



Original Article - Year 2019 - Volume 34 -
Abdominal etching
Lipoaspiração de definição abdominal
Maurício Schneider Salomone Viaro1,*
ABSTRACT
Introduction: Abdominal etching involves improvement of
the appearance of the abdominal musculature by removing fat
from several skin layers, including the superficial layer. This
study evaluated the aesthetic results of abdominal etching
using liposuction.
Methods: The aesthetic results and surgical
complications of female patients were evaluated between 2017
and 2018. All study patients answered a standard questionnaire
about the extent of improvement in body image, overall
satisfaction level, naturalness of the result, and changes in
exercise and dietary habits.
Results: The mean patient age
was 38.97 years, while the mean body mass index was 24.01.
In our sample, 75% of the subjects had previous pregnancies,
25% had previous abdominal surgeries, and 2.5% had a
history of smoking. Simultaneous surgeries were performed
in 90% of cases. The following surgery types were performed:
liposuction alone (40.00%), liposuction + abdominoplasty
(36.25%), miniabdominoplasty (12.50%), abdominoplasty +
liposuction (10.00%), and reverse abdominoplasty (1.25%).
Moderate aesthetic improvement was observed in 86.25%
of the patients, and surgical complications occurred in eight
patients. The satisfaction rate was 91.7%, and the result was
classified as natural by 97.5% of the patients.
Conclusion: Abdominal etching promoted high patient satisfaction and
achieved a natural appearance of the abdomen. This surgical
outcome was achieved using conventional liposuction
without the need for additional techniques. However,
further studies are needed to evaluate long-term outcomes.
Keywords: Lipectomy; Abdominoplasty; Abdominal fat; Body contouring; Aesthetics
RESUMO
Introdução: A lipoaspiração de definição abdominal consiste na criação de sulcos em locais específicos do abdome através da retirada de gordura em toda sua espessura, incluindo a camada superficial, permitindo um maior detalhamento da musculatura. O objetivo deste estudo foi avaliar os resultados da técnica de lipoaspiração na definição abdominal.
Métodos: Foram avaliadas 80 pacientes do sexo feminino no período de 2017 a 2018. O grau de definição e as complicações relacionadas ao procedimento foram avaliadas pelo autor. Todas as pacientes responderam um questionário padrão sobre grau de definição abdominal, satisfação, naturalidade do resultado, aumento da atividade física e melhora da alimentação.
Resultados: A média de idade das pacientes foi de 38,97 anos e a média de índice de massa corporal, 24,01. Gestação prévia foi observada em 75% dos casos, cirurgia abdominal pregressa em 25% e tabagismo em 2,5%. Cirurgias simultâneas foram realizadas em 90%. Em relação ao tipo de cirurgia realizada, ocorreu a seguinte distribuição: 40% lipoaspiração isolada, 36,25% lipoabdominoplastia, 12,5% minilipoabdominoplastia, 10% lipoaspiração pós-abdominoplastia e 1,25% lipoabdominoplastia reversa. Grau 2 de definição abdominal foi observado em 86,25% e complicações ocorreram em 8 pacientes. O índice de satisfação foi de 91,7% e o resultado foi classificado como natural por 97,5% das pacientes.
Conclusão: A lipoaspiração de definição abdominal promoveu um alto índice de satisfação e naturalidade à região abdominal. Esse resultado pode ser atingido através da técnica de lipoaspiração convencional, sem nenhum dispositivo tecnológico adicional. Contudo, são necessários novos estudos para avaliação dos resultados em longo prazo.
Palavras-chave: Lipectomia; Abdominoplastia; Gordura abdominal; Contorno corporal; Estética
INTRODUCTION
Liposuction is among the most commonly performed aesthetic procedures in Brazil and worldwide1,2. Since its inception, several technical improvements have been made; curettage, designated lipexeresis, preceded contemporary fat removal techniques (Schrudde, 1972)3,4. Illouz (1980)5 described another technique involving the use of large-bore blunt cannulae to remove subcutaneous fat, leaving 1-2 cm of subcutaneous cellular tissue to prevent the formation of irregularities5.
Superficial liposuction, one of the most significant advancements in traditional suction-assisted lipoplasty, improves skin retraction and was described by Gasperoni6-9, Gasparotti10-12, and De Souza Pinto13-15. However, this advancement increased the risk of abdominal deformities and irregularities in the abdominal musculature and the production of cutis marmorata when excessive fat was removed.
Liposuction can be performed in isolation or in association with abdominal skin resection. In 1985, Hakme16 introduced the technique of miniabdominoplasty with liposuction, which included elliptical resection of the suprapubic skin in selected cases. Saldanha popularized liposuction associated with abdominoplasty with preservation of the Scarpa fascia without undermining the abdominal flap17. This technique was safe, corrected aesthetic and functional deformities of the abdomen, and produced a better and more harmonious contour of the abdominal musculature. Bozola and Psillakis (1988)18 proposed a new concept of abdominal contouring and a classification based on the deformities of each layer of the abdominal wall and their differentiated treatment in patients eligible for abdominoplasty. The authors noted that a perfect and attractive abdomen is not flat but had relief resembling an English lyre18. Nahas (2001) described a classification for abdominoplasty based on excess skin and subcutaneous deformities19 and another classification based on myoaponeurotic deformities20.
Traditional liposuction failed to give the abdomen a defined contour and produced a flat appearance. Mentz et al. (1993)21 was the first to describe high definition liposculpture, in which selective superficial liposuction was performed to sculpt the abdomens of athletic men. A new concept of liposculpture was created using these principles that allowed surgeons to sculpt the body and enhance the abdominal musculature. Ersek and Salisbury (1997)22 performed superficial liposuction for abdominal etching in 25 athletic men using a customized cannula.
Hoyos (2003)23 improved Mentz’s concepts to a three-dimensional approach involving other muscle groups (trunk, legs, and back) and defined different aesthetic results to be achieved between men and women. Hoyos et al. (2007)24 introduced the combination of vibration amplification of sound energy at resonance (VASER), also known as ultrasonic liposuction, with high definition liposculpture24, miniabdominoplasty25, and liposuction + abdominoplasty26.
Danilla (2017)27 described the rectus abdominis fat transfer (RAFT) technique to improve abdominal contouring using liposuction + abdominoplasty, while Motta (2018)28 introduced the technique of diode lasering combined with high definition liposculpture.
METHODS
Patient selection
All consecutive patients who underwent abdominal liposuction performed by the lead author between November 2017 and November 2018 were selected. All patients were healthy women who were evaluated preoperatively. Patients with extensive abdominal scars and deformities due to previous liposculpture were excluded from the study.
All patients provided written informed consent, including authorization for disclosing images for academic purposes. The study complied with the guidelines of the Declaration of Helsinki and was approved by the Medical Ethics Committee of the Unimed General Hospital of Santa Maria, Rio Grande do Sul, Brazil (protocol no. 0012019).
Surgical procedure
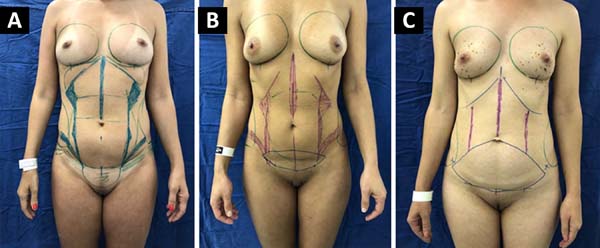
Surgical demarcation was performed with the patient in the standing position. Maneuvers to facilitate palpation of the abdominal and subcostal muscles were performed to identify areas requiring improvement (linea alba, linea semilunaris, subcostal muscles, Spigelian fascia, and oblique muscles) (Figure 1). Matarasso’s classification29 was used to evaluate the type of surgery to be performed.

All procedures were performed under general anesthesia. A thermal blanket and pneumatic compression boot were routinely used. Antimicrobial prophylaxis with 2 g of cefazolin was administered at the time of anesthetic induction.
When liposuction of the dorsal region was indicated, the procedure was started with the patient in prone position. After this stage was completed, the patient was placed in the supine position for finishing the liposuction and performing other surgeries when necessary. The super-wet technique was used with the infiltration of adrenaline in saline (1:1000).
After a mean 15 min, liposuction using a straight 3.5-mm Mercedes cannula connected to a vacuum (MEDAP-BORA UP 2080; Germany) at a constant pressure of 80 cmHg was performed. Deep liposuction was initially performed in the demarcated areas. When abdominoplasty, reverse abdominoplasty, or miniabdominoplasty was indicated, the skin was removed following the surgical markings and the rectus abdominis muscles were plicated when necessary. Next, liposuction was performed in the demarcated areas to define the shape of the abdominal musculature. Only superficial liposuction was performed in cases in which deep liposuction was not indicated.
In the anterior region, the cannula was inserted through one port each in the inguinal region, inframammary fold, and umbilicus. In the dorsal region, the cannula was inserted through one port in the intergluteal cleft and two sites lateral to it, following the contour of the gluteus maximus. Two additional ports located in bilateral paravertebral muscles were used to complement the treatment of the lower back, while two ports located near the scapular region were used treatment in the upper back was necessary.
Prolonged drainage was required in the intergluteal region when liposuction from the dorsal area was extensive or considerable bleeding occurred in this region during the procedure. Drainage was required in the ventral region only in cases involving abdominoplasty. At the end of the procedure, compression bandaging was used in the operated areas in all patients.
The patients received antibiotic prophylaxis of 500 mg of cefadroxil for 7 days and chemoprophylaxis of 40 mg of enoxaparin for 7-14 days starting the morning after surgery.
The mean length of hospital stay for patients undergoing abdominoplasty was 1 day. Patients who underwent liposuction, even when associated with other procedures, were discharged on the day of surgery. The first follow-up visit was on mean day 7 after surgery. Subsequent visits were made at 14 days, 30 days, 3 months, 6 months, and 1 year after surgery. Photographs were acquired in the anterior, lateral, oblique, and posterior views with the patient standing since the first follow-up consultation.
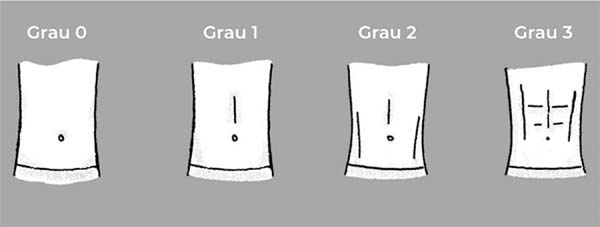
The patients were evaluated by the author for the extent of improvement in body image and surgical complications. The extent of improvement was classified as follows: grade 0, no improvement; grade 1, presence of midline or linea semilunaris, or very faint midline and linea semilunaris; grade 2, well-defined midline and linea semilunaris; and grade 3, significant improvement.
The patients assessed the extent of improvement, overall level of satisfaction, naturalness of the result, and lifestyle changes (exercise and diet) using a standard questionnaire. The extent of improvement was assessed by the patient, who chose one of the schematic drawings that reflected the postoperative abdominal contour (Figure 2).

RESULTS
Eighty female patients were included in this study. The average age was 38.96 (range, 26-63) years, while the average body mass index was 24.01 (range, 18.32-30.97). In addition, 73.75% of patients had previous pregnancies, while 25% had previous abdominal surgeries (liposuction or abdominoplasty). Two (2.5%) patients had a history of smoking. Simultaneous procedures were performed in 90% of the patients. The mean postoperative follow-up period was 7.27 (range, 2-13) months. The following types of surgery were performed: liposuction alone (40.00%), liposuction + abdominoplasty (36.25%), miniabdominoplasty (12.5%), abdominoplasty + liposuction (10.00%), and reverse abdominoplasty (1.25%) (Table 1).
| Variable | Mean | Variation | Percentage |
|---|---|---|---|
| Age | 38,96 | 26-63 | |
| Body mass index | 24,01 | 18,32-30,97 | |
| Previous pregnancy | 59 | 73,75% | |
| Previous abdominal surgery | 20 | 25% | |
| Smoking (No) | 2 | 2,50% | |
| Surgery | 80 | 100% | |
| Liposuction | 32 | 40% | |
| Abdominoplasty + liposuction | 8 | 10% | |
| Liposuction + abdominoplasty | 29 | 36,25% | |
| Miniabdominoplasty | 10 | 12,50% | |
| Reverse abdominoplasty | 1 | 1,25% | |
| Associated surgeries | 72 | 90% | |
| Gluteal fat grafting | 50 | 62,50% | |
| Mammoplasty | 34 | 42,50% | |
| Other surgical procedures | 2 | 2,50% |

Most (86.25%) patients reported moderate (grade 2) improvement in abdominal shape (well-defined midline and linea semilunaris). Five (6.25%) patients had no improvement, while four (5%) and three (3.75%) patients classified the improvement as minor (grade 1) and significant (grade 3), respectively.
Typical complications occurred in four (5%) patients who underwent lipoabdominoplasty, including keloid scars (two cases [2.5%]), seroma (one case [1.25%]), and minor abdominal flap necrosis (one case [1.25%]). Surgical complications occurred in four (5%) patients, including contour asymmetry in the semilunar lines (two cases [2.5%]) and abdominal deformities (two cases [2.5%]) (Table 2).
| Complications | N (%) |
|---|---|
| Typical | |
| Keloid scar | 2 (2,5%) |
| Seroma | 1 (1,25%) |
| Abdominal flap necrosis | 1 (1,25%) |
| Directly related to surgical technique | |
| Asymmetry of the linea semilunaris | 2 (2,5%) |
| Irregularities | 2 (2,5%) |

All patients answered the questionnaire via email or in person. Forty-nine patients (61.25%) classified the improvement as grade 2. Two (2.5%) patients reported no improvement, whereas seven (8.75%) and 22 (27.5%) patients rated the improvement as grades 1 and 3, respectively (Table 3).
| Examiner | Grade 0 | Grade 1 | Grade 2 | Grade 3 |
|---|---|---|---|---|
| Author | 6,25% | 5% | 82,25% | 3,75% |
| Patient | 2,50% | 8,75% | 61,25% | 27,50% |

Most patients were very satisfied (71.25%) with the outcome, 30% were satisfied, and 8.75% were reasonably satisfied. None of the study patients were dissatisfied with the surgical results.
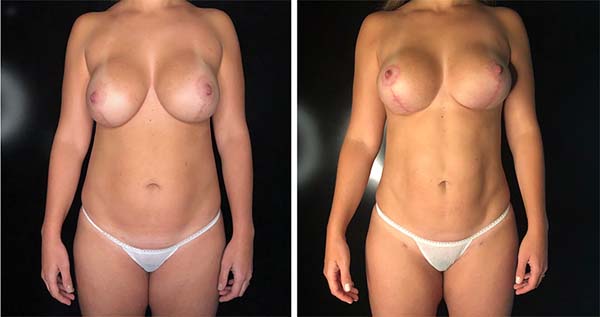
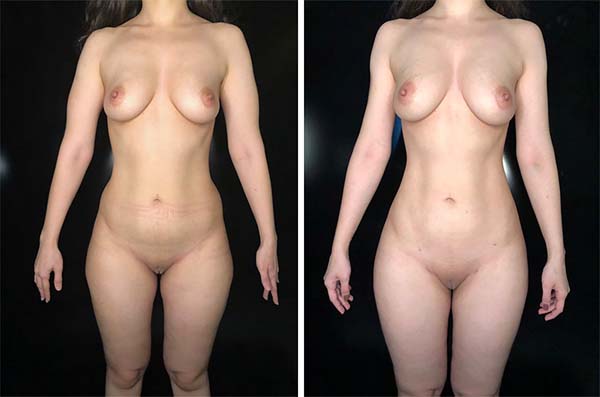
The result was classified as natural by 97.5% of the patients. All patients would undergo the surgery again and would recommend it to another person. Among our sample, 63.5% of the patients increased their physical activity level, 81.25% improved their dietary habits, and 55% lost weight (Figures 3-9).












DISCUSSION
The ideal abdomen is not flat; rather, it is a combination of convex and concave shapes that follow the deep bone and muscle anatomy30.
Superficial liposuction for abdominal etching is an evolution of traditional suction-assisted lipoplasty. The removal of superficial fat is necessary to achieve the abdominal shape of athletes. It consists of enhancing specific areas (alba line, linea semilunaris, subcostal muscles, semilunar fascia, and oblique muscles) by removing fat from all skin layers, including the superficial layer.
Abdominal etching in female patients involves improving the lateral margins and midline of the rectus abdominis muscle but not of transverse tendinous intersections. Women usually prefer partial to complete abdominal etching31.
In the present study, most patients reported intermediate improvement (grade 2) in abdominal shape (well-defined midline and linea semilunaris). Little or no improvement was observed in patients with excessive weight and residual abdominal flaccidity. Almost one-third of the patients rated the improvement as grade 3 (significant), although only 5% (three patients) received this grade by the surgeon. This result may be explained by the subjectivity of the outcome and/or the fact that removal of the deep fat layer above the rectus abdominis muscle combined with adequate eating habits and exercise after surgery favors the appearance of transverse tendinous intersections, improving body contour.
Abdominal etching may help improve patient lifestyles after surgery, including dietary and exercise habits. The present results showed that most patients improved their habits during the study period, particularly diet.
Almost all patients reported that the abdominal contour appeared natural after the procedure, and the high satisfaction rate here (91.25%) agrees with the literature. Hoyos and Millard (2007)24 reported an 84% satisfaction rate of the sample. Hoyos et al. (2018)26 showed a 91.79% satisfaction rate of procedures involving lipoabdominoplasty. Motta (2018)28 observed that all study patients were satisfied with the surgical outcome.
Abdominal etching can be achieved using liposuction, VASER24-26, or lasering28 without the need for other techniques21,22,27. The most effective procedure is unknown because no studies have compared the outcomes of abdominal etching. Mentz et al. (1993)21 used conventional liposuction in the 8 male patients in his study. Danilla (2017)27 found a high degree of abdominal definition in his 26 patients associating rectus abdominis fat grafting with lipoabdominoplasty without the use of associated technologies.
The main complications related to superficial liposculpture are irregularities and asymmetries, which impart an unnatural appearance to the abdomen. In our assessment, 4% of patients had irregularities and/or asymmetries due to excessive liposuction from the deep layers and asymmetrical positioning and/or closer proximity of the linea semilunaris. Hoyos et al. (2007)24 reported that 3.2% of patients had irregularities that required surgical revision.
Most patients presented fibrosis in the abdominal area subjected to superficial liposuction, and the compromised areas healed spontaneously after 6 months or less. Danilla (2017)27 observed that these irregular fibrotic areas resolved spontaneously in 3-4 months and healed completely in up to 8 months.
One of the limitations of this study was its short follow-up period. For this reason, whether the lifestyle changes of these patients continued over time is unknown. In addition, future studies are necessary to assess whether situations such as variability in body weight and pregnancy created loss of naturalness of the result. The literature on the subject is scarce21-28, and few studies have evaluated the results of abdominal etching with long-term follow-up.
CONCLUSION
Abdominal etching using liposuction was very satisfactory and gave a natural appearance to the abdomen. This result can be achieved through conventional liposuction technique without the need for additional technological devices.
COLLABORATIONS
|
MSSV |
Analysis and/or data interpretation, Conception and design study, Conceptualization, Data Curation, Final manuscript approval, Formal Analysis, Funding Acquisition, Investigation, Methodology, Project Administration, Realization of operations and/or trials, Resources, Software, Supervision, Validation, Visualization, Writing - Original Draft Preparation, Writing - Review & Editing |
REFERENCES
1. International Society of Aesthetic Plastic Surgery (ISAPS). ISAPS Global Statistics [Internet]. 2019; [cited 2019 Jan 11]. Available from: https://www.isaps.org/medical-professionals/isaps-global-statistics/
2. Heidekrueger PI, Juran S, Patel A, Tanna N, Broer PN. Plastic surgery statistics in the US: evidence and implications. Aesthetic Plast Surg. 2016 Apr;40(2):293-300. DOI: https://doi.org/10.1007/s00266-016-0611-3
3. Schrudde J. Lipektomie und lipexhaerese im Bereich der unteren Extremitäten. Langenbecks Archiv für Chirurgie. 1977 Dec;345(1):127-31. DOI: https://doi.org/10.1007/BF01305460
4. Schrudde J. Lipexeresis as a means of eliminating local adiposity. Aesthetic Plast Surg. 1980 Dec;4(1):215-26. DOI: https://doi.org/10.1007/BF01575221
5. Illouz YG. Surgical remodeling of the silhouette by aspiration lipolysis or selective lipectomy. Aesthetic Plast Surg. 1985;9(1):7-21. PMID: 2986432 DOI: https://doi.org/10.1007/BF01570678
6. Gasperoni C, Salgarello M. Suction-assisted lipectomy of the subdermal fat layer: a new way of performing liposuction. Annals of the International Symposium Recent Advances in Plastic Surgery. s.l, RAPS International Corporation [Internet]. 1990; [cited 2019 Jan 11]. Available from: http://pesquisa.bvsalud.org/portal/resource/pt/lil-130513 DOI: https://doi.org/10.1007/BF01578339
7. Gasperoni C, Salgarello M, Emiliozzi P, Gargani G. Subdermal liposuction. Aesthetic Plast Surg. 1990;14(2):137-42. PMID: 2333810
8. Gasperoni C, Salgarello M. Rationale of subdermal superficial liposuction related to the anatomy of subcutaneous fat and the superficial fascial system. Aesthetic Plast Surg. 1995 Jan/Feb;19(1):13-20. DOI: https://doi.org/10.1007/BF01578339
9. Gasperoni C, Salgarello M. MALL liposuction: the natural evolution of subdermal superficial liposuction. Aesthetic Plast Surg. 1994 Jun;18(3):253-7. PMID: 7976757 DOI: https://doi.org/10.1007/BF00209305
10. Gasparotti M, Lewis CM, Toledo L. Superficial Liposculpture: manual of technique. New York: Springer-Verlag New York; 1993.
11. Gasparotti M. Superficial liposuction: a new application of the technique for aged and flaccid skin. Aesthetic Plast Surg. 1992;16(2):141-53. PMID: 1570777
12. Gasparotti M. Superficial liposuction for flaccid skin patients. In: Annals of the International Symposium Recent Advances in Plastic. Surgery. 1990;90:441. DOI: https://doi.org/10.1007/BF00450606
13. De Souza Pinto EB, de Almeida AE, Knudsen AF, de Andrade SM, de Medeiros JC. A new methodology in abdominal aesthetic surgery. Aesthetic Plast Surg. 1987;11(4):213-22. PMID: 3445812
14. Souza Pinto EB, Indaburo PE, Muniz Ada C, Martinez YP, Gerent KM, Iwamoto H, et al. Superficial liposuction. Body contouring. Clin Plast Surg. 1996 Oct;23(4):529-48; discussion:49.
15. Souza Pinto EB. Superficial liposuction. Rio de Janeiro (RJ): Revinter; 1999.
16. Hakme F. Technical details in the lipoaspiration associate with liposuction. Rev Bras Cir. 1985;75(5):331-7.
17. Saldanha OR, Souza Pinto EB, Mattos Júnior WN, Pazetti CE, Bello EML, Rojas Y, et al. Lipoabdominoplasty with selective and safe undermining. Aesthetic Plast Surg. 2003 Jul/Aug;27(4):322-7. PMID: 15058559 DOI: https://doi.org/10.1007/s00266-003-3016-z
18. Bozola AR, Psillakis JM. Abdominoplasty: a new concept and classification for treatment. Plast Reconstr Surg. 1988 Dec;82(6):983-93. PMID: 2974166 DOI: https://doi.org/10.1097/00006534-198812000-00008
19. Nahas FX. A pragmatic way to treat abdominal deformities based on skin and subcutaneous excess. Aesthetic Plast Surg. 2001 Sep/Oct;25(5):365-71. DOI: https://doi.org/10.1007/s00266-001-0025-7
20. Nahas FX. An aesthetic classification of the abdomen based on the myoaponeurotic layer. Plast Reconstr Surg. 2001 Nov;108(6):1787-95; discussion:96-7. DOI: https://doi.org/10.1097/00006534-200111000-00058
21. Mentz HA 3rd, Gilliland MD, Patronella CK. Abdominal etching: differential liposuction to detail abdominal musculature. Aesthetic Plast Surg. 1993;17(4):287-90. DOI: https://doi.org/10.1007/BF00437100
22. Ersek RA, Salisbury AV. Abdominal etching. Aesthetic Plast Surg. 1997 Sep/Oct;21(5):328-31. DOI: https://doi.org/10.1007/s002669900131
23. Hoyos AE. High Definition liposculpture. Bucaramanga, Colombia: XIII International Course of Plastic Surgery; 2003.
24. Hoyos AE, Millard JA. VASER-assisted high-definition liposculpture. Aesthet Surg J. 2007 Nov/Dec;27(6):594-604. DOI: https://doi.org/10.1016/j.asj.2007.08.007
25. Hoyos AE, Perez ME, Castillo L. Dynamic definition mini-lipoabdominoplasty combining multilayer liposculpture, fat grafting, and muscular plication. Aesthet Surg J. 2013 May;33(4):545-60. PMID: 23636628 DOI: https://doi.org/10.1177/1090820X13484493
26. Hoyos A, Perez ME, Guarin DE, Montenegro A. A report of 736 high-definition lipoabdominoplasties performed in conjunction with circumferential VASER Liposuction. Plast Reconstr Surg. 2018 Sep;142(3):662-75. DOI: https://doi.org/10.1097/PRS.0000000000004705
27. Danilla S. Rectus Abdominis Fat Transfer (RAFT) in lipoabdominoplasty: a new technique to achieve fitness body contour in patients that require tummy tuck. Aesthetic Plast Surg. 2017 Dec;41(6):1389-99. DOI: https://doi.org/10.1007/s00266-017-0909-9
28. Motta RP. Lipoaspiração laser-assistida de alta definição. Rev Bras Cir Plást. 2018;33(1):48-55.
29. Matarasso A, Swift RW, Rankin M. Abdominoplasty and abdominal contour surgery: a national plastic surgery survey. Plast Reconstr Surg. 2006 May;117(6):1797-808. PMID: 16651953 DOI: https://doi.org/10.1097/01.prs.0000209918.55752.f3
30. Avelar J. Regional distribution and behavior of the subcutaneous tissue concerning selection and indication for liposuction. Aesthetic Plast Surg. 1989;13(3):155-65. PMID: 2801296 DOI: https://doi.org/10.1007/BF01570212
31. Hoyos A, Prendergast PM. High Definition Body Sculpting: art and advanced lipoplasty techniques. Berlin, Heidelberg: Springer-Verlag; 2014.
1. Sa.Vi Medicina, Santa Maria, RS, Brazil.
Corresponding author: Mauricio Schneider Salomone Viaro Avenida Presidente Vargas 2084, sala 1301, Santa Maria, RS, Brazil. Zip Code: 97015-512. E-mail: msviaro@hotmail.com
Article received: January 22, 2019.
Article accepted: June 22, 2019.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket