1999, Cook(4,5) described his experience with subcutaneous tissue vaporization on the face using laser. Blugerman(6), in 2000, and Schavelzon(7), in 2001, showed results obtained by using only laserlipolysis. Neira(8,9,10,11), in 2001, reported his experience with the external laser on fat and the hemodynamic variables and levels of lidocaine associated with the procedure. In the same year, Solarte(12) described the low power effects of laser on fat.
In the present study we present our experience using Nd-YAG laser to treat lipodystrophies, a procedure calied laserlipolysis.
MATERIAL AND METHODS
In laserlipolysis, we use Nd-YAG type laser equipment with a 1064 nm wavelength associated with a Helium- Neon laser. The laser ray is conducted to the fat by a 300 micra optic fiber with a stainless steel 1 mm diameter and variable length microcannula. The optic fiber runs 2 or 3 mm beyond the distal extremity of the cannula and the laser action is limited to this site (Fig. 1). After the team and patient are protected adequately with special eyeglasses, small 1 mm incisions are made in the desired sites, through which a microcannula is introduced advancing back and forth in fan-like movements, at different levels of depth, including the subcutaneous, similar to superficial liposuction. These movements are helped by the action ofthe laser. The low power laser (maximum 6W) produces a photo-hyperthermia effect when in contact with fat, transforming luminous energy into heat in adipocytes. The reddish tone ofthe ray (He-Neon) on the skin can be perceived due to transillumination. The time of action of the laser depends on the amount of existing fat, tissue resistance and the extension of the treated area, in addition to trans-operative palpation. The passage of the laser creates small tunnels of fat and the delicate protein membrane of fat cells burst due to photothermia, liberating the oily content they contain (Figs. 2 and 3). The oily solution that remains dispersed in the treated areas is generally drained. For this purpose, a 2 mm multi-perforated cannula, attached to the same peristaltic pump is used for infusing the tumescent solution, specially developed for this purpose. By means of negative pressure, not above 450 or 500 mmHg, the product of laserlipolysis is removed from the treated areas. The routine that follows is similar to traditional liposuction, with slightly compressive dressings, analgesics and general care. Practically all are outpatient procedures and after the second post-operative day one may return to activities. Manual lymphatic drainage starts on the first week after surgery.
In a period of 30 months, 1,734 surgeries were performed in three centers for cosmetic surgery. Of the total, 82% (1,421 patients) were women and 18% (312) men. Age varied between 15 and 78 years. Practically all procedures were performed with local tumescent anesthesia using a peristaltic infusion pump and a solution containing 1 mg of adrenaline, 15 ml of molar Sodium Bicarbonate and 15 ml of 1% Lidocaine for each liter of warm saline. The concentration and volume of lidocaine, as well as the amount of injected solution, varied according to the amount of fat to be treated and its localization. There was a 20 to 30 minute waiting period before beginning the process. The technique was indicated for treating localized lipodystrophy and irregular fat in healthy patients, preferably non-smokers and near their ideal weight. The maximum aspirated volume did not exceed 5% of the body weight.
RESULTS
Results obtained with laserlipolysis are similar to those obtained with traditional liposuction methods. Of the 1,734 patients treated, one suffered a small 1 cm diameter burn that healed without sequela; there were 37 cases of asymmetry; one seroma and a small infection in the site where the microcannula penetrated.
DISCUSSION
The major limitation of traditional lipoplasty methods seems to be the amount of fat removed due to the associated hematic loss. Although observations are preliminary and more studies and follow-up are needed, laserlipolysis with a 1064nm Nd-YAG laser, associated with tumescent infiltration using a peristaltic infusion pump, proved to be a method with low hematic loss, a low rate of ecchymosis and little discomfort in the post-operative period. The treatment of areas that traditionally pose greater difficulty in removing fat, such as the dorsal regions or breasts, in gynecomastia, is made easier, as the microcannula with the laser has a diameter of only 1 mm, and penetration is made easier by action of the ray. This also causes less effort and fatigue for the surgeon. This facilitating effect is also observed in previously operated areas. The observation of a reddish color from the Helium-Neon source, due to transillumination, makes the procedure quite accurate, as it allows the surgeon to identify the exact place where the tip of the microcannula is and where the laser is working. Histological studies have shown positive effects as in the coagulation of small vessels in fat (Fig. 4), rupture of adipocytes (Figs. 2 and 3), reorganization of reticular derme (Fig. 5) and coagulation of fat collagen (Fig.6). The effect of vessel coagulation would corroborate to a small blood loss and less ecchymosis. Collagen coagulation and reorganization of the derme, effects already observed with other types of laser, would contribute to adequate tissue retraction.
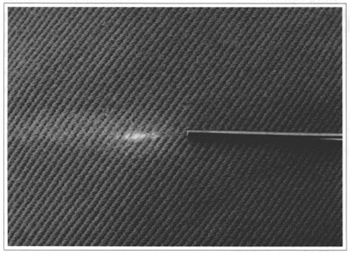
Fig. 1 - Exposed optic fiber emitting laser to the tip of the 1 mm diameter cannula.
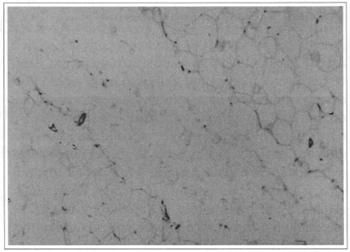
Fig. 2 - Tunnel produced in fat by the Nd-YAG laser, showing the ruptured cell structure.
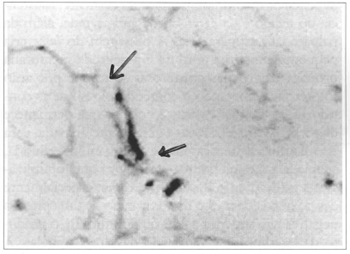
Fig. 3 - Proximal view of the cell membrane rupture.
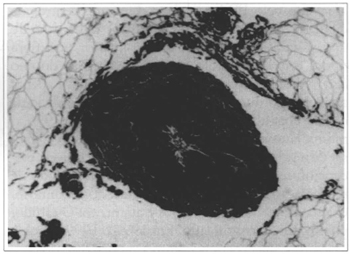
Fig. 4 - Histological detail showing the coagulation of a small vessel in fat due to laser action (Orceine 32x).
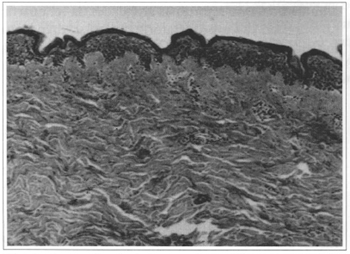
Fig.5 - Reorganization of the reticular derme (HE 32x).
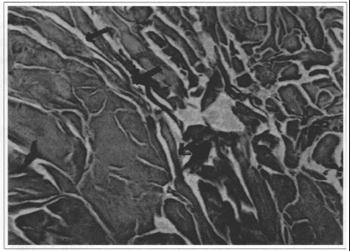
Fig. 6 - Collagen coagulation (HE 100x).
It is difficult to measure the amount of fat removed because laserlipolysis is different from usual lipoplasty methods since it does not simply remove fat whenever it is used as an isolated method. Tumescence infiltration, however, makes accurate measuring difficult. The amount of tumescent solution infiltrated varied from 270 ml to 3.3 liters.
Hemoglobin, hematocrit, triglycerides and cholesterol dosing were performed in 20 patients in the pre-operative period, one day; one week and one month after the procedure (when performed alone) and did not present any significant change.
CONCLUSION
Laserlipolysis represents another resource for treating lipodystrophies, whether used alone or as an adjuvant to liposuction. In the study, it showed some advantages compared to liposuction when used alone, mainly in terms of better quality recovery. Laserlipolysis proved to be quite efficient for treating an irregular body contour after liposuction treatment. As a disadvantage, there is the need for training and knowing the physical principies of laser, more time for performing the surgical procedure, in addition to the high cost of equipment.
ACKNOWLEDGEMENTS
The authors would like to thank Dr. Dejalma Johann and staff for the histological studies.
REFERENCES
1. Illouz YG. Une nouvelle technigue pour les lipodystrophies localisées. Ver Chir Esth Franc. 1980;6(9).
2. Apfelberg DB, Rosenthal S, Hunstad JP, Achauer B, Fodor PB. Progress report on multicenter study of laser-assisted liposuction. Aesth Plast Surg. 1994;18(3) :259-64.
3. Apfelberg DB, et al. Results of multicentric study of laser-assisted liposuction. Clin Plast Surg.
1996;23(4):713-9.
4. Cook WR. Laser neck and jowl liposculpture including platysma laser resurfacing, dermal laser resurfacing and vaporization of subcutaneous fat. Dermatol Surg. 1997;23(12):1143-8.
5. Cook WR. Alternative to the facelit. Liposculpture of the face, neck, and jowls with laser dermal resurfacing and platysrnal plication. Dermatol Clin. 1999;17(4) :773-82.
6. Blugerman G. Laserlipolisys for the treatment of localized adiposity and "cellulite". Abstracts of Word Congress on Liposuction Surgery. 2000; Dearborn, Michigan, USA.
7. Schavelzon D, Blugerman G, Goldman A, et al. Laser Lipolisys. Abstracts of the 10th International Symposium on Cosmetic Laser Surgery; 2001; Las Vegas, USA.
8. Neira R. Laser Lipolysis Lipoplastia asistida con laser. Anais do Congreso Colombiano de Cirugía Plástica; 2001; Calí, Colômbia.
9. Neira R. Reportaje clínico de 700 pacientes practicados con técnica lipoescultura laser. In: Anais do Congreso Colombiano de Cirugía Plástica; 2001; Calí, Colômbia.
10. Neira R, Zúfiiga E. Niveles sanguíneos de lidocaína y variables hemodinámicas en lipoescultura laser.
Anais do Congreso Colombiano de Cirugía Plástica; 2001; Calí, Colômbia.
11. Neira R, Isaza C. Efectos del Laser de díodo eléctrico en adipositos humanos cultivados in vitro. Anais do Congreso Colombiano de Cirugía Plástica; 2001; Calí, Colômbia.
12. Solarte E. Efectos de la luz Laser de baja potencia en tejido adiposo. Anais do Congreso Colombiano de Cirugía Plástica; 2001; Calí, Colômbia.
I - Senior Member of the Brazilian Society of Plastic Surgery. Member of the International Society of Aesthetic Plastic Surgery.
II - Plastic Surgeon.
Address for correspondence:
Alberto Goldman, MD
Av.Augusto Meyer, 163 Cj. 1203
90550-110 - Porto Alegre - RS Brazil
Phone: (55 51) 3342-7722
e-mail: alberto@goldman.com.br
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket