



Original Article - Year 2020 - Volume 35 -
Quality of life of mastectomized women undergoing immediate breast reconstruction in a cancer referral hospital in Amazonas: a cross-sectional study
Qualidade de vida de mulheres mastectomizadas submetidas à reconstrução mamária imediata em hospital de referência oncológica no Amazonas: um estudo transversal
Roberto Alves Pereira1,* ; Hilka Flavia Barra do Espírito Santo Alves Pereira1; Gabriel Pacífico Seabra Nunes2; Edson De Oliveira Andrade3; Valbécia Tavares de Aguiar2
; Hilka Flavia Barra do Espírito Santo Alves Pereira1; Gabriel Pacífico Seabra Nunes2; Edson De Oliveira Andrade3; Valbécia Tavares de Aguiar2
ABSTRACT
Introduction: The assessment of the quality of life is considered important for a more humanistic and comprehensive treatment approach.
Methods: This is a descriptive cross-sectional observational study using a quantitative approach. The quality of life of women undergoing immediate breast reconstruction after mastectomy at the Amazonas Oncology Control Center Foundation (Centro de Controle de Oncologia do Amazonas) from January to June 2015 was assessed. The assessment instrument used was the WHOQOL-BREF questionnaire, following the syntax of the WHOQOL Group.
Results: The sociodemographic profiles of 22 patients were evaluated. The predominant age group was 45-49 years, the predominant educational level was high school (63.64%), 90.91% of the patients were from Manaus, and 72.73% were married. A total of 41% of the respondents defined their quality of life as good in the questionnaire, with the physical domain being the most affected and the social relationships domain being the less affected.
Conclusion: The assessment of the quality of life should be prioritized in the choice of treatment for breast cancer.
Keywords: Plastic surgery; Breast implants; Breast neoplasms; Quality of life; Aesthetics.
RESUMO
Introdução: A avaliação da qualidade de vida é importante para uma abordagem mais humana e abrangente.
Métodos: Trata-se de um estudo observacional transversal descritivo com abordagem quantitativa que avaliou a qualidade de vida em mulheres submetidas à reconstrução mamária imediata após a mastectomia, no período de janeiro a junho de 2015, na Fundação Centro de Controle de Oncologia do Amazonas. O instrumento de avaliação foi o questionário WHOQOL-bref, seguindo a sintaxe do Grupo WHOQOL.
Resultados: Foram avaliadas 22 pacientes, em relação ao perfil sócio demográfico, a faixa etária predominante foi de 45 a 49 anos, o ensino médio foi o mais frequente no estudo (63,64%) e em relação a procedência 90,91% das pacientes foram de Manaus, quanto a estado civil 72,73% eram casadas. Na avaliação através do questionário, a autoavaliação de qualidade de vida foi definida como boa em 41%, o domínio físico apresentou o maior comprometimento, enquanto o domínio de relações sociais foi o menos afetado.
Conclusão: A avaliação da qualidade de vida deve ser parte primordial na escolha do tratamento do câncer de mama.
Palavras-chave: Cirurgia plástica; Implantes de mama; Neoplasias da mama; Qualidade de vida; Estética
INTRODUCTION
Cancer and its treatment still involve a crucial factor, namely body image changes, which are intensively experienced by women. Women with cancer may experience significant emotional and psychosocial trauma. Cancer is a disease that is often associated with death; hence, cancer patients develop a stigma toward the disease. Patients diagnosed with malignant neoplasm experience various losses, extending from the diagnosis to the treatment and prognosis of the disease. In women, body image changes are associated with significant psychological trauma1.
The assessment of the quality of life (QOL) considers the subjective perception of the patient, which is an important step toward a more comprehensive and humanistic approach to cancer treatment. This trend is well documented in the literature due to the increased number of breast cancer studies presenting results obtained through the assessment of the QOL1.
Breast reconstruction can restore the patient’s physical form and integrity, among other demonstrated benefits. In this scenario, psychological well-being plays a crucial role since breast reconstruction can reduce the impact generated by stigmas and the sequelae of cancer surgery. An increasing number of patients are being favored2 by the spread of this surgical technique and its advances.
Indicating immediate breast reconstruction not only optimizes body contour of women but also, causes a positive impact on their QOL. Understanding this should increase the awareness of the importance of this parameter because treatment of the disease is not enough; it is necessary to provide QOL after treatment2.
This study aims to demonstrate, by assessing the QOL questionnaire, the importance of QOL for all professionals involved in the treatment, which would ensure that this parameter is prioritized in the choice of treatment of women with breast cancer at the CECON Foundation (FCECON).
METHODS
This is an observational, cross-sectional, descriptive, quantitative study where we assessed the QOL of women undergoing mastectomy with immediate breast reconstruction through the administration of the WHOQOL-BREF questionnaire. It is a self-explanatory and self-assessment instrument comprising 26 questions related to 4 domains: physical, psychological, social relationships, and environment. Each of the questions was scored on a scale from 1 to 5. The scores of the domains were calculated according to the syntax proposed by the WHOQOL Group ranging from 0 to 100 and following a positive direction, that is, higher scores represented a better assessment of QOL.
The study population comprised women registered at FCECON who underwent a mastectomy and who wanted to undergo immediate breast reconstruction and who spontaneously agreed to complete the WHOQOL-BREF questionnaire. Twenty-two patients were selected.
From January 2015 to June 2015, 51 mastectomies were performed at FCECON (6 in January, 5 in February, 10 in March, 11 in April, 12 in May, and 7 in June). Only 25 patients were selected because the remaining 26 patients had advanced tumors, and the breast service did not indicate immediate reconstruction for these patients (3 in January, 5 in March, 8 in April, 5 in May, and 5 in June). A total of three patients withdrew from the study: one patient decided at the time of surgery not to undergo immediate breast reconstruction after mastectomy (March, 15) and two patients did not undergo breast reconstruction due to tumor growth and loss of surgical margin of safety (1 in March and 2 in May).
The patients answered the questionnaire during outpatient care 30 days after undergoing the surgical procedure of immediate breast reconstruction after mastectomy. The questionnaire was administered during this time because, at that time, patients have not yet received adjuvant treatments, such as chemotherapy and radiotherapy, whose side effects could interfere with QOL.
The study was assessed and approved by the Human Research Ethics Committee of the FCECON (CAAE number: 39808514.4.0000.0004).
RESULTS
The age group with the highest incidence of breast reconstruction was 45–49 years, corresponding to 27.27% of patients, and the age groups with the lowest incidence of breast reconstruction were 60–64 years and 65–69 years, corresponding to 4.55% of patients. High school was the most prevalent educational level, accounting for 63.64% of patients, and higher educational level and complete and incomplete elementary education accounted for 22.73% and 4.55% of patients, respectively. Married, divorced, and single women accounted for 72.73%, 18.18%, and 9.09% of the study sample, respectively.A total of 90.91% of the patients were from Manaus City, and the rest were from the countryside cities of Itacoatiara and Apuí.
A total of 41% of the patients defined their QOL as good, and 5% defined it as bad. Approximately 50% of patients considered themselves very satisfied with their health, while 4% reported dissatisfaction.
In the psychological domain, which assesses the acceptance of physical appearance, 55% of the patients reported being completely satisfied, and the rest was divided between being very satisfied and moderately satisfied. None of the patients reported being completely dissatisfied with their physical appearance. While 5% of patients reported being dissatisfied with themselves, 50% reported being satisfied. A total of 82% of women had negative feelings.
A total of 36%, 9%, and 14% of patients reported being satisfied, being very satisfied, and being dissatisfied with their performance in daily activities, respectively.
Regarding social relationships, while 46% of patients reported being satisfied with their sexual life, 13.5% reported being dissatisfied. In the subjective self-assessment of personal relationships, 46% of patients reported being very satisfied, and only 9% reported being dissatisfied to some extent.
As shown in Table 1, although there was no significant difference between the domains, the scores for personal relationships and self-assessment of QOL domains were slightly higher than those of other domains.
| Domínio | Mean | Standard Deviation |
Coefficient Of Variation |
Minimum Value | Maximum Value | Extent |
|---|---|---|---|---|---|---|
| Physical | 15.01 | 2.36 | 15.72 | 10.86 | 18.86 | 8.00 |
| Psychological | 15.58 | 2.33 | 14.98 | 7.33 | 18.00 | 10.67 |
| Social relationships | 16.00 | 3.05 | 19.07 | 8.00 | 20.00 | 12.00 |
| Environment | 15.70 | 1.89 | 12.02 | 12.00 | 19.00 | 7.00 |
| Self-assessment of QOL | 16.73 | 3.30 | 19.71 | 8.00 | 20.00 | 12.00 |
| Total | 15.60 | 1.96 | 12.55 | 9.85 | 18.62 | 8.77 |

Figure 1 shows the means of the domains’ scores of the questionnaire for assessing the QOL on a scale from 0 to 100. All domains had an approximate score of 72.51, with the physical domain having the lowest score of 68.83.
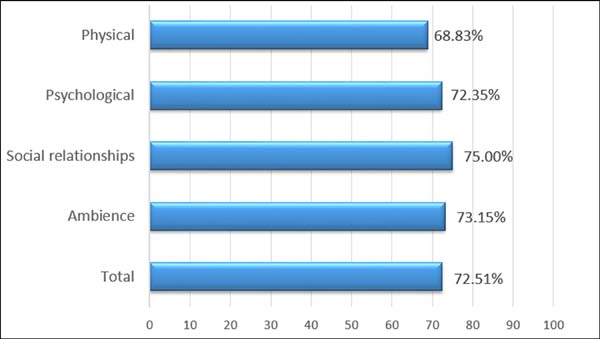

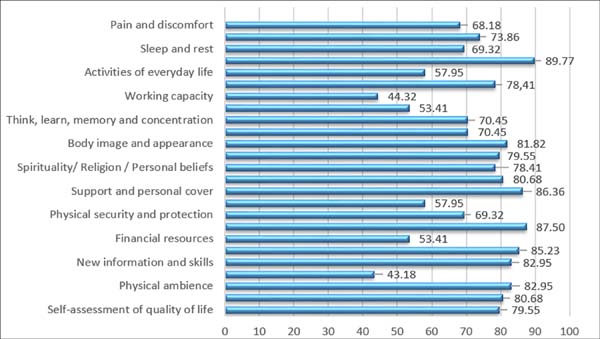
Figure 2 shows the means of the scores of the 24 facets and the QOL self-assessment question on a scale from 0 to 100. The mobility facet, which belongs to the physical domain, had the best score, with 89.77. However, the environment domain, represented by the recreation and leisure facet, had the lowest score, with 43.18. The score of self-assessment of QOL was 79.55, showing that the patients had good QOL.

DISCUSSION
The predominant age group undergoing breast reconstruction was 45–49 years, corresponding to 27.27% of patients. The age groups 40–44 years and 55–59 years corresponded to 22.73% of patients. Gomes et al., in 20153, conducted a cross-sectional study with 37 women and observed a mean age of 57 years and a prevalence of 72% of women aged 50 years or higher. Similarly, Garcia et al., in 20184, conducted a cross-sectional study with 35 women and observed a mean age of 50 years.
High school was the predominant educational level, corresponding to 63.64% of the patients assessed. Complete and incomplete elementary education corresponded to 4.55% of patients. Seidel et al., in 20175, assessed 35 patients in the State of Santa Catarina and observed a prevalence of 53.1% of patients who had completed high school. Ferraz, in 20096, observed that 65% of patients had incomplete elementary education, and 16.7% had completed high school, a result which is inconsistent to the results obtained in the present study.
Married women were predominant, corresponding to 72.73% of the study sample; moreover, 18.18% and 9.09% of women were divorced and single, respectively. Hughet et al., in 20097, conducted a cross-sectional study with 110 women in Campinas (São Paulo) and observed that 68% of them were married. Seidel et al., in 20175, found a similar result in their study conducted in 58 women in Santa Catarina with a prevalence of 56.6% of married women, which is consistent with the results obtained in the present study.
A total of 90.91% of patients were from the Manaus City, and the rest were from the countryside cities of Amazonas. Pereira et al., in 2017,8, assessed 211 women from 2003 to 2013 at FCECON and observed that 21% were from countryside cities different from those of the present study.
A total of 41% of patients defined their QOL as good. Our results were consistent with the results obtained from the study of Paredes et al., in 20139, who assessed 27 women in Fortaleza and obtained a satisfaction level of 41%.
The physiological score was 72.35, which is close to the scores obtained by Gomes et al., in 20153, 71.87, and by Fuga, in 201610, who assessed 18 patients in Rio Grande do Sul and found a mean age of 55.83 years and a score of 75.17.
The physical domain had the lowest score, with 68.83. This finding is consistent with the findings observed in the study of Garcia et al., in 20184, in which the physical domain score of the 35 women assessed was 65.09. Jorge e Silva, in 201011, conducted a cross-sectional descriptive study with 50 patients in the region of Triângulo Mineiro, from August 2007 to April 2009, and observed that the physical domain was the most affected, with a score of 56.00.
Kluthcovsky and Urbanez, in 201212, conducted a cross-sectional study with 199 women in Paraná and observed that the social relationships domain had the highest score, a result consistent with the results obtained in the present study, with a social relationship score of 75.00. However, in the study by Gomes et al., in 20153, comprising 37 patients, the social relationships domain had a score of 62.39.
Jorge e Silva, in 201011, and Garcia et al., in 20184, found low environment scores, 58.10 and 60.31, respectively. The present study had different results, with a score of 73.15.
Paredes et al., in 20139, assessed 27 mastectomized women undergoing immediate or late breast reconstruction using the WHOQOL-BREF questionnaire and found that women who underwent late reconstruction were more satisfied compared to women who underwent immediate breast reconstruction.
CONCLUSION
When analyzing the criteria for QOL, negative feelings had an unfavorable outcome. However, breast reconstruction had a positive impact on the physical, social relationships, and environment domains.
The assessment of the QOL of women undergoing breast carcinoma treatment should be prioritized in the choice of surgical treatment since body image directly influences their QOL. In this way, breast reconstruction can provide this woman with an improved body contour, which will directly impact her QOL.
QOL should be prioritized in the choice of treatment to be offered to women with breast cancer. Further studies will certainly demonstrate the importance of this assessment.
COLLABORATIONS
|
RAP |
Analysis and/or data interpretation, Conception and design study, Conceptualization, Data Curation, Final manuscript approval, Formal Analysis, Funding Acquisition, Investigation, Methodology, Project Administration, Realization of operations and/or trials, Resources, Visualization, Writing - Original Draft Preparation, Writing - Review & Editing |
|
HFBESAP |
Writing - Original Draft Preparation, Writing - Review & Editing |
|
GPSN |
Data Curation |
|
EOA |
Writing - Review & Editing |
|
VTA |
Data Curation |
REFERENCES
1. Oliveira RR, Morais SS, Sarian LO. Efeitos da reconstrução mamária imediata sobre a qualidade de vida de mulheres mastectomizadas. Rev Bras Ginecol Obstetr [Internet]. 2010; [cited 2018 jun 20]; 32(12):602-8. Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0100-72032010001200007
2. Angheben E, Garnica G. Oncoplastia mamaria. Rev Argent Cancerol. 2014;42(1):41-8.
3. Gomes NS, Soares MBO, Silva SR. Autoestima e qualidade de vida de mulheres submetidas à cirurgia oncológica de mama. Rev Min Enferm. 2015;19(2):120-6.
4. Garcia CP, Barazzetti DO, Rendón NB, Parente ELM, Vasconcelos ZAA, Ely JB. Avaliação da qualidade de vida em pacientes submetidas à reconstrução mamária no Mutirão Nacional da SBCP ano de 2016 em Santa Catarina. Rev Bras Cir Plást. 2018;33(Supl 1):172-5.
5. Seidel W, Bins-Ely J, Barazzetti DO, Giustina RD, Walter GP, Ferri TA, et al. Breast reconstruction after mastectomy for breast câncer: comparative analysis of early and delayed reconstruction. Minerva Chir. 2017;72(3):188-99.
6. Ferraz AMN. Avaliação da qualidade de vida de mulheres mastectomizadas [dissertação]. Rio Grande do Sul: Universidade Federal do Rio Grande do Sul – Programa de Pós-graduação em Medicina; 2009.
7. Hughet PR, Morais SS, Osis JMD, Pinto-Neto AM, Gurgel MSC. Qualidade de vida e sexualidade de mulheres tratadas de câncer de mama. Rev Bras Ginecol Obstet. 2009;31(2):61-7.
8. Pereira HFBESA, Viapiana OS, Silva KLT. Aspectos clínicos e patológicos do câncer de mama em mulheres jovens atendidas na FCECON entre 2003 e 2013. Rev Bras de Cancerologia. 2017;63(2):103-9.
9. Paredes CG, Pessoa PSG, Peixoto DTT, Amorin DN, Araújo JS Barreto PRA. Impacto da reconstrução mamária na qualidade de vida de pacientes mastectomizadas atendidas no Serviço de Cirurgia Plástica do Hospital Universitário Walter Cantídio. Rev Bras Cir Plást. 2013;28(1):100-4.
10. Fuga FM. Avaliação da qualidade de vida e da autopercepção corporal em mulheres com câncer de mama submetida à reconstrução mamária [dissertação]. Porto: Universidade Fernando Pessoa – Fisioterapia Materno-infantil; 2016.
11. Jorge LLR, Silva SR. Avaliação da qualidade de vida de portadora de câncer ginecológico. Rev Latino-Am Enfermagem. 2010 Set/Out;18(5):[aprox. 7 telas].
12. Kluthcovsky ACGC, Urbanetz AAL. Qualidade de vida em pacientes sobreviventes de câncer de mama comparada à de mulheres saudáveis. Rev Bras Ginecol Obstetr. 2012;34(10):453-8.
1. Fundação Centro de Controle de Oncologia do Amazonas, Manaus, AM, Brazil.
2. Universidade Nilton Lins, Faculdade de Medicina, Manaus, AM, Brazil.
3. Universidade Federal do Amazonas, Programa de Pós-Graduação Stricto Sensu, Manaus,
AM, Brazil.
Corresponding author: Roberto Alves Pereira Rua Acre, 12, Salas 519/520, Cemon Building, Manaus, AM, Brazil. Zip Code: 69053-130. E-mail: robertopereiracp@me.com
Article received: June 19, 2019.
Article accepted: February 22, 2020.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket