



Original Article - Year 2020 - Volume 35 -
Epidemiological study of burns at the Hospital of Clinics, Federal University of the Triângulo Mineiro
Estudo epidemiológico das queimaduras no Hospital de Clínicas da Universidade Federal do Triângulo Mineiro
ANDERSON JOSÉ GONÇALVES1 ; MARCO TULIO RODRIGUES DA CUNHA1,*; JOSÉ FERNANDES DOS SANTOS1
; MARCO TULIO RODRIGUES DA CUNHA1,*; JOSÉ FERNANDES DOS SANTOS1
ABSTRACT
Introduction: Burns are a serious public health problem.
Knowledge of the main epidemiological data of affected
patients is paramount for preventing and establishing the
best clinical treatment for these individuals. The objective
was to survey the epidemiological profile of burns, the main
mechanisms involved, treatments, and outcomes of these
cases at the Hospital de Clínicas da UFTM.
Methods: This is
a retrospective and cross-sectional study of hospitalizations
for burns at HC-UFTM from January 2015 to December
2019. Gender, age, depth of burns, location, etiology, use
of opioids, hospitalization duration, outcome (hospital
discharge or death), and extent of burned areas (EBA%).
Results: This study was composed of 138 patients, divided
into three groups: group 1 (G1), 39 patients; group 2 (G2),
89 participants, of which 5 died; and group 3 (G3), 10
participants, 4 of whom died. As for the trauma mechanism,
the most common was scald (17.39%), followed by thermal
burn (13.76%), alcohol (8.69%), and electric burns (5.79%).
Conclusion: There was a higher prevalence of second-degree
burns in male patients. The most prevalent mechanism of
trauma was scald, and the EBA had an average of 23.9%.
The face and neck were the most affected segments, and
61.59% of the patients required opioids during hospitalization.
Regarding the outcome, 91.30% of patients were discharged
from the hospital, and 6.52% died, with most cases in G2.
Keywords: Burns; Epidemiology; Plastic surgery; Public health systems; Multiple traumas.
RESUMO
Introdução: As queimaduras são um grave problema de saúde pública. O conhecimento dos principais dados epidemiológicos dos pacientes acometidos é de suma importância para a prevenção e instituição do melhor tratamento clínico a esses indivíduos. Objetivou-se realizar um levantamento sobre o perfil epidemiológico das queimaduras, os principais mecanismos envolvidos, tratamentos e desfechos destes casos no Hospital de Clínicas da UFTM.
Métodos: Trata-se de um estudo retrospectivo e transversal, das internações por queimadura no HC- UFTM, de janeiro de 2015 a dezembro de 2019. Foram avaliados: gênero, idade, profundidade das queimaduras, localização, etiologia, utilização de opioides, tempo de internação hospitalar, desfecho (alta hospitalar ou óbito) e extensão das áreas queimadas (SCQ%).
Resultados: Este estudo foi composto por 138 pacientes, divididos em 3 grupos: grupo 1 (G1), 39 pacientes; o grupo 2 (G2), 89 participantes, dos quais 5 foram a óbito; e o grupo 3 (G3), 10 participantes, sendo que 4 vieram a óbito. Quanto ao mecanismo do trauma, o mais comum foi por escaldadura (17,39%), seguida pela queimadura térmica (13,76%), pelo álcool (8,69%) e queimaduras elétricas (5,79%).
Conclusão: Houve uma maior prevalência de queimaduras de segundo grau em pacientes do gênero masculino. O mecanismo de trauma mais prevalente foi escaldadura e a SQC teve média de 23,9%. A face e o pescoço foram os segmentos mais acometidos e 61,59% dos pacientes necessitaram com uso de opioides na internação. Com relação ao desfecho, 91,30% dos pacientes receberam alta hospitalar e 6,52% vieram a óbito, com a maioria dos casos no G2.
Palavras-chave: Queimaduras; Epidemiologia; Cirurgia plástica; Sistemas públicos de saúde; Traumatismo múltiplo
INTRODUCTION
Burns have been considered a severe public health problem in Brazil and bring with them physical and psychological trauma, in large part, irreversible. Knowledge of epidemiological data is of great importance to providing subsidies for burn prevention and treatment programs and defining a parallel between the experiences of national and international centers1,2.
Burns, in their most diverse presentations, represent an aggravating factor in public health in Brazil. They cause diverse damage to patients, including physical and psychological, which in many cases can be irreversible or difficult to repair. Thus, knowledge of the main epidemiological data of affected patients is of paramount importance for the prevention and institution of the best clinical treatment for these individuals and helps define a parallel between the experiences of other specialized centers1,2.
In Brazil, it is estimated that there are around 1,000,000 accidents with burns per year. Some researches show that, among the cases of burns reported in the country, most are in children, being more common in boys up to two years of age3,4.
Statistical data on burn injuries in Brazil are scarce. However, these are important to understand the magnitude of the problem and identify the populations most affected and the circumstances in which burns occur so that prevention programs can be implemented5.
As in other areas, statistical data on burn injuries are challenging to obtain in Brazil, despite being essential for the proper assessment of the problem’s relevance5.
Thus, this study’s general objective was to survey data on hospitalizations made at the Hospital de Clínicas of the Federal University of Triângulo Mineiro (HC-UFTM), resulting from burns, in the last five years. The purpose is to understand and evaluate the demand for this type of care in the hospital’s plastic surgery service and characterize the epidemiology of burns in the Triângulo Sul.
OBJECTIVES
Specifically, it is a survey on the epidemiological profile of burns and the main mechanisms involved, treatments, and outcomes in patients treated by the plastic surgery service at Hospital de Clínicas da UFTM.
METHODS
This is a retrospective, cross-sectional study of patients hospitalized with burns, at Hospital de Clínicas da UFTM, from January 2015 to December 2019. After approval of the research by the research ethics committee of the Hospital de Clínicas da Federal University of Triângulo Mineiro, data were obtained under number 3,532,691. After obtaining the data, they were double-checked, with epidemiological data being evaluated, such as gender, age, depth of burns, location, etiology, date of occurrence of the burns, types of treatment performed (dressings, debridement, grafts, fasciotomies, etc.), use of opioid anesthetics during hospitalization, length of hospital stay, IDC recorded in care, outcome (hospital discharge or death) and extent of burned areas (EBA%). Descriptions of the burned areas and the “Lund-Browder” tables for adults and children were used to assess this data. Descriptions of the medical records’ burnt body surfaces were discarded for standardization of data, as these were not included in most of the evaluated medical records. The individuals participating in the research were divided into three groups, with “group 1” consisting of patients aged 0-18 years, “group 2” with patients aged 19-59 years, and “group 3” consisting of individuals over 60 years old.
A database was created with the information obtained from the patients’ medical records in GraphPad Prism 8.0.2.263® for statistical analysis. The results were expressed as number, percentage, average, and standard deviation, calculated among individuals in the same group, and the median applied exclusively to the length of hospital stay. Statistical analysis was performed using One-way ANOVA®, followed by the Brown-Forsythe and Welch’s test. The Wilcoxon Signed-Rank Test performed the distribution among individuals in the same group. Differences between individuals were considered significant when p <0.05.
RESULTS
In the analyzed period, 144 hospitalizations were identified, at HC-UFTM, with an international disease code (IDC) related to burns. Six patients were admitted to another specialty, with the IDC erroneously related, and were excluded from the study. Thus, this study is composed of 138 patients under the direct care of the plastic surgery discipline. Group 1 (G1) had 39 patients; group 2 (G2), 89 participants, of which five died; and group 3 (G3), 10 participants, 4 of whom died.
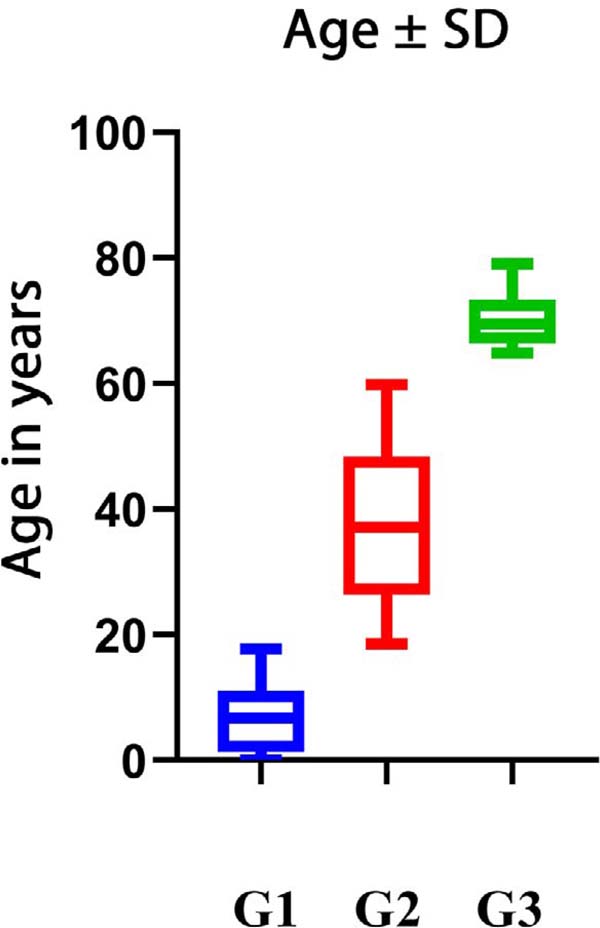
Our sample consisted of 89 male patients (64.50%) and 49 female patients (35.50%). The participants’ age had a general average of 32.63 years, [0.09-79.09 years]. Analyzing patients aged 0-18 years, the average age was 6.7 years, with a standard deviation (SD) of 5.46, while between 19 years and 59 years the average age was 37.15 years, with an SD of 11.85, and for patients over 60 years of age, the average was 69.45, with an SD of 4.75 (Figure 1). There was no significant difference between the three groups analyzed, with p = 0.9157, 0.8870, and 0.5114, respectively. There was a wide variety of IDC-10, with which patients were referred, at hospital discharge. 34 IDC-10 were described, and of these, T21.2, “second-degree burn of the trunk,” the most prevalent (8.69%).

As for the mechanism of trauma, the most common was scald (including all boiling liquids, such as water and oil), with 24 cases (17.39%), followed by a thermal burn, with 19 cases (13.76%), by alcohol, with 12 cases (8.69%), electric burns with 8 cases (5.79%), attempted self-extermination with 5 cases (3.62%), explosions with 4 cases (2.89%), fire indoors (1.44%), gasoline (1.44%), fire burns (1.44%) and chemical burns (1.44%). In 58 medical records (42.02%), there was no detailed description of the causal agent, which we consider an essential bias for this item in this study (Table 1).
| Mechanism | G1 | G2 | G3 | Total |
|---|---|---|---|---|
| Alcohol | 5 | 7 | - | 12 |
| Self-extermination | - | 4 | 1 | 5 |
| Electric | 1 | 6 | 1 | 8 |
| Scald | 16 | 8 | - | 24 |
| Explosion | 1 | 3 | - | 4 |
| Fire | 1 | 1 | - | 2 |
| Petrol | 1 | 1 | - | 2 |
| Indoor fire | 1 | 1 | - | 2 |
| Chemical | 1 | 1 | - | 2 |
| Thermal | 2 | 15 | 2 | 19 |
| Not described | 10 | 42 | 6 | 58 |
| Total | 39 | 89 | 10 | 138 |
Source: Medical records of UFTM Hospital de Clínicas, 2020.

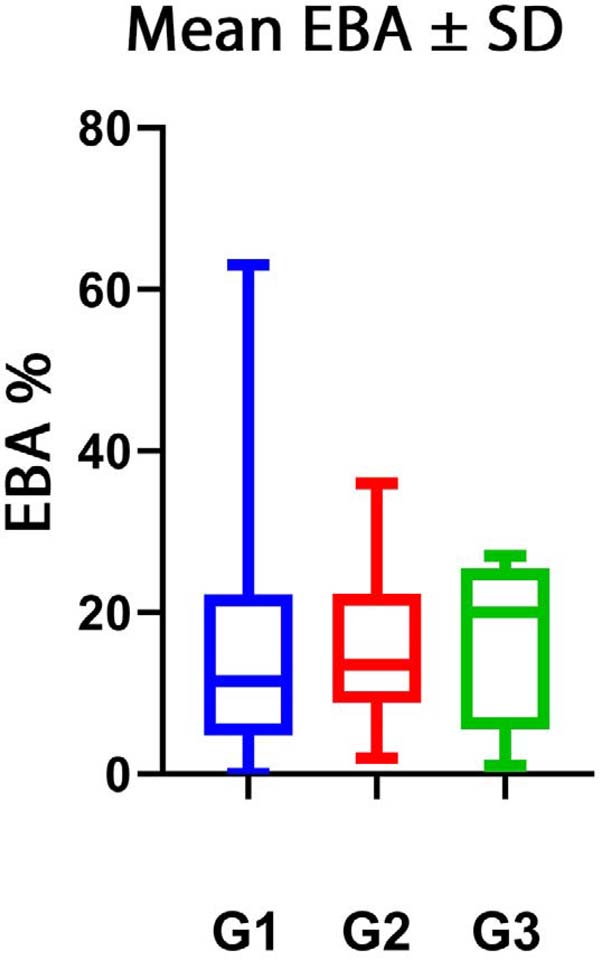
Regarding the burned body surface (EBA), 124 (89.85% of the sample) of the 138 medical records had descriptions, which enabled the EBA calculation. Thus, the mean EBA area was 15% [1-63% EBA] in group 1, while group 2 had an average of 19.17% [2-72% EBA] and group 3 had a mean of 17% [1-27% of EBA], as shown in Figure 2. Regarding the depth of burns were described in the medical records, 60.86% were 2nd degree, 31.88% 3rd degree, and 7, 26% of 1st degree. As for the use of opioid anesthetics, these drugs were used in 85 patients (61.59%), and their use was not necessary for 23 individuals (16.67%) and, in 30 patients, this information was not reported (21.74%).

As an outcome of the cases, 126 patients were discharged from the hospital with an “improved” diagnosis, with subsequent outpatient follow-up, corresponding to 91.30% of the patients, there were 9 cases of death (6.52%) and 3 cases (2.18 %) of evasion. All patients in group 1 (100%), 81 patients in group 2 (91.01%) and 6 patients in group 3 (60%) were discharged.
Of the patients analyzed, nine patients died after more than 24 hours of hospitalization, which corresponds to 6.52% of the total sample. Of these, most deaths occurred in the age group between 19 years and 59 years (55.55%), while the remainder (44.45%) was in elderly patients, and no deaths were observed in pediatric patients. Regarding hospital stay, the general median was six days; for group 1, it was three days, nine days for group 2, and 12.5 days for group 3. The most prolonged stay was in group 1, with 105 days.
As for the dressing applied to the patients, the most performed procedure was dressing with 1% silver sulfadiazine, associated with fibrinolytic ointment, with 41 cases (29.71%). Surgical debridement was performed in 27 cases (19.56%). Skin grafting was the third most performed procedure, with 26 cases (18.84%). After hospital discharge, there was a new hospitalization for three zetaplasties (2.17%), two amputations (1.44%), and the remaining cases (10.17%) were treated on an outpatient basis, with silver sulfadiazine dressing 1%. In 25 medical records (18.11%), there was no description of the conduct performed.
The body segments most affected by burns were also analyzed. The face was the most affected site, with 39 cases (11.07%), followed by burns on the right upper limb (MSD) with 33 cases (9.37%) and on the left lower limb (MSE) with 27 cases (7, 67%). The least affected burned areas were the lumbar regions and the knees, with only 1 case each (0.28%). The other affected sites are described in Table 2.
| Region | G1 | G2 | G3 | Total |
|---|---|---|---|---|
| Face | 11 | 25 | 3 | 39 |
| Right upper limb | 5 | 25 | 3 | 33 |
| Left upper limb | 5 | 22 | - | 27 |
| Right lower limb | 5 | 15 | - | 20 |
| Left lower limb | 4 | 18 | - | 22 |
| Abdomen | 2 | 13 | - | 15 |
| Chest | 3 | 11 | 3 | 17 |
| Left hand | 6 | 12 | - | 18 |
| Right hand | 4 | 12 | - | 16 |
| Airways | - | 10 | - | 10 |
| Thighs | 5 | 10 | - | 15 |
| Trunk | 7 | 6 | - | 13 |
| Arms | 6 | 4 | - | 10 |
| Genitals | 6 | 3 | - | 9 |
| Back | 1 | 7 | - | 8 |
| Neck | 1 | 6 | - | 7 |
| Forearm | 1 | 5 | - | 6 |
| Axillary | 4 | 1 | 1 | 6 |
| Right leg | 1 | 4 | - | 5 |
| Left leg | 2 | 3 | - | 5 |
| Gluteus | 2 | 3 | - | 5 |
| Right foot | 3 | 1 | - | 4 |
| Shoulders | 1 | 3 | - | 4 |
| Cervical | 2 | 2 | - | 4 |
| Left foot | 3 | - | - | 3 |
| Buttocks | 1 | 1 | - | 2 |
| Hips | - | 2 | - | 2 |
| Grips | 1 | 1 | - | 2 |
| Lumbar | 1 | - | - | 1 |
| Knee | - | 1 | - | 1 |
| Malar | 1 | - | - | 1 |
| Not described | 3 | 16 | 3 | 22 |
| Total | 97 | 242 | 13 | 352 |
Source: The authors, 2020.

DISCUSSION
This study aimed to evaluate the epidemiological profile of patients admitted to the Hospital de Clínicas, Universidade Federal do Triângulo Mineiro.
Some studies claim that the risk factors for burns can vary according to the location analyzed and life habits, such as alcohol and smoking6,7.
Part of the world literature8-11, on burns in children, includes children under seven years old. We included patients between 0 and 18 years of age12 in group 1, so our data can be correlated to these studies since this group’s average age was 6.7 years. In a study by Silva et al., in 201713, one of the major risk factors for burns in minors is access to the kitchen due to the family nucleus’s permissiveness and non-recognition environment as a place not safe. For these studies, burns represent the second most frequent cause of childhood accidents with a high degree of morbidity and mortality and organic dysfunctions, such as hypovolemic shock, progressive malnutrition, and infections. Besides, these individuals have burns in more than one body segment due to this age group’s inherent characteristics, such as curiosity and lack of knowledge, especially in male individuals8-11,14,15.
In all age groups, except patients older than 80 years, there are considerably more male patients than female patients, in agreement with the study carried out by Cruz et al. in 201216. The data of this study are according to other researches, in which there is a bimodal distribution of greater prevalence in the pediatric age group from 1 year to 15 years, comprising 23.5% of the total burns and the age group of adults from 20 years to 59 years, which represents 55% of burns, patients aged 60 years or more represented 15% of cases7.
Differences in burn mortality rates vary between different age groups and between genders. There is an increase in the number of burn deaths according to the age and extent of the burn and carbon monoxide and heated air inhalation injuries. Fire-related burns are the sixth leading cause of death among children aged 5 to 14 years and the eighth leading cause of death among people aged 15 to 29 years in low- and middle-income countries6,7.
Correctly obtaining information for epidemiological surveys is extremely important, as this information will serve as a basis to help understand the mechanisms involved and the construction of local burn prevention programs. They also help to improve hospital care. This information, as well as the patient’s pain level and the evaluation of the burn area tend to be miscalculated, even by specialists, and thus it is a challenge for the entire multidisciplinary team9,17-19.
Burns lead to metabolic, respiratory, cardiac, renal, and gastrointestinal changes that result in immunosuppression and can progress to septicemia. Emotional disorders affect their family, social, and work relationships, not only due to the countless physical deformities but also to the extended hospital stay often required. There was a 105-day hospitalization with several complications during this hospital stay; it was not addressed in this study because it was outside the scope of this research20-21.
In a study carried out by the American Burn Association, in 20177, regarding hospitalization, over ten years, from 2008 to 2017, the average length of hospital stays for women decreased from 9.4 days to 7.3 days, while for men it decreased less significantly from 9.5 to 8.5 days. In our series, the median days of hospital stay were six days, while the mortality rate for women decreased from 3.9% to 2.7% and from 3.4% to 2.6% in men, from January 2015 to December 2019.
In our study, the longer the hospital stay, the greater the depth of the burn. A retrospective, descriptive, and cross-sectional study with a quantitative approach, found similar results and states that mortality increases proportionally with the size of the burn22.
Scald burns were the most frequent causal agent in the medical records evaluated, in line with what is described in the literature10. They are also associated with high morbidity and mortality10. In our study, burns on the face and neck were the most frequent in 26.35% of cases. They require special care due to possible damage to the upper airways, ear cartilage, and eyes. There is also the possibility of scar microstomy, cervical contracture, and injury to the upper airways10,23.
Our study’s significant bias was the absence of a specific form for patients with burns and the filling in data by different resident physicians over time, sometimes with incomplete data. There was a need to standardize the burnt body surfaces’ calculation, based on the burnt areas’ descriptions, disregarding some calculations of the existing EBA, in part of the medical records. For this, the “Lund-Browder” table was used. Despite this, these data were able to better understand burns in the macro-region of the Triângulo Sul, improve the care provided by our service, and diagnose the need for a specific medical record institution for burned patients3,24,25.
CONCLUSION
There was a higher prevalence of second-degree burns and in male patients. The most-reported trauma mechanism was scald, and the burned body surface (EBA) averaged 23.9%. The face and neck were the most affected sites, and 61.59% of the patients required opioids during hospitalization.
REFERENCES
1. Aragão JA, Aragão MECS, Filgueira DM, Teixeira RMP, Reis FP. Epidemiologic study of burn injuries in children admitted to the Burn Unit of the Hospital de Urgência de Sergipe. Rev Bras Cir Plást. 2012;27(3):379-82.
2. Nigro MVAS, Maschietto SM, Damin R, Costa CS, Lobo GLA. Epidemiological profile of 0-18-year-old child victims of burnstreated at the Plastic Surgery and Burns Service of a University Hospital in Southern Brazil. Rev Bras Cir Plást. 2019;34(4):504-8.
3. Takejima ML, Netto RFB, Toebe BL, Andretta MA, Prestes MA, Takaki JL. Prevention of burns: evaluation of knowledge about prevention of burns in users of Curitiba health facilities. Rev Bras Queimaduras. 2011;10(3):85-8.
4. Barcelos RS, Santos IS, Matijasevich A, Barros AJD, Barros CF, França GVA, et al. Falls, cuts and burns in children 0-4 years of age: 2004 Pelotas (Brazil) birth cohort. Cad Saúde Pública. 2017;33(2):e00139115.
5. Rossi LA, Barruffini RP, Garcia TR, Chianca TC. Burns: characteristics of patients treated in a teaching hospital in Ribeirão Preto (São Paulo), Brazil. Rev Panam Salud Publica. 1998;4(6):401-4.
6. Mock C, Peden M, Hyder AA, Butchart A, Kruga E. Child injuries and violence: the new challenge for child health. Bull WHO. 2008;86(6):420.
7. American Burn Association (ABA). National Burn Repository 2017 Update. Report of data from 2008-2017. Dataset Version 13.0. Chicago: ABA; 2017.
8. Prata PHL, Flávio Júnior WF, Lemos ATO. Fluid resuscitation in the burned child. Rev Med Minas Gerais. 2010;20(4 Supl 3):S38-S43.
9. Fernandes FMFA, Torquato IMB, Dantas MSA, Pontes Júnior FA, Coutinho FA, Collet N. Burn injuries in children and adolescents: clinical and epidemiological characterization. Rev Gaúcha Enferm. 2012;33(4):133-41.
10. Barcellos LGB, Silva APP, Piva JP, Rech L, Brondani TG. Characteristics and outcome of burned children admitted to a pediatric intensive care unit. Rev Bras Ter Intensiva. 2018;30(3):333-7.
11. Santomé LM, Leal SMC, Mancia JR, Gomes AMF. Children hospitalized due to maltreatment in the ICU of a Public Health Service. Rev Bras Enferm. 2018;71(Suppl 3):1420-7.
12. Eisenstein E. Adolescência: definições, conceitos e critérios. Adolesc Saúde. 2005 Jun;2(2):6-7.
13. Silva SP, Sampaio J, Silva CT, Braga R. Child safety in preschool years: what do caregivers know?. Birth Growth Med J. 2017;26(4):221-6.
14. Bisceglia TS, Benatia LD, Faria RS, Boeira TR, Cidb FB, Gonsaga RAT. Profile of children and adolescents admitted to a Burn Care Unit in the countryside of the state of São Paulo. Rev Paul Pediatr. 2014;32(3):177-82.
15. Malta DC, Mascarenhas MDM, Silva MMA, Carvalho MGO, Barufaldi LA, Avanci JQ, et al. The occurrence of external causes in childhood in emergency care: epidemiological aspects, Brazil, 2014 Ciênc Saúde Coletiva. 2016;21(12):3729-44.
16. Cruz BF, Cordovil PBL, Batista KNM. Epidemiological profile of patients who suffered burns in Brazil: literature review. Rev Bras Queimaduras. 2012;11(4):246-50.
17. Hettiaratchy S, Papini R. ABC of burns: initial management of a major burn: II-assessment and resuscitation. BMJ. 2004;329(7457):101-3.
18. Castro RJA, Leal PC, Sakata RK. Pain management in burn patients. Rev Bras Anestesiol. 2013;63(1):149-58.
19. Soares J, Martin A, Arruda GO, Marcon SS, Barreto MS. Factors associated with level of pain in admission and high in victims of trauma. Enferm Glob. 2016;16(1):130-67.
20. Vale ECS. Inicial management of burns: approach by dermatologists. An Bras Dermatol. 2005;80(1):9-19.
21. Giordani AT, Sonobe HM, Guarini G, Stadler DV. Complications in burned patients: literature review. Rev Gest Saúde. 2016;7(2):535-48.
22. Nascimento LKA, Barreto JM, Costa ACSM. Variables analysis of the degree and size of the burn, length of hospital stay and occurrence of deaths in patients admitted in a Burn Care Unit. Rev Bras Queimaduras. 2013;12(4):256-9.
23. Teles GGA, Bastos JAV, Amary A, Rufatto LA, Ritty RS, Broglio LAP, et al. Treatment of superficial second degree burn of face and neck with topical heparin: a comparative, prospective and randomized study. Rev Bras Cir Plást. 2012;27(3):383-6.
24. Souza MT, Nogueira MC, Campos ESC. Care flows of moderate and severe burned patients in regions and health care networks of Minas Gerais. Cad Saúde Coletiva. 2018 Jul;26(3):327-35.
25. Arruda CN, Braide ASG, Nations M. "Raw and charred flesh": the experience of burned women in Northeast Brazil. Cad Saúde Pública. 2014;30(10):2057-67.
1. Federal University of the Triângulo Mineiro, Department of Surgery, Uberaba, MG,
Brazil.
AJG Analysis and/or data interpretation, Conception and design study, Conceptualization, Data Curation, Final manuscript approval, Formal Analysis, Investigation, Methodology, Project Administration, Realization of operations and/or trials, Writing - Original Draft Preparation, Writing - Review & Editing
MTRC Analysis and/or data interpretation, Conception and design study, Conceptualization, Data Curation, Final manuscript approval, Formal Analysis, Methodology, Supervision, Writing - Original Draft Preparation, Writing - Review & Editing
JFSJ Analysis and/or data interpretation, Final manuscript approval, Formal Analysis, Investigation, Realization of operations and/or trials, Writing - Original Draft Preparation, Writing - Review & Editing
Corresponding author: Marco Tulio Rodrigues da Cunha, Rua Vigário Carlos, 100, 4º Piso, Sala 423, Nossa Senhora da Abadia, Uberaba, MG, Brazil. Zip Code: 38025-350. E-mail: cunhamarco@hotmail.com
Article received: April 17, 2020.
Article accepted: July 15, 2020.
Conflicts of interest: none
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket