



Original Article - Year 2020 - Volume 35 -
Surgical treatment for breast ptosis with silicone prosthesis: evaluation of surgical results and patient satisfaction
Tratamento cirúrgico de ptose mamária com inclusão de prótese de silicone: avaliação de resultados cirúrgicos e satisfação de pacientes
Giselly de Fátima Mendes Pascoal1,* ; Jorge luiz abel2; Geraldo Scozzafave3
; Jorge luiz abel2; Geraldo Scozzafave3
ABSTRACT
Introduction: The correction of breast ptosis associated with skin flaccidity is done through mastopexy with the inclusion of an implant. This work's objective was to evaluate the surgical results and the satisfaction of patients who underwent breast ptosis surgery with silicone prosthesis placement.
Methods: We selected 22 patients who underwent mastopexy with implant placement, from February to September 2016, at the Plastic Surgery Service of Hospital Heliópolis. Interviews were conducted applying to the patients a questionnaire to verify the degree of satisfaction and changes in the daily routine after surgery. The surgical results evaluation was carried out by three surgeons, who attributed scores to different items.
Results: 100% of the interviewees feel satisfied with the surgery, and all reported an improvement in their self-esteem. In the evaluation of surgeries performed with surgeons, about 91% of the results are between regular and good.
Conclusion: The degree of patient's satisfaction who underwent mastopexy with insertion was excellent. There was a favorable impact on the quality of life and well-being of the patients evaluated, with the post-surgical result being classified as regular or good.
Keywords: Plastic surgery; Breast implants; Mammoplasty; Self-image; Silicone gels
RESUMO
Introdução: A correção da ptose mamária associada à flacidez de pele é corrigida através
da mastopexia com inclusão de implante. O objetivo deste trabalho foi
avaliar os resultados cirúrgicos e a satisfação de pacientes submetidas à
cirurgia de ptose mamária com inclusão de prótese de silicone.
Métodos: Foram selecionadas 22 pacientes submetidas à mastopexia com inclusão de
implante, no período de fevereiro a setembro de 2016, no Serviço de Cirurgia
Plástica do Hospital Heliópolis. Foi realizada entrevista com as pacientes,
por meio de aplicação de questionário, com a finalidade de verificar o grau
de satisfação e as alterações no cotidiano diário após a cirurgia. A
avaliação dos resultados cirúrgicos foi realizada mediante avaliação de três
cirurgiões, do qual atribuíram notas a diferentes itens.
Resultados: 100% das entrevistadas se sentem satisfeita com a cirurgia e todas relataram
a melhora da autoestima delas. Na avaliação das cirurgias realizada com os
cirurgiões, cerca de 91% dos resultados estão entre regular e bom.
Conclusão: O grau de satisfação das pacientes submetidas à mastopexia com inserção foi
excelente e houve impacto favorável na qualidade de vida e bem-estar das
pacientes avaliadas, sendo que o resultado pós-cirúrgico se enquadra como
regular ou bom.
Palavras-chave: Cirurgia plástica; Implantes de mama; Mamoplastia; Autoimagem; Géis de silicone
INTRODUCTION
Breast ptosis is characterized by breasts fall, decreased volume, sagging skin, or both. It is an alteration resulting from the inadequate relationship between the breast skin and its content1. It can be defined in varying degrees, according to the relationship between the nipple and the inframammary fold2.
Mastopexy is plastic surgery that treats breast ptosis, aiming to improve the breast’s shape through tiny scars, the anatomical repositioning of the breasts and the nipple-areola complex, avoiding lesions or neurovascular changes3.
The correction of breast ptosis is done with an increase in breast volume through silicone implants or removal of excess skin and lifting (mastopexy), or the association between them. Mastopexy associated with silicone implants is considered a more complex procedure than mastopexies without implants, due to the variable results, relapses, and related complications4.
The correction of breast ptosis associated with skin flaccidity is still a topic of discussion and controversy. The critical analysis of aesthetic results and patient and team satisfaction is not well established in the literature5. On the other hand, patients have become increasingly critical about the result of breast surgery, as they expect a natural, lasting shape and minimal scarring6.
OBJECTIVE
This study’s objective was to evaluate the surgical results and the satisfaction of patients who underwent mastopexy with an implant, from February to September 2016, at the Plastic Surgery Service of Hospital Heliópolis.
METHODS
We selected all patients who underwent mastopexy with breast implant operated by the same resident doctor from the last year of plastic surgery, from February to September 2016, at the Plastic Surgery Service of Hospital Heliópolis.
Twenty-two patients were counted and followed from the preoperative outpatient interview until the 6(th) postoperative month when they were discharged.
All patients were initially screened at the outpatient clinic, being subjected to a directed medical interview with clarification about the surgery, expectations, and possible complications. Further laboratory tests were requested, including complete blood count, complete biochemistry, serology for HIV (human immunodeficiency virus) and hepatitis, beta HCG (human chorionic gonadotropin), and liver function as well as chest X-ray, electrocardiogram and cardiological consultation.
After this screening, the patients were photographed, then the surgical planning, length of stay, complications, and the size and shape of the prosthesis were discussed.
Inclusion factors: female gender, aged between 18 and 70 years, not having undergone previous plastic surgery in another service, stable weight with BMI (body mass index) up to 28, and presenting a deficient breast volume that justified the placement of the prosthesis.
Exclusion factors: being a smoker, having uncontrolled comorbidities, history of previous surgical complications, refusing to sign a free and informed consent form for the study, having laboratory alterations, or high risk that contraindicate the surgery, and emotionally unstable patients or who do not understand the procedure surgical.
Two questionnaires were carried out for the present study. The first questionnaire included data regarding age, prosthesis shape, profile, implant volume, surgical reintervention, intraoperative complications, postoperative complications, the distance between the wishbone and point A, the scar shape ( periareolar, inverted T, areola and vertical), mammary pocket plane (subglandular, subfascial and submuscular), capsular contracture (Baker scale), degree of previous ptosis and pregnancy.
The analysis followed the principles of resolution 466/2012 of the National Health Council, which deals with the ethical and legal aspects of research involving human beings in Brazil.
The second questionnaire included an interview directed at the satisfaction with the surgery and if it interfered with the patients’ social, sexual life, and body care.
Evaluation of surgical results
A critical and qualitative analysis of the 22 patients’ surgical results was carried out. Three different plastic surgeons from the Plastic Surgery Service of Hospital Heliópolis with experience in performing mastopexy with a prosthesis compared the pre- and postoperative photographs. For this, a questionnaire with five items (Chart 1) was used as described in Cintra Júnior et al. in 20167.
| Scores | 0 - Bad | 1 - Regular | 2 - Good |
|---|---|---|---|
| Breast form | Inadequate | Regular | Adequate |
| Breast volume | Inadequate and disharmonious | Adequate and disharmonious | Adequate and harmonic |
| Inadequate and disharmonious | |||
| Symmetry between breasts | Very different | Little different | Equal or very similar |
| Posicionamento NAC* | Away from the breast cone apex | Near the breast cone apex | Exactly at the breast cone apex |
| Quality and extent of scars | Alargadas | Slightly enlarged and well-positioned | Thin, clear and well-positioned |
| Hypertrophic or very extensive |

After data collection, a results descriptive evaluation was performed.
RESULTS
In the protocol for evaluating the surgical results obtained through the application of the questionnaires, the following data were recorded: age ranging from 26 to 69 years; weight from 49 to 77kg; prosthesis shape: 100% round; profile: 54.54% high, 31.81% super high and 13.63% moderate; implant volume: 240 to 350ml; reintervention: 13.63% of cases; and intraoperative complication: 0%.
Regarding patients who presented complications in the postoperative period, it was observed that 14 patients had some type of complication or more than one type (Table 1).
| Number of cases | Complications |
|---|---|
| 4 | Enlargement |
| 1 | Enlargement + dehiscence |
| 1 | Enlargement + dehiscence + asymmetry |
| 3 | Asymmetry |
| 4 | Hypertrophic scar |
| 2 | Dark scar |
| 1 | Hematoma |
| 1 | Inflammation |
| 2 | Serous secretion |
| 1 | Necrosis |
| 1 | Infection |
| 1 | Keloid |

It was found that three patients needed surgical reintervention, one of the cases was due to asymmetry and scarring, another to perform the resuture and the third to perform hematoma drainage.
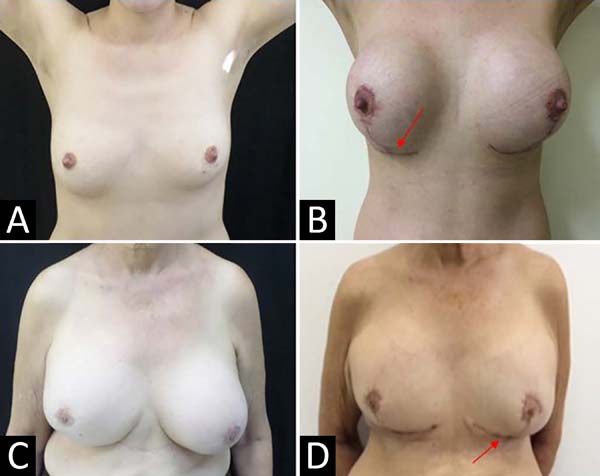
Regarding the shape of the scar, 31.81% of the patients had a periareolar shape, 45.45% an inverted T shape (Figure 1), and 22.72% a vertical periareolar shape.

In the breast pocket plane, 63.63% were subglandular, 31.81% subfascial, and 4.5% submuscular.
Capsular contracture was seen in only one patient, with four on the Baker scale. Type 1 ptosis was observed in 40.90% of patients, type 2 in 50.0%, and type 3 in 9.0%. Regarding the number of pregnancies, 45.45% of the patients had two pregnancies, 40.90% had one pregnancy, and 13.63% had no pregnancy.
When questioning patients’ satisfaction with the surgery, it was found that most patients were satisfied with the change after surgery (Table 2).
| Question | Yes | No |
|---|---|---|
| Do your breasts interfere with professional life? | 7 | 15 |
| Did you regret having the surgery? | 0 | 22 |
| Did surgery influence social life? | 15 | 7 |
| Did the surgery influence the affective life? | 16 | 8 |
| Did surgery influence sex life? | 16 | 8 |
| Are you satisfied with the result of breast surgery? | 22 | 0 |
| Was the result of the surgery close to what you heard from the plastic surgeon? | 22 | 0 |
| Is the result close to what you expected? | 22 | 0 |
| Did the surgery change your life? How? | 22 | 0 |
| Self-esteem | ||
| Did breast surgery affect body care? | 16 | 8 |
| Are you satisfied with your breasts? | 21 | Partly |
| Has your body improved? | 22 | 0 |
| Are you satisfied with your body? | 21 | 1 |
| Do you believe that breast surgery has anything to do with satisfaction with your body? | 21 | 1 |

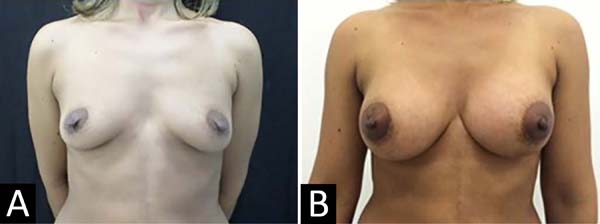
When the patients were asked what they liked most about the result of the breast surgery, most of them (50%) reported that they liked everything (Figure 2) and the others said they liked the volume, the shape, the correction of the ptosis and the removal of excess skin.

On the other hand, when asked about what they liked least about the result of the surgery, 50% answered that nothing, that is, they liked everything, 33.3% did not like the scar (Figure 3) and a smaller percentage even mentioned the points and pain as an answer to this question.
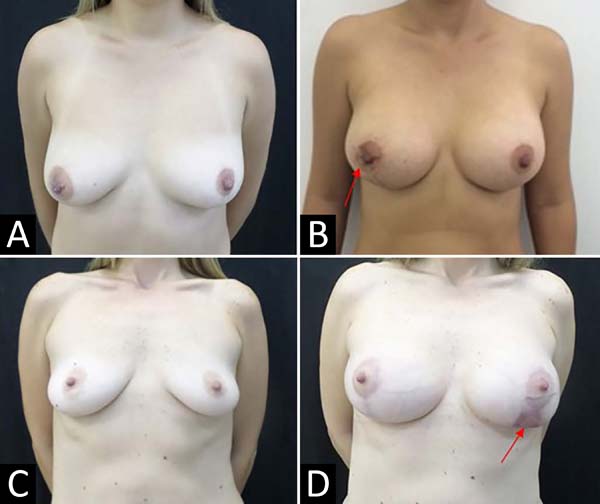

It is possible to observe in Figure 3D that the left breast had an abnormal scar, around the areola and vertically, and it was also one of the patients that presented asymmetry, as can also be seen in Figure 4. This patient was one of the three patients that needed surgical reintervention for correction.


Regarding the evaluation carried out by the three surgeons, it is possible to observe the divergence of the results among them. However, it is noteworthy that the majority of patients fit the post-surgical result, in regular or good in the different items evaluated (Table 3), and only 8,8% of the results were considered bad.
| Evaluated items | Score 0 | Score 1 | Score 2 |
|---|---|---|---|
| Surgeon 1 | |||
| Form | 1 | 5 | 16 |
| Volume | 1 | 3 | 18 |
| Symmetry | 2 | 9 | 11 |
| NAC* | 3 | 7 | 12 |
| Scar | 3 | 10 | 9 |
| Surgeon 2 | |||
| Form | 1 | 15 | 6 |
| Volume | 1 | 7 | 14 |
| Symmetry | 1 | 8 | 13 |
| NAC | 2 | 15 | 5 |
| Scar | 2 | 10 | 10 |
| Surgeon 3 | |||
| Form | 2 | 10 | 10 |
| Volume | 0 | 11 | 11 |
| Symmetry | 1 | 12 | 9 |
| NAC | 3 | 10 | 9 |
| Scar | 6 | 7 | 8 |
| Total (%) | 29 (8,8) | 139 (42,2) | 161 (48,9) |
* NAC: Nipple-areola complex.

DISCUSSION
Female breasts are essential symbols of femininity, sexuality, and motherhood. Thus, they are extremely related to female psychosexual well-being8. Therefore, in the last few years, the number of breast surgeries performed has increased a lot. However, this increase has, consequently, also a more significant number of complications9,10. In this study, a considerable number of patients were observed who presented some type of complication in the postoperative period, but the complications presented were of lesser intensity.
The objectives of breast surgeries are focused on a good evaluation of the final aesthetic result and a postoperative free of complications. For the patient, it is a satisfactory result from both an aesthetic and functional point of view, improving her quality of life in several aspects11.
In the present study, half of the patients had their inverted T-type scars. According to Neligan, in 201512, the various surgical approaches to mastopexy are divided based on the scar’s pattern. There are four basic scar patterns for mastopexy techniques: periareolar, vertical, J or L, and inverted T.
Regarding the breast pocket plane, 75% of patients had the subglandular plane. According to Spear et al., in 20041, in daily surgical practice, inserting a silicone implant, particularly in the subglandular plane, seems simple. However, the indications for the best tissue plane to use for implant coverage and association with mastopexy can become challenging, eventually requiring secondary procedures1.
Among the existing mastopexy techniques, Neligan, in 201512, states that the periareolar technique is the most suitable for patients with mild to moderate breast ptosis, which would be the case for more than 83% of the patients evaluated in this study. In this technique, firmer parenchyma is preferable to more flaccid tissues. The incisions for this technique range from an upper half moon to a full circle of removed skin.
Mild ptosis was defined as presenting the nipple 1 cm from the inframammary fold and being above the breast’s lower pole. In moderate ptosis, the nipple is 1-3 cm below the inframammary fold but is still above the breast’s lower pole. In severe ptosis, the nipple is more than 3 cm below the inframammary fold and is located below the lower breast contour. In pseudoptosis, the nipple is above the inframammary fold, but most of the breast tissue is below and gives the appearance of ptosis2.
Regarding the questioning about the patients’ satisfaction with the surgery, Ozgür et al., in 199813, affirm that psychology should be an integral part of plastic surgery since many patients showed relief from psychological and social problems after the surgical procedures.
All patients reported that they did not regret having the surgery and said that the surgery result was within the expected expectations; only one was partially satisfied because she would like it to get bigger. According to Neligan, 201512, most patients come to the consultation with some notion of what to expect from the surgery. These predetermined ideas come from internet research and image observation and conversations with other people who have undergone mastopexy.
All patients evaluated stated that their self-esteem improved after the surgery. In this sense, several studies have already been carried out, highlighting the improvement in self-esteem11,14. According to Santos et al., in 201915, in a study with patients who underwent breast surgery, most were dissatisfied with the body in the pre-surgical period and pointed out the breast as the most significant discomfort, and the desire to raise self-esteem showed as the primary motivation among the evaluated group. Finally, the authors report that the level of post-surgical satisfaction among patients was high, with surgery interfering in professional, personal, and sexual aspects.
When asked about what they liked least about the surgery, about 33% of patients reported that they did not like the scar. In 201512, Neligan stated that although scars are an inherent part of any surgical procedure, their final quality cannot be predicted. According to Sanfelice and André, in 200716, the breasts have very varied shapes, and therefore they must have specific approaches for each type in particular and, consequently, they can present different results in the face of surgery due to this variation.
Among the characteristics mainly cited by patients they liked the most, are the increase in volume and the reduction of sagging. Mansur and Bozola, in 200917, claim that most patients who seek breast plastic surgery, want larger breasts and correction of flaccidity.
Regarding the difference between surgeons in the results obtained, the significant variability and subjectivity in the evaluation of the items analyzed are perceived, which was also reported in a study carried out by Cintra Júnior et al., in 20167. However, these same authors affirm that the weak agreement between the scores awarded by the evaluators do not invalidate the results obtained.
However, it is noteworthy that surgeons considered 91.1% of surgeries to be regular or good, demonstrating that even surgeons considered surgeries with satisfactory results.
CONCLUSION
The degree of satisfaction of patients who underwent mastopexy with insertion was excellent, and there was a favorable impact on the quality of life and well-being of the patients evaluated.
In the evaluation of plastic surgeons, the post-surgical results of mastopexy with insertion of the evaluated patients, the majority, 90%, of the items were considered to be fair or good.
REFERENCES
1. Spear SL, Pelletiere CV, Menon N. One-stage augmentation combined with mastopexy: aesthetic results and patient satisfaction. Aesthetic Plast Surg. 2004 Nov;28(5):259-67. DOI: https://doi.org/10.1007/s00266-004-0032-6
2. Regnault P. Breast ptosis. Definition and treatment. Clin Plast Surg. 1976 Abr;3(2):193-203.
3. Rohrich RJ, Gosman AA, Brown AS, Reisch J. Mastopexy preferences: a survey of board-certified plastic surgeons. Plastic Reconstr Surg. 2006 Dez;118(7):1631-8. DOI: https://doi.org/10.1097/01.prs.0000248397.83578.aa
4. Spear SL, Low M, Ducic I. Revision augmentation mastopexy: indications, operations, and outcomes. Ann Plast Surg. 2003 Dez;51(6):540-6. DOI: https://doi.org/10.1097/01.sap.0000096450.04443.be
5. Hurwitz DJ, Agha-Mohammadi S. Postbariatric surgery breast reshaping: the spiral flap. Ann Plast Surg. 2006 Mai;56(5):481-6. DOI: https://doi.org/10.1097/01.sap.0000208935.28789.2d
6. Daher JC, Amaral JDLG, Pedroso DB, Cintra Júnior R, Borgatto MS. Mastopexy associated with submuscular or subglandular silicone implants: indications and complications. Rev Bras Cir Plást. 2012 Jun;27(2):294-300. DOI: http://dx.doi.org/10.1590/S1983-51752012000200021
7. Cintra Júnior W, Modolin MLA, Rocha RI, Gemperli R. Augmentation mastopexy after bariatric surgery: evaluation of patient satisfaction and surgical results. Rev Col Bras Cir. 2016 Jun;43(3):160-4. DOI: https://doi.org/10.1590/0100-69912016003005
8. Pitanguy I, Bretano J, Ramalho MC, Porto MJ. Implante de silicone gel com revestimento de poliuretano. Rev Bras Cir Plást. 1990;80(2):119-30.
9. Grewal NS, Fisher J. Why do patients seek revisionary breast surgery?. Aesthet Surg J. 2013 Fev;33(2):237-44. DOI: https://doi.org/10.1177/1090820X12472693
10. Hanwright PJ, Hirsch EM, Seth AK, Chow G, Smetona J, McNichols C, et al. A multi-institutional perspective of complications rates for elective non-reconstructive breast surgery: an analysis of NSQIP data from 2006 to 2010. Aesthet Surg J. 2013 Mar;33(2):378-86. DOI: https://doi.org/10.1177/1090820X13478819
11. Freire M, Sabino Neto M, Garcia EB, Quaresma MR, Ferreira LM. Functional capacity and postural pain outcomes after reduction mammaplasty. Plast Reconstr Surg. 2007 abr;119(4):1149-56. DOI: https://doi.org/10.1097/01.prs.0000254358.55104.9f
12. Neligan PC. Cirurgia plástica. 3ª ed. Rio de Janeiro: Elsevier; 2015. v. 5.
13. Ozgür F, Tuncali D, Güler GK. Life satisfaction, self-esteem, and body image: a psychosocial evaluation of aesthetic and reconstructive surgery candidates. Aesthetic Plast Surg. 1998 Nov/Dez;22(6):412-9.
14. Silva MMA, Resende VCL, Veiga DF, Brito MJ, Sabino Neto M, Ferreira LM. Impacto da mamoplastia redutora na sexualidade feminina. Rev Bras Cir Plást. 2013;28(Supl 1):1-103.
15. Santos GR, Araújo DC, Vasconcelos C, Chagas RA, Lopes GG, Setton L, et al. Impacto da mamoplastia estética na autoestima de mulheres de uma capital nordestina. Rev Bras Cir Plást. 2019;34(1):58-64.
16. Sanfelice AF. Mammary plastic arts planning: new classification of mammary shapes. ACM Arq Catarin Med. 2007 Jun;36(Supl 1):55-8.
17. Mansur JRB, Bozola AR. Mastopexy and breast augmentation with protection and inferior support of the prosthesis with inferior pedicle flap. Rev Bras Cir Plást. 2009;24(3):304-9.
1. Federal University of Pará, Belém, PA,
Brazil.
2. Plastic Surgery Clinic Dr. Wilson Cintra,
Jardim Paulista, São Paulo, SP, Brazil.
3. Heliópolis Hospital, Sacomã, São Paulo, SP,
Brazil.
GFMP Analysis and/or data interpretation, Conception and design study, Data Curation, Final manuscript approval, Investigation, Methodology, Project Administration, Realization of operations and/or trials, Writing - Original Draft Preparation, Writing - Review & Editing
Corresponding author: Giselly de Fátima Mendes Pascoal Rua Artur Sabóia, 328, Paraíso, São Paulo, SP, Brazil. Zip Code: 04104-060 E-mail: gisapascoal@yahoo.com.br
Article received: July 08, 2019.
Article accepted: July 15, 2020.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket