



Ideas and Innovation - Year 2019 - Volume 34 -
Treatment of marked abdominal wall musculoaponeurotic flaccidity: 26 years of experience
Tratamento da flacidez músculo aponeurótica acentuada da parede abdominal, experiência de 26 anos
Alberto Magno Lott Caldeira1,* ; John Fortunato Jaulis Solórzano1; Kelly Stelle Carrión MAuricio1
; John Fortunato Jaulis Solórzano1; Kelly Stelle Carrión MAuricio1
ABSTRACT
We investigated the causative factors of abdominal support and shape and found that excessive musculoskeletal flaccidity of primary origin causes an inability to support the abdominal wall and may be associated with the predisposing factors. For such cases, we developed a treatment consisting of the placement of a subcutaneous mesh. Here, we present our experience with this treatment. We present a case series of 15 patients in our 26 years of experience who were treated with primary and secondary abdominoplasties. The abdominal wall was reinforced by placing a polypropylene mesh in the submuscular plane with U-stitches in the transversalis fascia, aiming at strengthening the muscle and transverse fascia. The results were satisfactory in the long term. Abdominal bulges were repaired, and muscle harmony was restored. Only two complications occurred: chronic pain localized in the abdomen, which was treated with steroid infiltrations, and an early umbilical fistula with spontaneous and rapid resolution, regardless of the proposal.
Keywords: Abdominoplasty; Muscular diastasis; Muscular atrophy; Secondary treatment; Subcutaneous mesh.
RESUMO
Realizamos uma análise de quais são os elementos responsáveis pelo sustento e formato abdominal, determinando assim, que é devido a uma excessiva flacidez musculoaponeurótica de origem primária, à qual promove uma incapacidade do suporte da parede abdominal e pode estar relacionada a fatores predisponentes. Para esses casos específicos, desenvolvemos um tratamento propondo a colocação da tela e apresentando nossa experiência. Apresentamos esta série de casos de experiência em 26 anos. Onde 15 pacientes foram tratados com abdominoplastia primária e secundária. O reforço da parede abdominal foi realizado através da colocação de tela de polipropileno no plano submuscular com pontos em U na fáscia transversalis, buscando-se fortalecer o músculo e a fáscia transversa. Os resultados foram satisfatórios a longo prazo. Obtendo resolução das protuberâncias abdominais e restaurando a harmonia dos músculos. Apenas duas complicações ocorreram, que foram a presença de dor crônica localizada no abdome tratada com infiltrações de esteroides e fístula umbilical precoce de resolução rápida espontânea, independente da proposta.
Palavras-chave: Abdominoplastia; Diástase muscular; Atrofia muscular; Tratamento secundário; Tela subcutânea
INTRODUCTION
Abdominoplasty is a popular surgical procedure, as the abdominal region is an important functional esthetic unit defining the body contour. We observed some patients with a prominent abdominal bulge, which was difficult to treat based on unsatisfactory results or recurrence with conventional treatments1,2.
This bulge is the chief complaint in most patients undergoing abdominoplasty and is most often caused by rectal diastasis. It may be associated with musculoaponeurotic flaccidity or physiological incompetence, which may have predisposing and aggravating factors, such as age, multiparity, significant weight loss in obese patients, and cesarean section.
The degree of competence of the anterior abdominal wall depends on the balance among the intra-abdominal pressure, visceral movements, diaphragm, and muscular and aponeurosis tensions, determining the presence of abdominal protuberances3,4.
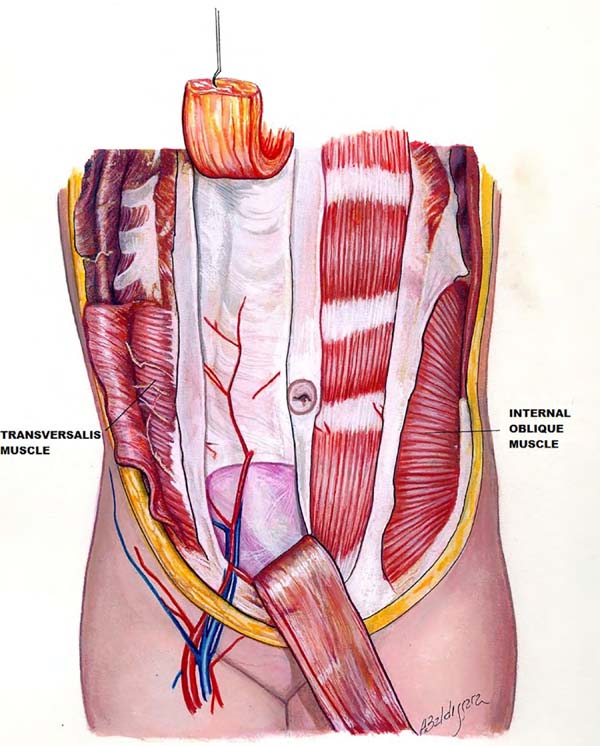
We believe that the protuberances are caused by the diastasis of the rectus abdominis muscle and abdominal wall musculoaponeurotic flaccidity. Therefore, we considered the transversalis fascia and transverse muscle the most important components of the abdomen (Figure 1). We initiated the study in 1993, proposing the treatment by strengthening these structures with polypropylene mesh1,5,6.

METHODS
In 32 years of professional practice, 925 patients were treated with the body contouring surgery. In this period, we observed patients with prominent abdomen showing unsatisfactory results or recurrences.
Fifteen patients were treated (Table 1). Seven patients who underwent primary abdominoplasty and eight patients who underwent secondary abdominoplasty showed an abdominal bulge even after abdominoplasty, and consequently, were not satisfied with the result1,5.
| Patient | Age (years) | Primary Procedure | Secondary Procedure | Complications | Results | |
|---|---|---|---|---|---|---|
| 1 | C.S.M.A.T. | 52 | Abdominoplasty + plication of the rectus abdominis muscle + external oblique flap + liposuction | After 2 years: Abdominoplasty with a polypropylene mesh | None | Satisfactory |
| 2 | M.E.B.P." | 42 | Abdominoplasty + plication of the rectus abdominis muscle + external oblique flap + liposuction | After 14 years: Abdominoplasty with a polypropylene mesh | None | Satisfactory |
| 3 | M.G.E. | 41 | Miniabdominoplasty + plication of the rectus abdominis muscle + external oblique flap + liposuction | After 6 years: Abdominoplasty with a polypropylene mesh | None | Satisfactory |
| 4 | R.C.M.A. | 40 | Miniabdominoplasty + plication of the rectus abdominis muscle + liposuction | After 1 year: Abdominoplasty with a polypropylene mesh | None | Satisfactory |
| 5 | T.M.A.B. | 52 | Abdominoplasty + plication of the rectus abdominis muscle + liposuction | After 15 years: Abdominoplasty with a polypropylene mesh | Chronic pain | Satisfactory |
| 6 | T.J. | 70 | Abdominoplasty + polypropylene mesh + liposuction | - | Chronic pain | Satisfactory |
| 7 | C.X.* | 34 | Fleur-de-Lis abdominoplasty + polypropylene mesh + plication of the rectus abdominis muscle + liposuction | - | None | Satisfactory |
| 8 | A.M.N. | 55 | Abdominoplasty + polypropylene mesh + liposuction | - | None | Satisfactory |
| 9 | L.E.M.C.B. | 51 | Abdominoplasty + polypropylene mesh + plication of the rectus abdominis muscle + liposuction | - | None | Satisfactory |
| 10 | A.I. | 46 | Abdominoplasty + polypropylene mesh + plication of the rectus abdominis muscle + liposuction | - | None | Satisfactory |
| 11 | O.A.P.* | 40 | Anchor abdominoplasty + polypropylene mesh + plication of the rectus abdominis muscle + liposuction | - | None | Satisfactory |
| 12 | R.F.S. | 31 | Abdominoplasty + polypropylene mesh + plication of the rectus abdominis muscle + external oblique flap + liposuction | - | Umbilical fistula | Satisfactory |
| 13 | R.S.C. | 25 | Miniabdominoplasty + plication of the rectus abdominis muscle + liposuction | After 3 years: Miniabdominoplasty + polypropylene mesh | None | Satisfactory |
| 14 | E.C.G. | 30 | Vertical abdominoplasty + polypropylene mesh + liposuction | - | None | Satisfactory |
| 15 | V.C.H.R. | 53 | Abdominoplasty + plication of the rectus abdominis muscle + liposuction | After 20 years: Abdominoplasty with a polypropylene mesh | None | Satisfactory |

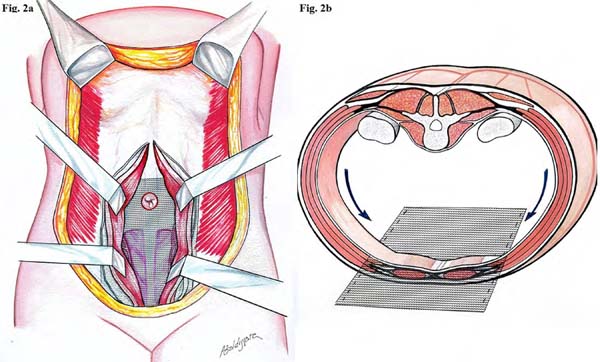
These patients underwent abdominoplasty with a suprapubic incision, which has a curved line of superior concavity than the pre-existing scar. Subsequently, the subcutaneous flap was raised, xiphoid process perforated, and linea alba incised to dissect the rectus abdominis muscle of the posterior aponeurosis layer and transverse fascia, reaching the external border of the rectus abdominis muscle on both sides (Figure 2). We applied the polypropylene mesh in direct contact with the deep aponeurosis layer and transverse fascia, fixing it cranially to the xiphoid process, caudally to the pubis at the origin of the pyramidalis muscle, and laterally to the musculoaponeurotic complex of the oblique and transverse muscles (Figures 3A, 3B and 3C). The mesh was sutured with Prolene 0, U-stitches and was distended over the transverse fascia and posterior sheath of the rectus abdominis muscle, resecting their excesses6,7. Subsequently, the rectus abdominis muscle was continuously sutured (Figures 4A, 4B and 4C). The suction drainage was left underneath the dermal fat flap and closed in three planes.












All patients attended the follow-up for five postoperative years and underwent annual ultrasound examinations of the abdominal wall.
RESULTS
In our observation period, the esthetic results and integrity of the abdominal wall were maintained in the long term and showed no recurrences.
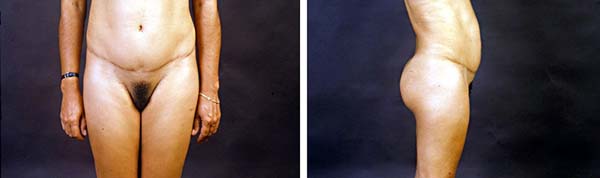
For example, we found a representative case of unsatisfactory results following abdominoplasty by another surgeon in a 42-year-old patient. After the evaluation, a secondary abdominoplasty was performed with plication of the rectus abdominis muscle and external oblique aponeurosis flap8. Despite improvement, a slight upper abdominal projection persisted. She returned 14 years later with the complaint of increased upper abdominal projection. We indicated the performance of an abdominoplasty with reinforcement of the abdominal wall using a polypropylene mesh, fully correcting the abdominal projection, even in the sitting position.
Three complications were observed in our cases. Two patients had localized chronic intermittent pain (laparodinias), which improved with conventional anti-inflammatory drugs and was treated with corticosteroid infiltrations. Another complication was an early umbilical fistula with spontaneous and rapid resolution, regardless of the proposal.
The satisfaction assessments were obtained using the Body-QoL® instrument, which is structured in 5 domains with 20 questions in total. The questions are presented as Likert-type statements in which the patient expresses his/her degree of agreement of that statement9. We administered this instrument in the patients in the postoperative period of 6 months and 5 years, considering the answers in the questionnaires as the final result.
DISCUSSION
It is concluded that this treatment cannot be indicated as the first-line treatment, as many patients with musculoaponeurotic flaccidity obtained satisfactory results with the conventional treatment and therefore, reinforcement with the polypropylene mesh was not necessary. It is necessary to correctly evaluate the recurrent factors, as this treatment consists of an aggressive intervention, which we only recommend for select cases.
The surgeon should know and consider the miodynamism and importance of muscle layers in the appearance of abdominal protuberances, the most important element being the transverse abdominal muscle10. The external oblique muscle causes an upward lateral traction and the descending internal oblique muscle causes two equal antagonistic forces, acting harmoniously. On the other hand, the longitudinal position of the rectus abdominis muscle helps approach the thorax as an antagonist of the spinal muscles3,4,10. Similarly, the transverse muscle allows contraction and expansion of the abdominal wall, keeping the viscera in the correct position and bringing the anterolateral muscles against the strong spine4. These traction forces make the linea alba a neutral support point, allowing the intra-abdominal content to be in perfect balance, promoting normal functioning of the upper diaphragm, which facilitates pulmonary ventilation and the dynamics of the mesenteric complex. The rupture of this balance may lead to consequences, such as rectal diastasis, increase in the abdominal area, change in the center of gravity, change in the lumbar spine, low back pain, decrease in the diaphragmatic domes with decreased pulmonary ventilation, and digestive disturbances resulting from visceral dislocations4. Our proposal is based on the abdominal dynamics, reinforcing the aponeurosis muscle wall, and consequently, restoring abdominal balance.
In our proposal, the mesh is placed over the transverse fascia and posterior to the abdominal rectum, preventing the patient from experiencing the sensation of a foreign body and providing additional protection and a reduced possibility of infection11.
CONCLUSION
One disadvantage we found in our experience was the episode of intermittent localized pain (laparodinias). It is important to note that pain is a subjective complication, and improvement with anti-inflammatory drugs is possible, in addition to determining the correct use of polypropylene mesh in each case. New materials such as ADM and ULTRAPRO will probably be incorporated as the technique evolves, as they provide improved safety owing to the lower number of reactions in other procedures11.
COLLABORATIONS
|
AMLC |
Analysis and/or data interpretation, Conception and design study, Final manuscript approval, Realization of operations and/or trials, Supervision |
|
JFJS |
Analysis and/or data interpretation, Conception and design study, Conceptualization, Data Curation, Realization of operations and/or trials, Writing - Original Draft Preparation, Writing - Review & Editing |
|
KSCM |
Conception and design study, Conceptualization, Data Curation, Realization of operations and/or trials, Writing - Original Draft Preparation, Writing - Review & Editing |
REFERENCES
1. Caldeira AML, Lucas A. Flacidez músculo-aponeurótica abdominal intensa y su tratamiento. Cir Plást Iberolatinoam. 1998;24(1):9-15.
2. Caldeira AML, Robles MBM. Chapter 30 – Challenges in Abdominoplasty, In: Avelar J, editor. New Concepts on Abdominoplasty and Further Applications. Switzerland: Springer Internacional Publishing. 2016. p.481-495. DOI: 10.1007/978-3-319-27851-3_30
3. Testut L, Jacob O. Traité d’Anatomie Topographique. Avec Applications Médico-Chirurgicales. Paris: Gaston Doin; 1909.
4. Alcino LS, Pimenta LG. Técnica da Transposição Peritoneoaponeurótica Longitudinal Bilateral. In: Alcino LS, Luiz GP, editores. Hérnia Incisional. São Paulo: MEDSI; 2004.
5. Caldeira AML, Niéves PA, Oliveira AL. Cirurgia do Contorno Corporal – Reflexões sobre um novo enfoque da cirurgia plástica do abdome. I – Classificações das deformidades abdominais e suas correlações cirúrgicas. Rev Bras Cir. 1990; 80(2):95-104.
6. Usher FC, Ochsner J, Tuttle LL. Use of marlex mesh in the repair of incisional hernias. Am Surg. 1958 Dec;24(12):969-74.
7. Caldeira AML, Niéves PA, Oliveira AL. Cirurgia do Contorno Corporal – Reflexões sobre um novo enfoque da cirurgia plástica do abdome – II Parte. Rev Bras Cir. 1990;80(3):169-186.
8. Psillakis JM. Abdominoplasty: Some ideas to improve results. Aesth Plast Surg. 1978 Dec;2(1):205-215. DOI: 10.1007/bjs.1800590134
9. Anson BJ, McVay CB. Surgical Anatomy. 6th ed. Philadelphia: WB Sauders; 1984.
10. Danilla S, Dominguez C, Cuevas P, et al. The Body-QoL®: measuring patient reported outcomes in body contouring surgery patients. Aesth Plast Surg. 2014 Jun;38(3):575-583. DOI: 10.1007/ s00266-014-0302-x DOI: https://doi.org/10.1007/s00266-014-0302-x
11. Caldeira AML, Carrión K, Jaulis J. Repair of the Severe Muscle Aponeurotic Abdominal Laxity with Alloplastic Mesh in Aesthetic Abdominoplasty. Aesth Plast Surg. 2018 Feb;42(4):1039-1049. DOI: https://doi.org/10.1007/s00266-018-1101-6 DOI: https://doi. org/10.1007/s00266-018-1101-6
1. Instituto Avançado de Cirurgia Plástica Alberto Caldeira, Rio de Janeiro, RJ, Brazil.
Corresponding author: Alberto Magno Lott Caldeira Rua Visconde de Pirajá, 414, Grupo 1012, Ipanema, Rio de Janeiro, RJ, Brasil. Zip Code: 22410-002. E-mail: lottcaldeira@gmail.com
Article received: January 24, 2019.
Article accepted: June 24, 2019.
Institution: Instituto Avançado de Cirurgia Plástica, Hospital Casa Evangélico, Rio de Janeiro, RJ, Brazil.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket