



Original Article - Year 2021 - Volume 36 -
Profile of patients hospitalized in a burn treatment center in northern Paraná
Perfil de pacientes internados em um centro de tratamento de queimados do norte do Paraná
Flávia Mendonça da Silva Oussaki1,* ; Lilian Denise Mai1; Mariana Sbeghen Menegatti2
; Lilian Denise Mai1; Mariana Sbeghen Menegatti2
ABSTRACT
Introduction: Burns are injuries arising from heat and represent a serious public health problem in the world due to physical or psychological sequelae of permanent character, and require specialized investment and quality. The objective is to know the profile of patients hospitalized in a burn treatment center in northern Paraná in 2012.
Methods: Retrospective, descriptive and quantitative analysis research, conducted in 2013, with data collected from 241 clinical records of patients treated at a burn treatment center in northern Paraná in 2012. Analyses of percentage and incidence of cases were performed.
Results: Readmission was present in 8% of the cases,70% of them were men, and 59% were adults; the patients had as their origin the patients originated from the regional health center in 44% of cases in 44% of the cases; the time to hospital stay was equal to or greater than three days in 38% of the cases and the mean length of stay was 17 days. Accidents in the domestic environment stood out in 75.5%; were the main causal agents of liquid alcohol: 32%, followed by scalding: 31%; the parts of the body most affected were face, upper limbs, trunk and lower limbs. There was death in 14%, reaching 44% of the elderly attended.
Conclusion: Burns is a problem that affects both sexes and different age groups, triggering physical, emotional and socioeconomic consequences. These injuries are a challenge for public policies and the health system, requiring investments in specialized services and treatments, in addition to prevention strategies.
Keywords: Burns; Burn units; Health profile; Hospitalization; Inpatients.
RESUMO
Introdução: Queimaduras são lesões decorrentes da ação do calor e representam um grave problema de saúde pública no mundo devido às sequelas físicas ou psicológicas de caráter permanente, e exigem investimento especializado e de qualidade. O objetivo é conhecer o perfil de pacientes internados em um centro de tratamento de queimados do norte do Paraná no ano de 2012.
Métodos: Pesquisa retrospectiva, descritiva e de análise quantitativa, realizada no ano de 2013, com dados coletados em 241 prontuários clínicos de pacientes atendidos em um centro de tratamentos de queimados do norte do Paraná em 2012. Foram realizadas análises de percentual e incidência dos casos.
Resultados: Reinternações estiveram presentes em 8% dos casos, 70% dos foram homens e 59% eram adultos; os pacientes tinham como origem a regional de saúde local em 44% dos casos; o tempo para internação foi igual ou maior que 3 dias em 38% dos casos e o tempo médio de permanência foi de 17 dias. Destacaram-se acidentes em ambiente doméstico em 75,5%; foram os principais agentes causais o álcool líquido: 32%, seguido por escaldo: 31%; as partes do corpo mais atingidas foram face, membros superiores, tronco e membros inferiores. Houve óbito em 14%, chegando a 44% dos idosos atendidos.
Conclusão: Queimaduras são um problema que acomete ambos os sexos e diferentes faixas etárias, desencadeando consequências físicas, emocionais e socioeconômicas. Estas lesões são um desafio para as políticas públicas e para o sistema de saúde, exigindo investimentos em serviços e tratamentos especializados, além das estratégias de prevenção.
Palavras-chave: Queimaduras; Unidades de queimados; Perfil de saúde; Hospitalização; Pacientes internados
INTRODUCTION
Burns are tissue lesions resulting from heat, directly or indirectly, destroying the skin, its annexes, muscles and tendons1. They represent a serious public health problem in the world due to physical or psychological sequelae of a permanent nature2.
The Ministry of Health estimates that approximately one million people suffer burns annually, with a higher prevalence in individuals with lesser economic circumstances, highlighting socio-cultural and environmental influences on the etiology of burns3. If efforts are perceived to identify risk factors and conditions that favor burns, the data show high incidence values and significant mortality rates2.
The Unified Health System (SUS), Ordinance GM/MS No. 1273, of 21 November 2000, organized the care of patients with burns in hierarchical and regionalized services, the burn treatment centers (BTC), which were implemented in the country and are a reference in the network. The state of Paraná has three BTCs in different regions, two of them are active. The BTC attend 3rd-degree burns in more than 10% of the burned body surface (BBS); adults over 20% of BBS and children over 10% of BBS; burns on the face, hands and feet, perineum, airways or circumferential; electrical or chemical; with trauma or associated systemic diseases; and the impossibility of oral hydration4. Patients with these conditions wait in general hospitals for specialized care, subject to the availability of a vacancy in BTC. Although health is a constitutional right, the structuring of the service network in the care of the burned still encounters legal or financial obstacles5.
The production of data on burns’ profile over the years provides greater knowledge of the etiology of cases and the delineation of the epidemiological profile of care. Identifying risk groups and behaviors can contribute to educational and prevention campaigns and highlight the impact of the service on the health network and provide greater knowledge for its structuring.
OBJECTIVE
To know the profile of patients hospitalized in a burn treatment center in northern Paraná in 2012.
METHODS
This is a retrospective, descriptive study of quantitative analysis, which aims to know the profile of hospitalized patients burned in a BTC in northern Paraná in 2012. It was inclusion criteria for the patient to have been hospitalized in the BTC during 2012. Exclusion criteria were that the patient did not have burns as the primary cause of hospitalization and the date of burn before 2012.
A total of 312 medical records of patients hospitalized in the period were collected, and after applying the exclusion criteria, the sample totaled 241 medical records. Cases with hospitalization and readmission in 2012 were counted only once.
Of the variables investigated, the following are presented in this article: age, gender, city of origin, source of burn and BBS. The data were organized in a spreadsheet, and analyses of percentage and incidence were performed.
The ethics committee approved the study on research involving human beings of the State University of Maringá, CAAE no. 11590313.8.0000.0104, of 27 February 2013. Considering that the sources were medical records, the free and informed consent form was waived, and the researcher signed the confidentiality and confidentiality term.
RESULTS
Two hundred forty-one medical records were analyzed. The epidemiological profile of the inmates was 70% (169) male. Adults (18 to 59 years old) predominated in 59% (143) of the cases, followed by children (up to 11 years old) in 30% (72), elderly (over 60 years old) in 7% (16) and adolescents (12 to 17 years) by 4% (10). Among the total medical records analyzed, 8% (20) went through one to three readmission episodes. The readmission rate in males was 8% (13) and in females 10% (7). Regarding the age group, there were 10% (1) in adolescents, 6% (9) in adults and 14% (10) in children; there was no readmission of the elderly this year. Concerning BBS, 80% (16) of those readmitted had up to 10% of body surface affected, third-degree burn in 50% (10) and scalding causal agent in 35% (7). As for the origin of the patients, it was observed that the service absorbed the demand from 18 different health regions (HR) in Paraná. The highest concentration was in the northern, northwest and western regions, with 44% (106) of the 17th HR, which includes the municipality where the service is located, 9% (21) of the 15th HR, 7% (17) of the 20th HR and 7% (17) of the 11th HR. Specifically, on the 17th HR, the origin of 65% (69) of the patients was from the city where the BTC was located, of the 106 patients of the 17th HR, 62% (66) were affected by 2nd-degree burns, and 73% (77) had up to 10% of the BBS.
About the interval between accident occurrence and hospitalization in the BTC, 26% (63) were hospitalized on the same day that the burn occurred, 21% (51) one day later, 15% (35) two days later and 38% (92) three days or more. Among the total, 40% (97) underwent hospitalization in intensive care bed, with an average stay of eight days. The mean length of stay of patients in this BTC was seventeen days.
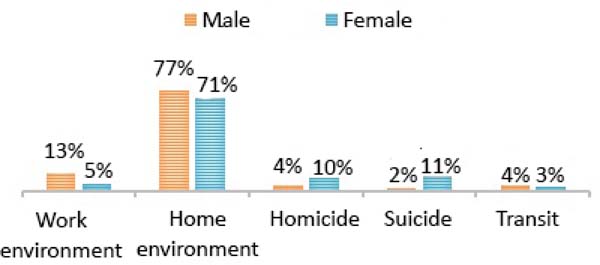
Regarding the nature of the accident, there was a predominance of 75.5% (182) in the domestic environment, followed by work environment 11% (26), homicides 6% (14), suicide 4.5% (11) and traffic 3% (8). Figure 1 shows the nature of the accident according to gender.

Among male victims, there was an increase in burns in July and December, reaching 12% (21) and 13% (22) of the entire year, respectively, with alcohol’s causal agent. It is noteworthy that in December, the causal agent liquid alcohol was responsible for 41% (9) of burns in men. Work accidents reached 13% (22) of men, with electricity being the main cause in 50%.
In female patients, the highest percentage of cases was concentrated in November with 15% (11), April with 12% (9) and December with 10% (7). As for the causal agents, the scald corresponded to 47% (34) and alcohol to 28% (20).
Table 1 shows the prevalence of accidents according to age group and causal agent. A higher percentage of burns with causal agent liquid alcohol (32%) is visualized, followed by scalding (31%). Scalding burn numbers are also highlighted in children (57%) and alcohol in adolescents (40%), and adults (41%).
| Alcohol | Flame | Energia elétrica | Electricity | Clothes iron | Gasoline | Others | |
|---|---|---|---|---|---|---|---|
| Child | 12% (9) | 9% (6) | * | 57% (41) | 7% (5) | 1% (1) | 14% (10) |
| Adolescent | 40% (4) | 10% (1) | 20% (2) | 30% (3) | |||
| Adult | 41% (59) | 10% (14) | 8% (12) | 20% (28) | 4% (6) | 17% (24) | |
| Elderly | 25% (4) | 25% (4) | 6% (1) | 25% (4) | 19% (3) | ||
| Total | 32% (76) | 10% (25) | 5% (13) | 31% (75) | 2% (5) | 4% (10) | 16% (37) |
Source: The authors, 2020.
* Remained blank where the number of cases by a given causal agent was zero.

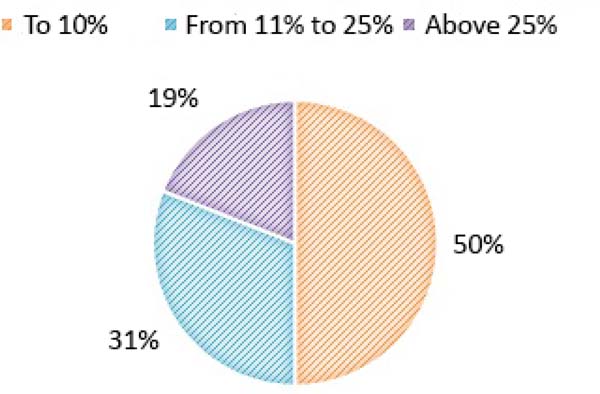
Regarding the degree of burn, 51% (123) of the hospitalized patients had second-degree burns and 49% (118) of the 3rd degree. The analysis of BBS is presented in Figure 2.

Among the most affected body parts were 48% (116), upper limbs 68% (164), trunk 41% (99) and lower limbs 37% (89). Face burn was present in all age groups, being 43% (31) in children, 60% (6) in adolescents, 56% (9) in the elderly and 49% (70) in adults.
Among the 241 patients, 14% (33) died, 11% (18) male and 21% female. Among women who died, the nature of the accident was a homicide in 33% (5) and suicide in 40% (6). Among men who died, 78% (14) suffered burns in the domestic environment.
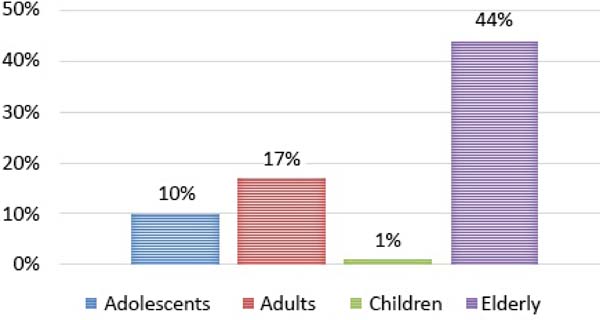
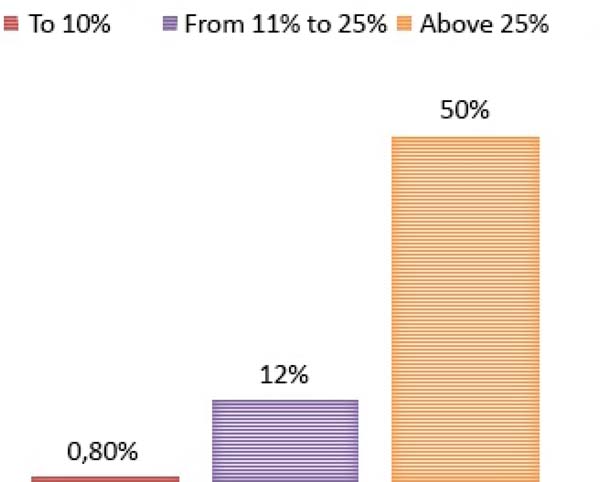
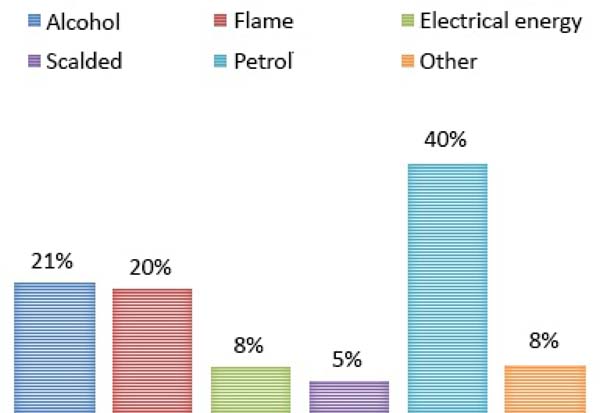
Figure 3 shows the occurrence of death by age group of patients, Figure 4 shows the occurrence of death from BBS, and Figure 5 shows the percentage of deaths by type of causal agent of the burn.
DISCUSSION
It is important to highlight the number of necessary readmissions; about 8% in 2012, 50% were affected by third-degree burns. The need for long-term care requires multidisciplinary and interdisciplinary action, requiring constant investments and improvements; otherwise, the effectiveness and efficiency of the treatment are compromised in the face of precariousness and access difficulties for some patients.
Regarding the epidemiological profile, 70% (169) were male, similar to that found in national and international studies, and specialized services in the country presented percentages of 61%6 and 69.5%7. In an international study, the percentage of men reached 73%8. Less cautious behavior, aggressive attitudes and games, in addition to greater occupational exposure to risk, can make men more vulnerable. Individuals of adulthood correspond to the economically active population and with greater performance in dangerous activities, so young construction workers are among the populations at higher risk7. The findings show that 13% of burns in men are work accidents, being the main cause of electricity.
There was a predominance of hospitalizations of adult patients, followed by children. This differs from a study conducted in Nepal in which children between one and four years of age represented the highest number of admissions to the service9.
The origin of the patients was not restricted to the HR where the service is located; about 56% of the cases were from other HR, which indicates the importance of this service as a reference in care. The state of Paraná has only one more BTC in operation. In the eastern region, no other specialized services with a similar purpose entered into activity in the years after this research was carried out.
Regarding the 17th HR, 62% of patients were affected by 2nd-degree burns, and 73% had up to 10% of BBS, which goes against the findings in an Australian emergency service where most of the patients had low burn severity8.
It was found that in 38% of the cases treated, there was a time equal to or greater than three days after the burn to enter the service and that only 26% occurred on the same day. Such delay represents a greater compromise in the effectiveness of assistance to major burns since the prognosis is directly related to the type of care and the moment it is provided, negatively affecting recovery10.
Among the total patients, 40% underwent hospitalization in intensive care bed, with an average stay of eight days. In a study conducted in 2018, the percentage of patients with ICU stay reached up to 50%, with a mean hospitalization of 14.7 days6.
The average stay was 17 days, less than in a burn unit in Goiânia, 23 days6; however, significantly longer than in a reference center in Pará with a maximum of 7 days7. The length of hospital stay can be related to different factors, such as the quality and efficiency of the assistance provided, but also to the complexity of the burn; the shorter it is, the shorter the stay will require. By associating the variables sex and nature of the accident shown in Figure 1, significant aspects are revealed that reinforce social, behavioral differences and risk groups for the occurrence of burns. In the male sex, accidents in the home and work environment stood out, with 6% and 8% more than in women, respectively. Occupational exposure coincides with the predominance of adulthood in 59% of cases, followed by children, the elderly and adolescents, which is similar to those of another study. The elderly were the least affected when compared to the adult population11. However, the population aged over 60 years has a progressively higher mortality rate6,9, in this study reaching 44%, as shown in Figure 3.
The individual analysis by sex showed increases in the numbers that differed between months, and men had a higher number of accidents in December (13%), with causal agent alcohol (41%), reflecting on the use of these products in parties and common fraternizations at this time of year. In females, the cases did not have concentrations in the coming months, presenting mostly in November; however, the causal agent of women differed from that found in men, with scalding accounting for 47% and alcohol by 28%.
In the burns that occurred in the female sex, it is necessary to watch for cases of suicide attempt (11%) and homicide (10%), being the only cases in which the nature of accidents was higher in women than men, as seen in Figure 1. In agreement with the findings presented here, a study conducted in 2018 indicates that men are burned more in the work and domestic environment, while women are burned more by self-injury. In addition, the burn in women was also related to domestic violence12.
As for the causal agent, Table 1 presents liquid and scalded alcohol as the main causative agents in all cases; however, alcohol is among adolescents (40%) and adults (41%). Liquid alcohol is pointed out as one of the main sources of burn6. Even when it does not cause death, alcohol is significantly presented as a causal agent. This product is used customarily and indiscriminately in homes, both in daily cleaning and leisure time. To restrict access to the product, the incidence and severity of burns, on 29 January 2013, a new determination prohibiting the marketing of liquid alcohol with content greater than 54° GL13 entered into force.
Table 1 also highlights the data on burns in children and the elderly, and in children, the scalded (57%) was involved in a greater number of occurrences, mostly domestic. Scalding is one of the main etiological agents of burns in the infant population, reaching 51% of visits9. The occurrences in children aged between one and five years are associated with the moment when they are no longer totally dependent on the adult and start to experience and explore the extra-home environment14.
In the elderly, accidents with alcohol, flames, and scalding had the same incidence between cases, totaling 75%. In a 2019 survey, the causes of burns were alcohol and electricity, in first and second place, respectively15, in a survey carried out in Nepal, the main cause of burns was flames9, this research did not mention the use of alcohol in the environment domestic market, which signals once again the cultural character of the consumption of this product in our country.
It is noticeable in Figure 2 that hospitalizations according to body extension for patients with up to 10% BBS was equal to the sum of patients with BBS of 11% to 25% and above 25%. These findings are similar to a study that found a prevalence of small-scale lesions16. This does not represent a lower severity in cases since the degree of burn, and the patient’s general health conditions should also be evaluated.
The numbers of patients with 2nd and 3rd-degree burns were close, 51% and 49%, respectively, differing from research that presented 45% of 2nd degree and 6% of 3rd degree, respectively, indicating greater severity care at BTC in the study. However, it is also important to consider the organization of the service and the possibility that many patients with 1st-degree burns may have outpatient care and not enter the group of inpatients considered in the research.
Among the most affected parts of the body were the face, upper limbs, trunk and lower limbs, the first two being the most affected. Burning in the face region can be difficult to accept as the disfigurement of a completely visible body area can have a social and psychological impact. Considering the high incidences and challenging consequences, it is necessary to closely examine the BTC teams for multi-professional support in the rehabilitation period and return to daily life activities.
The total number of deaths was 14%, higher than in studies that presented percentages ranging from 6%7 to 11%6. Women had a higher percentage of death than men, reaching 10% more and had 73% of burns related to homicide and suicide; these numbers become even more alarming when we observed that deaths among men were related to domestic occurrences in 78% cases.
Suicide is related to life history, fragility in interpersonal relationships, individual difficulties, psychological distress and mental disorders12. Despite advances in available treatments, burn mortality derived from homicide and suicide becomes a significant indicator of social and human impact and denounces the physical and psychological violence to which women are subjected, reiterated by another Brazilian study12.
Figure 3 shows the occurrence of death by age group, highlighting a higher occurrence among the elderly, followed by adults, adolescents and children, in decreasing order, which may be related to the general conditions of individuals who favor recovery, with the time of care, severity of injuries and their complications 6.
Figure 4 shows the percentage of deaths according to the BBS of the patients, and the highest percentage of deaths was among individuals who had more than 25% of BBS, reaching 50% of the total. Extensive burns, which reach a large body proportion, trigger successive anatomical and physiological changes, which require high complexity care, mainly related to complications for body homeostasis, hydro electrolytic disorders and imbalance in the barrier of protection against infections. A study conducted in a reference hospital for burns contacted a strong correlation between the occurrence of deaths and the classification of BBS, and all patients who died in the service had previously been considered large burns11.
When analyzing Figure 5, which presents the percentage of deaths according to the type of causal agent of the burn, it was observed that there was a higher number of deaths among patients who suffered burns caused by gasoline, with a percentage that reached 40% of patients. The percentage of deaths in patients with burns from alcohol and flames reached 21% and 20%, respectively. It is important to highlight the dangerousness of flammable liquids such as gasoline and alcohol and the severity of burns they can cause, including the fact that both spread easily across the body surface, increasing the affected area.
The data of this research have similarities and divergences with previously published studies6-8,11,12, constituting an important analysis of the profile of the patients and their origin, as well as of the regional representativeness that the BTC has, which can contribute to the planning, quality and improvement these services in different places. The public policy of care for burns at the national level represents an important advance in the aspects of prevention and quality of care; however, the survey of data on hospitalizations in a BTC allowed highlighting important aspects, such as occurrences that could be prevented. The study’s limitations were the annual cut performed that restrict the collection to a single year and the descriptive character without robust data analysis. However, it contributes to the objective analysis of the findings that can be compared with previous and subsequent studies, carried out in this BTC or in other institutions in the country, to outline a long-term profile of patients and establish policies for the prevention and control of burns, resulting in a higher quality of care and cost containment17.
CONCLUSION
The findings showed a predominance of burns in adults (59%), males (70%), in a domestic environment (75.5%), with the most affected parts of the face, upper limbs, trunk and lower limbs. Regarding the burn degree, it was identified that 51% of the patients had 2nd-degree burns and 49% of the 3rd-degree, and concerning the affected body extension, 50% had up to 10% of BBS. The analysis showed significant numbers of deaths among older people who suffered burns (44%) and deaths of women who had burns related to cases of suicide (40%) and homicide (33%). It is concluded that burns affect both sexes and different age groups, with specificities related to the causal agent and nature of the accident. Burn injuries are a challenge for public policies and the health system, which requires investments in specialized services and treatments such as those offered at BTC and the fundamental prevention strategies for preventing health problems in the population.
REFERENCES
1. Souza MCA, Oliveira LCF. Fatores de risco de queimaduras domésticas: conhecimento de profissionais de Unidades Estratégia Saúde da Família. Rev Saúde. 2019;10(1):9-14.
2. Júnior EML, Melo MCA, Alves CC, Alves EP, Parente EA, Ferreira GE. Avaliação do conhecimento e promoção da conscientização acerca da prevenção de queimaduras na população de Fortaleza-CE. Rev Bras Queimaduras. 2014;13(3):161-7.
3. Ministério da Saúde (BR). Um milhão de brasileiros sofre queimaduras por ano [Internet]. Brasília (DF): Ministério da Saúde; 2017; [acesso em 2019 Out 12]. Disponível em: http://www.brasil.gov.br/editoria/saude/2017/06/um-milhao-de-brasileiros-sofrem-queimaduras-por-ano
4. Ministério da Saúde (BR). Portaria GM/MS nº 1.273, de 21 de novembro de 2000. Cria mecanismos para a organização e implantação de redes estaduais de assistência a queimados [Internet]. Brasília (DF): Ministério da Saúde; 2000. Disponível em: http://dtr2001.saude.gov.br/sas/PORTARIAS/PORT2000/GM/GM-1273.htm
5. Magalhães R. Governança, redes sociais e promoção da saúde: reconfigurando práticas e institucionalidades. Ciênc Saúde Coletiva. 2018 Out;23(10):3143-50.
6. Arruda FCF, Castro BCO, Medeiros JF, Valadão WJ, Reis GMD. Análise epidemiológica de 2 anos na Unidade de Queimados do Hospital de Urgências Governador Otávio Lage de Siqueira, Goiânia, Brasil. Rev Bras Cir Plást. 2018;33(3):389-94.
7. Silva JAC, Lima AVM, Borborema CLP, Cunha LM, Martins MM, Pantoja MS. Perfil dos pacientes queimados atendidos em um centro de referência na região metropolitana de Belém do Pará. Rev Bras Queimaduras. 2016;15(3):153-7.
8. Knol R, Kelly E, Paul E, Cleland H, Wellington-Boyd A, Lambert C, et al. The psychosocial complexities of acute burn patients in an Australian trauma hospital. Burns. 2019 Ago;46(2):447-53.
9. Wardhana A, Basuki A, Prameswara ADH, Rizkita DN, Andarie AA, Canintika AF. The epidemiology of burns in Indonesia's national referral burn center from 2013 to 2015. Burns Open. 2017 Out;1(2):67-73.
10. Valente TM, Nascimento MFA, Silva Júnior FR, Souza JPF, Martins CB, Valente TM, et al. Importância de um atendimento pré-hospitalar efetivo a adultos vítimas de queimaduras: uma revisão integrativa. Rev Bras Queimaduras. 2018;17(1):50-5.
11. Silva JAC, Lima AVM, Borborema CPL, Cunha LM, Martins MM. Perfil dos pacientes atendidos por queimaduras em um hospital de referência no norte do Brasil. Rev Bras Queimaduras. 2015;14(3):198-202.
12. Salomoni SS, Massa LDB. Mulheres queimadas: uma revisão integrativa de publicações nacionais. Rev Bras Queimaduras. 2017;16(1):34-44.
13. Ministério da Saúde (BR). Agência Nacional de Vigilância Sanitária (ANVISA). Restrição ao álcool líquido de maior potencial inflamável está em vigor [Internet]. Brasília (DF): Ministério da Saúde/ANVISA; 2013. Disponível em: http://portal.anvisa.gov.br/wps/content/anvisa+portal/anvisa/sala+de+imprensa/menu++noticias+anos/2013+noticias/restricao+ao+alcool+liquido+de+maior+potencial+inflamavel+esta +em+vigor
14. Amaral ILPS, Rodrigues APSB, Magalhães VMPC, Rocha SWS. Perfil das internações de crianças vítimas de queimaduras em um hospital público de Recife. Enf Brasil. 2019 Fev;17(6):662-9.
15. Simaan IF, Botelho JLS, Ferreira PEN, Pinheiro DMS. Perfil epidemiológico dos pacientes queimados atendidos no hospital geral público de palmas, no período 2010/2017. Rev Patol Tocantins. 2019;6(1):12-7.
16. Aiquoc KM, Dantas DV, Dantas RAN, Costa IB, Oliveira SP, Lima KRB, et al. Avaliação da satisfação com a imagem corporal dos pacientes queimados. Rev Enferm UFPE Online. 2019 Abr;13(4):952-9.
17. Ahmadi M, Madani T, Alipour J. Development a national minimum data set (MDS) of the information management system for disability in Iran. Disabil Health J. 2019 Out;12(4):641-8.
1. State University of Maringá, Nursing, Maringá, PR, Brazil.
2. University of São Paulo, School of Nursing, São Paulo, SP, Brazil.
Corresponding author: Flávia Mendonça da Silva Oussaki, Avenida Robert Koch, 60, Operária, Londrina, PR, Brazil. Zip Code: 86038-350 E-mail: flaviaou@gmail.com
Article received: July 06, 2020.
Article accepted: April 23, 2021.
Conflicts of interest: none
COLLABORATIONS
FMSO Analysis and/or data interpretation, Conception and design study, Conceptualization, Data Curation, Final manuscript approval, Formal Analysis, Investigation, Methodology, Project Administration, Resources, Writing - Original Draft Preparation, Writing - Review & Editing
LDM Analysis and/or data interpretation, Conception and design study, Conceptualization, Data Curation, Final manuscript approval, Formal Analysis, Investigation, Methodology, Project Administration, Realization of operations and/or trials, Supervision, Writing - Original Draft Preparation, Writing - Review & Editing
MSM Analysis and/or data interpretation, Formal Analysis, Writing - Original Draft Preparation, Writing - Review & Editing
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket