



Case Reports - Year 1998 - Volume 13 -
Free Radial Forearm Flap with Preservation of the Cephalic Vein in Head and Neck Reconstruction: Case Report
Retalho Livre Radial do Antebraço com Preservação de Veia Cefálica em Reconstrução Cérvico-Craniana: Relato de Caso
ABSTRACT
The authors present one case of microsurgical reconstruction of head and neck, in a patient with basal squamous cells carcinoma of the scalp invading the skull in which the adopted technique was that of a radial forearm flap, but with the preservation of the cephalic vein in nil its course. This surgical maneuver was elected because of a per-operatipe teelmical difficulty consisting in the absence of a suitable recipient vein of a previons radial cervical dissection. The radial forearm flap was transferred to the receiving bed in the head and neck region, where the microsurgical aunastomosis between the radial and facial arteries Was performerd, with no need of venous anastomosis since the cephalic vein was preserved.
Keywords: radial forearm flap; cephalic vein; head and neck reconstruction; microsurgery; Chinese flap.
RESUMO
Os autores apresentam um caso de reconstrução microcirúrgica Cérvico-Craniana, em paciente com carcinoma basoespinocelular de couro cabeludo invadindo o crânio, na qual se utilizou o retalho antebraquial radial com preservação da veia cefálica em todo o seu trajeto. Tal manobra cirúrgica deveu-se a dificuldade técnica no pré-operatório, caracterizada por leito venoso receptor inadequado, decorrente de esvaziamento cervical prévio. O retalho antebraquial radial foi transferido para a área receptora na região Cérvico-Craniana, onde foi feita a anastomose microcirúrgica da artéria radial com a artéria facial, sendo desnecessária a anastomose venosa devido a preservação da veia cefálica.
Palavras-chave: retalho livre antebraquial; veia cefálica; reconstrução de cabeça e pescoço; microcirurgia; retalho chinês
YANG, BOAQUI AND YUZHI(1) (1978) described the forearm the flap in China. SONG et al.(2) (1982) popularized its usc as a tree tlap tor thc reconstruction of head and neck. BEIMER & STOCK(3) (1983) used the same flap, with reverse pedicle, for hand reconstruction.
The radial forearm flap, also called Chinese flap, is based on the radial artery and on its fasciocutaneous pertorating branches.
Its territory may extend from the lower third of the anterior aspect of the arm till the wrist flexion crease.
Its distal width extends from the tendon of the pollicis longus to the tendon of the extensor carpi ulnaris and its proximal width extends from the lateral to the medial humeral epicondylus.
Planning comprises the drawing ofa line from a point 1 cm below the center of the antecubital fossa to the tubercle of the scaphoid. This line corresponds on the surface to the anarumieal course of the radial artery and of the anterolateral intermuscular septum, representing the vascular axis of the flap.
The dissection is carried out from the distal to the proximal portion, and from the ulnar to the radial side, including the deep fascia and preserving the fasciocutancous branches which emerge from the intermuscular septum.
On reviewing the literature we found one case reported by NAKAYAMA(5) (1986), in which the same procedure of preservation of the cephalic vein was used, because of the lack of an adequate venous receiving bed. In such circumstances, venous grafts can be used to make the connection with receiving bed blood vessels.
It must be noticed, however, that long venous grafts are critical and exposed to thrombosis.
CASE REPORT
Male, 37 years old, white, arrived in our service In August, 1994, with a history of having already been submitted to 4 operations for exeresis of recurrent scalp tumor in the vertex region. In the latest operation, a local flap was used for reconstruction, and a drain was placed through a stab wound in the left mastoid area.
The patient developed tumoral recurrence on the scalp together with a new lesion in the left postauricular region, that we thought it could be a tumor seeding along the drain course.
On August, 1994, he underwent resection of the scalp lesion, as well as the excision of a portion of the underlying skull. The histopathologic examination detected a basal squamous cells carci noma wi th bone infiltration, and the specimen had free surgical margins.
The same operation also comprised the resection of the left postauricular tumoral lesion adherent to the mastoid process, and the histopathologic finding was basal squamous cells carcinoma removed with free surgical margins.
On December 18, 1994, the patient returned with a recurrence of the left postauricular tumor on the superior portion of the surgical scar, and the necessary excision was performed.
On March 9, 1996, the patient was reviewed, and detected a recurrence of the cutaneous lesions on the scalp, both in the left postauricular and in the temporal regions. On March 12, 1996, he underwent the excision of those lesions as well as a radical posrerolateral cervical dissection, ineluding the jugular vein, the external jugular vein, and the sternocleidomastoid and omohyoid museles. Acraniectomy was performed in the temporal region. The bare area was covered at first with advanced flaps from within this region and with split skin graft taken fium the left thigh. The histopathologic examination indicated the presence of invasive basal squanlous cells carcinoma affecting skin, subcutaneous tissue, subjacent muscle and bone tissue, as well as free surgical margins and the absence of metastasis in 14 studied lymph nodes.
On March 14, 1996, in a second stage of the operation, the patient was submitted to reconstruction with a microsurgical free radial forearm flap. Because of the absence of a suitable receiving venous bed for microsurgical anastomosis, the dissection of the cephalic vein was carried out till its point of union with the subelavia vein. The Chinese flap was so transposed to the head region through a subecutaneous tunnel undermined at the supraelavieular area. The anastomosis between the radial and facial arteries was performed in the receiving bed. The forearm donor area was covered with a split skin graft also taken from the left thigh.
The postoperative period was uneventful and the patient underwent temporal and cervical radiotherapy.
RESULTS
The last elinical control took place on July, 1997. No recurrence was found, and the patient was in good health.
DISCUSSION
The Chinese flap is well known and largely used in microsurgical reconstruction.
In the reported case, the venous receiving bed was critical due to a prior cervical radical dissection. The use of a venous graft that could have been used would also entail a high degree of danger, since long grafts are prone to thrombosis.
We favored the preservation of the cephalic vein, which was dissected all along its course till the outlet into the subelavia vein, so that the venous anastomosis for the drainage of the graft resulted unnecessary. We thought this approach to be original, but on reviewing the specific literature we fell across one similar case reported by NAKAYAMA(5).
CONCLUSION
In patients needing microsurgical head and neck reconstruction but lacking a suitable venous recipient bed, we think the forearm free flap with preservation of the cephalic vein is both feasible and efficient.

Fig. 1 - Craniectomy and radical cervical dissection were performed. The dura mater was tcmporarily covered by a split skin graft.
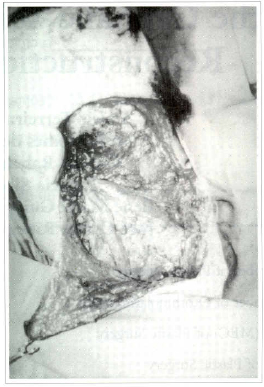
Fig. 2 - Defect of the skull after removing of the skin graft and elevation of the radical cervical dissection flap.
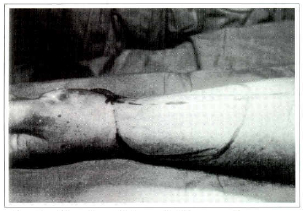
Fig. 3 - Planning of the radial forearm flap.
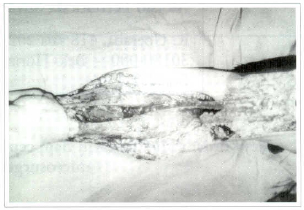
Fig. 4 - Elevation of the Chinese flap and dissection of the venous pedicle.
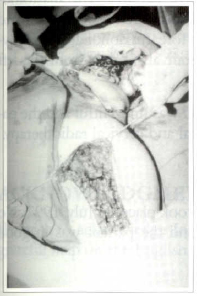
Fig. 5 - Transposition of the flap under a subcutaneous tunnel at the supraclavicular region, preserving the cephalic vein.

Fig. 6 - Anastomosis between the radial and facial arteries.
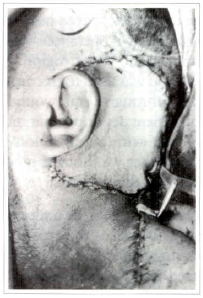
Fig. 7 . Operation completed; good perfusion of the flap.
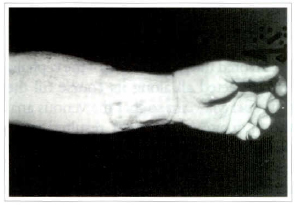
Fig. 8 - Donor area; late result.
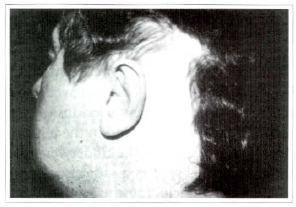
Fig. 9 - Radial antebraquial flap ar the head and neck region; late result.
REFERENCES
1. YANG G, BOAQUI C, YUZHI G. Free Forearm Skin Transplantation. Natl. Med. j. China. 1981;61:139.
2. SONG R, GAO Y, SONG Yet al. The Forearm Flap. Chin. Plast. Surg. 1982;9:21.
3. BEIMER E, STOCK W Toral Thumb Reconstruction: A One Stage Reconstruction Using an Osteocutaneous Forearm Flap. Br. j. Plast. Surg. 1983;36:52.
4. STRAUCH B, YU HL, CHEN ZW, LIEBLING R. Atlas of Microvascular Surgery; Anatomy and Operative Approaches. Thieme Medical Publishers, New York, 1993;49-52.
5. NAKAYAMA Y, SOEDA S, IINO T. A Radial Forearm Flap Based on an Extended Dissection of the Cephalic Vein: The Longest Venous Pedicle' Br. J. Palst. Surg. 1986;39:454-457.
ACKNOWLEDGMENTS
We wish to acknowledge Jorge affonso Ribeiro de Rezende Alves for his gratefu1 help on the English manuscript.
I - Sraff member of Plastic Surgery
II - Starr member of Otorhinolaringology
III - Resident (MEC) of Plastic Surgery
IV - Resident of Plastic Surgery
V - Chief of the Second Clinic of Plastic Surgery
Address for Correspondence:
Aloisio Ferreira da Silva Filho, MD
R. Uberaba, 418 sala 202
30180-080 - Belo Horizonte - MG - Brazil
From the Second Clinic of Plastic Surgery Felieio Roeho Hospital - Belo Horizonte - Brazil
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket