



Articles - Year 1997 - Volume 12 -
Breast Reconstruction With Sensitive Tram Flap Reinnervation
Reconstrução Mamária com Reinervação Sensitiva do Retalho Tram
ABSTRACT
Breast reconstruction with TRAM flap (a myocutaneous flap of the rectus abdominis muscle) needs the return of the sensibility to become a complete surgery. A new surgical technique, proposed by Doncatto and Hochberg sutures both the eleventh intercostal nerves of the TRAM flap to thoracic intercostal nerves. Fifty four patients submitted to breast reconstruction with TRAM flap were evaluated. Twenty seven patients were reinnervated and twenty seven were in a control group. The recuperation of the superficial feeling was the big conquest of this surgery, and it was present in all the twenty two (81,5%) (chi square test p < O,05) patients reinnervated on the 8th month after the surgery. In the control group the superficial feeling was present only in three case (11,2%). The return of the feeling occurred in all the cutaneous surface of the TRAM flap. There was an increase in the response to the tests some time after the surgery. Deep pressure and vibration tests were positive in all the twenty patients. Superficial pain and temperature were present in eight cases of reinnervated group and one case of control group.
Keywords: Breast Reconstruction, Mammary Sensibility, Breast Cancer, Plastic Surgery, Breast.
RESUMO
A reconstrução mamária com o TRAM flap (retalho miocutâneo de músculo reto abdominal) precisa do retorno da sensibilidade para ficar uma cirurgia completa. Uma nova técnica cirúrgica posposta por Doncatto e Hochberg sutura ambos os décimo-primeiros nervos intercostais do TRAM flap com nervos intercostais torácicos. Foram avaliados cinquenta e quatro pacientes submetidas a reconstrução mamária com TRAM flap. Foram vinte e sete pacientes reinervadas cirurgicamente e vinte e sete no grupo controle. A recuperação de tato superficial foi a grande conquista desta cirurgia em vinte e duas pacientes reinervadas no 8º mês após a cirurgia duas pacientes (81,5%) (teste qui-quadrado P< 0,05). No grupo controle o tato superficial esteve presente apenas em três casos (11,2 %). O retorno do tato ocorreu em toda a superfície cutânea do TRAM flap. Houve aumento de resposta aos testes com o passar do tempo pós-cirúrgico. Os testes de pressão profunda e vibração foram positivos em todas as pacientes. A dor superficial e a temperatura estiveram presentes em oito casos do grupo reinervado e três casos do grupo controle.
Palavras-chave: Reconstrução Mamária, Ressensibilização Mamária, Câncer de Mama, Cirurgia Plástica, Mama
Breast reconstruction techniques have been presenting significant progress lately. Undoubtedly, TRAM meant important evolution regarding the shape and volume obtained in the reconstructed breast. Besides,TRAM introduces other advantages, such as exempting the use of silicon prosthesis and making simultaneously possible an improvement of the abdomen. An important aspect which was challenging surgeons was the absence of sensibility. The transplanted tissue was denervated losing its sensibility. In some cases, after a certain time, it would occur a discrete and insufficient sensitive reinnervation beginning at the cutaneous edges.
The mammary gland receives sensibility from anterior cutaneous branches from the second to the sixth intercostal nerves and from supraclavicular branches of the cervical plexus. The fourth lateral cutaneous nerve innervates the mammilla, passing through the mammary structure. The autonomous fibers of the breast follow the lateral thoracic artery and the intercostal nerves, heading to the skin, to flat muscles of the areola and the mammilla, and also to vessels and glandular tissue(6, 7, 10, 15, 25).
In order to recreate the sensitive capacity for the new breast it is necessary to make a new nervous route which will conduct the stimuli from the TRAM flap to the brain. In the regeneration in peripherical nerves, the axonal growth primarily uses the complete and integral neurilemma sheath as a duct which occurs also through the border of the flap and of the receiving bed(17, 24, 26).
The reconstruction of this neuro-conductor route was proposed(6, 7, 15) based on anatomical studies of the thoracic and abdominal intercostal nerves. New improvements on reinnervation surgery with termino-lateral neurorrhaphy allowed the renovation of the TRAM's sensibility, without any injury to the donor area.
The neurosensory reconstruction with the use of neurosensory dorsalis pedis free flap was earliest described in 1976 by Ohmori(19); and afterwards, in 1977, by Davidt(5) who reported a neurosensory pedicled deltopectoral flap. More recently; the literature has advocated the use of reinnervated flaps with a neural anastomosis as a way to reestablish sensation(2, 5, 19, 27).
The improving of the sensory in breast reconstruction with reinnervated transverse rectus abdominus was already evaluated by Slezak(21). The study compared three patients who underwent the reinnervation with ten patients who underwent identical reconstruction without nerve anastomosis. In this procedure, the neurorraphy was performed between the 11. and 12. intercostal nerves with the lateral intercostal cutaneous branch in a end-to-end suture.
Sensory recovery is much more likely to occur after fasciocutaneous flap than after musculocutaneous flap(2, 5). A direct comparison of reinervated and noninnervated patients suggests that the reconstruction of sensation in noninnervated is markedy inferior to that achieved by adding a neural anastomosis(2).
Some studies have documented sensory recovery in denerveted skin flaps without the need of neural anastomosis(3, 16, 30), although other works have contested such results(14, 33).
The purpose of this study is to describe the first results in twenty seven patients, after eight months of observation, submitted to breast reconstruction with sensitive reinnervation of the TRAM flap.
MATERIALS AND METHODS
The clinical study was aleatory and prospective, it consisted of fifty four women, ages between 30 and 60 years, submitted to the mastectomy and breast reconstruction immediately or 2 years late, at the maximum, using TRAM flap. Twenty seven of these patients had TRAM reinnervated by the technique proposed by Doncatto & Hochberg, which consists in suturing both the eleventh intercostal nerves of TRAM to the lateral side of the fourth, fifth, sixth or seventh intercostal nerves, after the opening of a 1 mm of diameter window at the epineurum, with three stitches of nylon 8-0 - 10-0(6, 7, 15) in a termino-lateral position of Viterbo(28, 29, 30, 31)(pictures 1 and 2). The other twenty seven cases were not reinnervated and served as control. The patients were operated by the same crew, at Hospital Presidente Vargas - MS, in Porto Alegre, following the same surgical routine. They were submitted to monthly evaluation, by two examiners, by the clinical method described by Adams & Victor(1): touch (hair brush), pressure (finger), pain (needle), thermal sensibility (hot and cold water-filled test tube) and vibration (forks). We have evaluated both touch and moving touch, deep pressure, temperature, vibration and superficial pain. The tests were repeated ten times, and we considered them positive when patients declared that they were feeling the stimuli in at least half of the skin flap. The intensity of the stimulus was not measured.
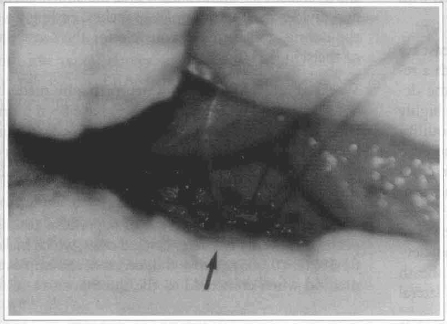
Fig. 1 - Picture of the termino-lateral neurorrhaphy of the 11th intercostal nerve with the 4th thoracic intercostal nerve.

Fig. 2 - Picture of the termino-lateral neurorrhaphy of both the 11th intercostal nerves with the 4th and 5th thoracic intercostal nerve.
RESULTS
Superficial feeling was the positive test that made a difference between the two groups. The twenty seven patients who were observed had positive results at the superficial feeling test after the 8th month of post-reinnervation (chi square test p < 0,05). On the twenty patients submitted to the neurorrhaphy with only one of the 11th intercostal nerves, it was observed the delimitation of the sensibility on the skin of TRAM between the are as with or without reinnervation in seventeen cases. In eigth cases thoracic skin was completely insensitive, but the reinnervated TRAM got a positive response from the test. In another case, in spite of the resection of the peripherical scar to the flap, it remained sensitive. At the control graup, not reinnervated, there was three cases with positive response to superficial feeling. Tests of deep pressure and vibration remained identical on both graups, turning positive in all cases. The temperature and superficial pain were present in eight cases in the reinnervated graup and in one case in the control graup.
DISCUSSION
New and important contributions to the breast reconstruction surgery arise, such as the possibility of the return of the new breast's sensibility, aesthetic refining of the TRAM, preservation of the submammary furrow and mastectomy by periareolar approach with immediate breast reconstruction(11, 12).
The psychological aspects involved in the breast reconstruction are widely known(4, 13). Even with a reconstructed breast insensitive to the touch, the degree of satisfaction of the patients is already highly elevated, contributing to their emotional equilibrium(13, 18, 22). It is not difficult to imagine the even better results which would be obtained at the emotional sphere if the reconstructed breast becomes sensitive to the touch. Anatomical studies(6, 7, 8, 15, 23) previously developed showed that the sensitive nerves of the TRAM flap are determined mainly by the eleventh intercostal nerve which crosses the lateral sheath of the rectus abdominus muscle, perforates its lateral third, crosses its lateral sheath and the subcutaneous and divides itself in multiples branches, ending up at the derma, and being responsible for the sensibility of the skin flap (fig. 3).

Fig. 3 - Picture of the innervation of the isle of TRAM done by the 11th intercostal nerve.
Works about termino-lateral neurorrhaphy made by Viterbo(28) and repeated by Ross(20) have been promising towards the sensitive(29) and motive(30, 31) reinnervation, allowing the utilization of one donor nerve without any damage to the structures innervated by it.
The results obtained in terms of superficial feeling, positive in twenty two reinnervated cases, which makes 81,5% (P < O,005), prove the success of the employed method when compared to the three positive result obtained in the twenty seven cases(11,2%) of the control group (not reinnervated). The results achieved with the bilateral reinnervation using both the eleventh intercostal nerves and obtaining sensibility on the full isle of TRAM indicate that this is the best option, since when the single neurorrhaphy was done, occurred an unilateral sensibility of the flap (fig. 4). The eight described cases where the thoracic skin nearby the flap was insensitive, opposing to the TRAM, confirm that the sensibility obtained was provenient from the neurorrhaphy. In another case, although there were a full resection of the scar around TRAM, the patient maintained the reinnervation tests. In these cases there would be no possibility of growth of the axons through the scar to make the TRAM sensitive(17, 24, 26).
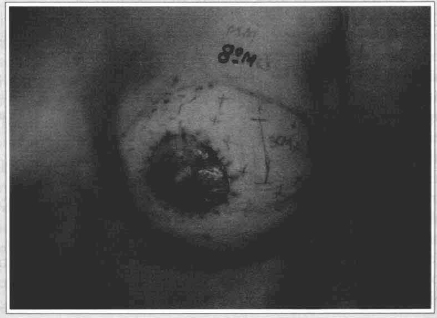
Fig. 4 - Patient on the 8th month of reinnervation, where the areas with (+) and without (-) tactile sensibility can be seen.
The termino-lateral neurorrhaphy occurred between the anterior and medium axiliary lines because in this area 70 to 90% of the fibers are sensitive(9, 17).
A progressive increase in the response to all of the tests, once the time of microneurorrahphy went by; was noticed. It suggests an increase on the density of reinnervated receivers on the surface of TRAM(17, 24). These finds were previously reported only for deep pressure and vibration(21).
The control group had three cases of superficial feeling present, which could be explained by aleatory reinnervation(9, 17, 21, 26).
The increase of the sensitive capacity of this new reinnervated breast will allow the patient to develop a sensitive reeducation of the postoperative and consequently to feel a visual response to localize the spots of the sensibility return. It will also allow the patient to acquire new feelings towards the new reinnervated breast(13, 21).
CONCLUSIONS
The presented cases show the possibility of sensitive reinnervation of TRAM flap in breast reconstruction with termino-lateral neurorrhaphy Reinnervated patients presented a return of the superficial feeling at the surface of TRAM. The rest of the tests were similar on both groups.
REFERENCES
1. ADAMS, R.; PAIN, V M. - Principles of Neurology. New York: Mc graw-hill, inc. 111-129. 1993
2. BOYD, B.; MULHOLLAND, S.; GULLANE, P. - Reinnervated lateral antebrachial cutaneous neurosome flaps in oral reconstruction: are we making sense? Plastic and Reconstructive Surgery, 93, 1350-1359. 1994.
3. CLOSE, L. G.; TRUELSON, J. M.; MILLEDGE, R. A, SCHWEITZER, C. - Sensory Recovery in Noninnervated Flaps Used for Oral Cavity and Oropharyngeal Reconstruction. Arch Otolaryngol Head Surg. vo1 121, sep. 1995.
4. COURTISS, E. H. & GOLDWYN, R. M. - Breast sensation before and after plastic surgery. Plastic and Reconstructive Surgery, 58, N. l, 1. 1976
5. DAVID, D. - Use of an innervated deltopectoral flap for intraoral reconstruction. Plastic and Reconstructive Surgery, 60, 377-380, 1977.
6. DONCATTO, L.; HOCHBERG, J.; CALEFFI, M. - O retalho TRAM com reinervação sensitiva para reconstrução mamária. Revista Brasileira de Mastologia. São Paulo, vol. 5, No. 3, 20-23. 1995.
7. DONCATTO, L.; HOCHBERG, J.; FAGERLI, J. - Sensory Reinnervation of the TRAM Flap for Breast Reconstruction - An Anatomical Study and Technique Proposal. Southeastern Surgical Congress 64th Annual Scientific Meeting & Postgraduate Course. Tampa, Florida. Feb., 39. 1996.
8. DUCHATEAU, J.; DECLETY, A; LEJOUR, M. - Innervation of rectus abdominal muscle: Implications for rectus flaps. Plastic and Reconstructive Surgery. Vol 82, No 2, 223-228. August. 1988.
9. FREILING, G.; HOLLE, J.; SULZGRUBER, S. C. - Distribution of motor and sensory fibers in the intercostal nerves. Plastic and Reconstructive Surgery. 62. n. 2. 240. 1980.
10. GARDNER, E.; GRAY, D. J.; O'RAHILLY, R. - Anatomia - Estudio por regiones del cuorpo humano. Barcelona. 2. ed. Salvat Editores, S.A Pp. 356-463. 1982.
11. GÓES, J. C. S. - Immediate Reconstruction with Tissue Expander after Mastectomy by Areolar Approach. The Breast Journal, 2(1): 71-76, 1996.
12. GÓES, J. C. S. - Mastectomy by Periareolar Approach with Immediate Breast Reconstruction. Rev Soc Bras Cir Plast 10(3): 44-55. 1995.
13. GOIN, M. K - Psychological reactions to prophylactic mastectomy synchronous with contralateral breast reconstructions. Plastic and Reconstructive Surgery. 70. n.3. 355. 1982.
14. HERMANSON, A.; DALSGAARD, C.; ARNANDER, C. - Sensibility and cutaneous reinnervation in free flaps. Plastic and Reconstructive Surgery. 79. 422-425. 1987.
15. HOCHBERG, J. & DONCATTO, L. - Sensory Reinnervation of the TRAM Flap for Breast Reconstruction. An Anatomical Study and Technique Proposal. 64th Annual Scientific Meeting of American Society of Plastic and Reconstructive Surgeons. INC. Montreal. Vo. XVIII, 227-229. 1995.
16. LEHMANN, C.; GUMENER, R.; MONTANDON, D. - Sensibility and cutaneous reinnervation after breast reconstruction with musculocutaneous flaps. Annals of Plastic Surgery. Vo1 26, no. 4 april l991.
17. LEE DELLON, A & MACKINNON, S. - An alternative to classical nerve graft for the management of the short gap. Plastic and Reconstructive Surgery. 82. n. 5. 849. 1988.
18. NOONE, R. B.; FRAZIER, T. G.; HAYWARD, C. Z.; SKILES, M. S. - Patients acceptance of immediate reconstruction following mastectomy. Plastic and Reconstructive Surgery. 69. n. 4. 632. 1982.
19. OHMORI, K., HARII, K. - Free dorsalis pedis sensory flap to the hand, with microneurovascular anastomosis. Plastic and Reconstructive Surgery 58, 546-554, 1976.
20. ROSS, D. A; MATSUDA, H.; ZUKER, R.M. - 64th Annual Scientific Meeting of American Society of Plastic and Reconstructive Surgeons. INC. Montreal. Vol. XVIII. 156-157. 1995.
21. SLEZAC, S.; McGIBBON, B.; LEE DELLON, A. - The sensational transverse rectus abdominis musculocutaneous flap (tram): Return of sensibility after tram breast reconstruction. Annals of Plastic Surgery. 28. n. 3. 210. 1992.
22. STEVENS, L. A, et al. - The psychological impact of immediate breast reconstruction for women with early breast cancer. Plastic and Reconstructive Surgery. 73. n. 4. 619. 1984.
23. TAYLOR, G. I.; GIANOUTSOS, M. P.; MORRIS, S. F - The neurovascular territories of the skin and muscle: anatomic study and clinical implications. Plastic and Reconstructive Surgery. 94, n. 1. 1984.
24. TERZIS, J. K.; VINCENT, M. P.; WILKINS, L. M., KEN RUTLEDGE, B. S. et al. - Reinnervation of glabrous skin in baboons: Properties of cutaneous mecanoreceptores subsequent to nerve transection. Journal of Neurophisiology. 44, n. 6, 1214. 1980.
25. TESTUT, L. - Traite D'anatomie Humaine. Paris. 2 tome. Octave doin editeur. Pp. 301-307.1897.
26. TURKOF, E.; JURECKA, W.; SIKOS, G.; PIZA-KATZER, H. I. - Sensory recovery in myocutaneous noninervated free flaps: A moephologic immunohistochemical and electron microscopic study. Plastic and Reconstructive Surgery. 92. n. 2. 238. 1993.
27. URKEN M. BILLER H. A new bilobed design for the sensate radial forearm flap to preserve tongue mobility following significant glossectomy. Arch Otolaryngol Head Surg. vol 120, jan. 1994.
28. VITERBO, F. V. O. N. - Neurorrhaphy latero-terminal. Thesis. Botucatu Medical School. São Paulo, Brazil, 1982.
29. VITERBO, F; PALHARES, A; FRANCIOSI, L. F - Restoration of sensitivity after removal of the sural nerve. A new application of termino-lateral neurorrhaphy. Rev Paul Med. 112(4): 658-660, out/nov/dez. 1994.
30. VITERBO, F.; FRANCIOSI, L. F.; PALHARES, A. - Nerve Graftings and End-to-side Neurorrhaphies Connecting the Phrenic Nerve to the Brachial Plexus. Plastic and Reconstructive Surgery. 96(2) 494-495. 1995.
31. VITERBO, F. - A New Method for Treatrnent of facial Palsy: The Cross-Face Nerve Transplantation with end-to-side Neurorrhaphy. Revista da Sociedade Brasileira de Cirurgia Plástica Estética e Reconstrutiva. Jan/Dec. 8(1-3): 29-38. 1993.
32. VRIES J. P. M.; ACOSTA, R.; SOUTAR, D. S.; WEBSTER, M. H. C. - Recovery of sensation in the radial forearm free in oral reconstruction. Plastic and Reconstructive Surgery. 98(4) 649-656. 1996.
33. WOODWARD, K.; KENSHALO, D. - The recovery of sensory function following skin flaps in humans. Plastic and Reconstructive Surgery. 79, no. 3, 428-433, 1987.
ACKNOWLEDGMENT
We acknowledge Dr. Julio Hochberg for his help in turning the anatomical dissection feasible, and for his contribution in the technique development.
I - Plastic Surgeon of Hospital Presidente Vargas
Titular of the Brazilian Plastic Surgery Association
II - Mastologyst of Hospital Presidente Vargas
Member of the Brazilian Mastology Association
Work Performed at the Department of Surgery and Gynecology of Hospital Presidente Vargas (HMIPV) Porto Alegre - RS
Address for Correspondence:
Léo Doncatto, MD
Rua Mostardeiro, 780 , cj. 202 - Moinhos de Ventos
90430-000 - Porto Alegre - RS - Brazil
Phone/Fax +55 51 222-6820
e-mail: doncatto@nutecnet.com.br
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket