



Special Article - Year 2021 - Volume 36 -
Z-plasty in the treatment of unilateral cleft lip: review of its history
Plástica em Z no tratamento da fissura labial unilateral: revisão de sua história
Sergio Carreirão1 ; Leila Lemos Azem1,*; Rafael Sucupira Menezes1; Laila Bleibel Zraik1
; Leila Lemos Azem1,*; Rafael Sucupira Menezes1; Laila Bleibel Zraik1
ABSTRACT
The study reviews the use of Z-plasty in the cheiloplasty techniques used to treat unilateral cleft lip. It highlights the contribution of Brazilian authors, especially that of Perseu Lemos. It also reports the conduct adopted by the senior author in this type of cheiloplasty.
Keywords: Burns; Cicatrix; Surgery, Plastic; Cleft lip; Surgeons.
RESUMO
O trabalho faz uma revisão do emprego da plástica em Z nas técnicas de queiloplastia empregadas para o tratamento da fissura labial unilateral. Destaca a contribuição de autores brasileiros, principalmente a de Perseu Lemos. Relata também a conduta adotada pelo autor sênior neste tipo de queiloplastia.
Palavras-chave: Queimaduras; Cicatriz; Cirurgia plástica; Fenda labial; Cirurgiões.
INTRODUCTION
This article aims to clarify and disseminate the history of cheiloplasty in the treatment of unilateral lip fissures. It intends to demonstrate the fundamental importance of eminent Brazilian plastic surgeons in their creation, execution and teaching1.
About the origins of Z-plasty
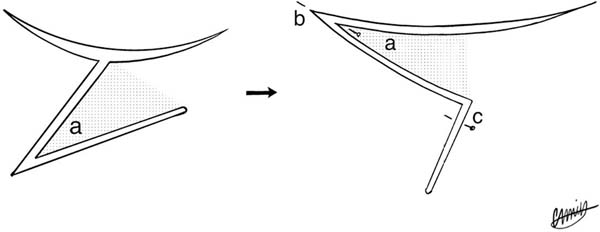
The first reference we found of a Z-plasty is credited to Horner in 18372,3. As professor of anatomy at the University of Pennsylvania, he reported the case of a left lower eyelid ectropion caused by a burn scar four years ago (Figure 1).
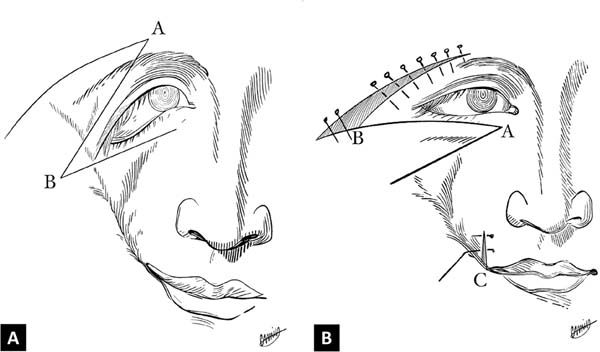
Some authors attribute to Denonvilliers (1863)4 the first execution of a Z-plasty when he operated on a young man with ectropion outside the lower right eyelid. The case was presented on 20/09/1854 at the Société de Chirurgie in Paris. This description was reported in Cazelles’ thesis in 18605 (Figure 2).
McCurdy was who first used the term Z-plasty at the University of Pittsburg in 19136. There are doubts that McCurdy has been aware of previous work on Z-plasty7.
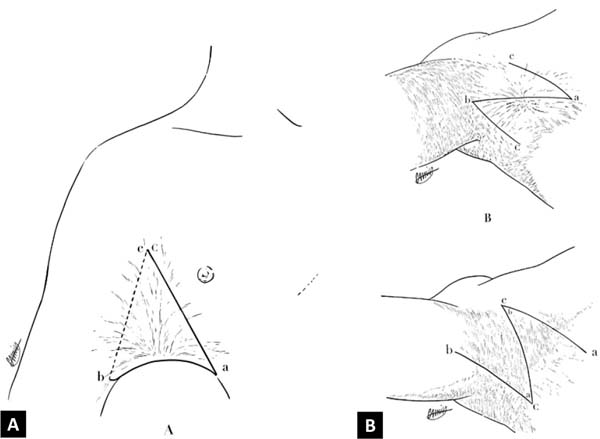
In 1904, Berger8 described a typical transposition of Z-plasty to treat armpit burn sequelae (Figure 3).
Small historical tour on the treatment of unilateral cleft lip
In 1836, Millard9 called for the treatment of unilateral cleft lip fissures by curved incisions, but which excised a lot of lip tissue, although stretching was effective. In 1891, Rose10 proposed a design similar to Millard (1836)9, with concave incisions on both sides of the fissure and preserving more labial tissue. The incisions went from the nostril to the vermilion, and the technique became popular (Figure 4).
Later, in 191211, Thompson described his technique with incisions angled at the edges of the fissure in an attempt to outline the curves of a normal lip. It performs curved incisions similar to rose’s (1891)10 at the fissure edges, making accurate measurements with a calibrated compass. Today the straight excision and scar technique is known as the Rose & Thompson technique (Figure 5).





Millard (1836)9 reports that Veau,in19259, published a unilateral cheiloplasty technique in which for the first time a Z-plasty was used, but located on the vermilion, slightly surpassing this and reaching the lip, which could impair the continuity of the cutaneomucosal line. At the time, Z-plasty was accepted as a procedure to solve straight line contractures, and according to Veau (1925) X could be used to attenuate the straight line of cheiloplasty secondarily.
It is important to note that although Masters et al., in 195412, have advocated using intermediate Z-plasties to repair incomplete labial fissures, it was Lemos in 195613 who first proposed a cheilo-Z-plasty for the repair of unilateral labial fissures. The technique of Lemos (1956)13 was modified by Spina and Lodoviciin 196014 and came to bring contributions to the technique of Lemos (1956)13. In 1961, Petit et al.15 proposed a technique with two triangular flaps; they preached that a double Z produced a better rotation of the nasal wings and a better release of the lip.
The technique of Perseu Lemos
We considered that Perseu Castro de Lemos (1956)13 was the first to recommend repairing unilateral cleft through a Z-plasty of the entire lip thickness: skin, musculature and mucosa. Its first publication was in the journal O Hospital in Rio de Janeiro (1956)13 soon after the technique was presented at the International Congress of Plastic Surgery in Rome (1967)16.
We also found in the literature reference of a previous note made by Lemos (1956)13 recorded at the 5th State Medical Congress of Pernambuco: “A new technique for the correction of the leporine lip17”.
Interesting to know the fundamentals of the technique by the author’s own description: “We then conceived our operation which consisted essentially of the excision of the edges of the fissure, respecting the beginning of the cupid’s bow, and then performing a simple Z-plasty to lengthen the lip and break the suture line. This Z-plasty, which was initially described in the middle third of the lip, can be placed where it is most necessary, that is, in the upper, middle or lower thirds. Equally, the branches’ angulation may vary in such a way as to obtain a more satisfactory result, according to the case. The resulting triangular flaps, incised throughout their lip thickness, are sutured between crossed, restraining the resulting small excesses. As a final result, we have a preserved cupid’s bow lip, with minimal tissue removed and a broken scar, with no tendency to shrink.”18.
The author adds: “Surgery is above all of easy to do, no longer requiring the surgeon than knowledge of the technical bases of Z-plasty. However, the only resulting drawback is the interruption of the common filter crest to all techniques with non-rectilinear scars.”18.
Dr. Perseu13 (this is how he was better known) refers to having applied the technique for the first time in 1953, performing the technique for all types of unilateral lip fissures: complete or incomplete, with or without cleft palate, in secondary repairs, always obtaining satisfactory results. To do so, he said, it is enough to have common sense in the positioning of the lateral branches of the Z, in the most convenient length, height and direction. In a 26-year retrospect, he assesses having operated around 1,000 cases19.
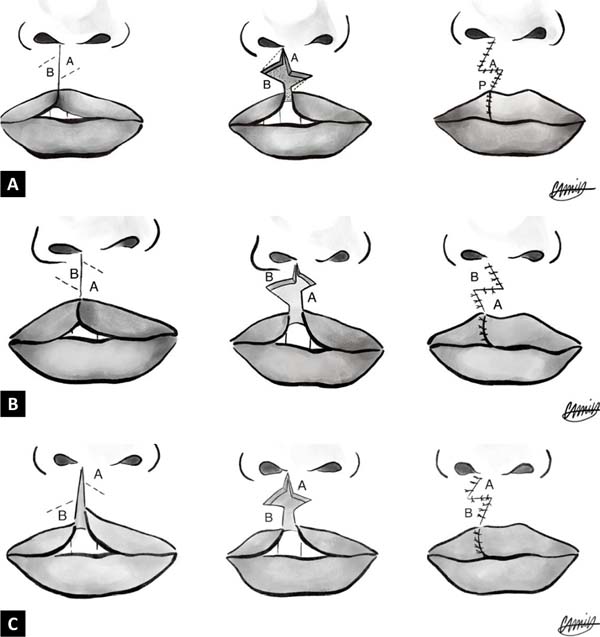
Still, in the words of the master himself: “Although we initially described the Z in the middle third of the lip, we immediately evolved into the concept that it can be positioned lower or higher or preferably in the upper third with Z branches arranged so that the external triangular flap created promotes the rotation alar up and in, better reconstructing the nasal introitus. In fact, we think that the wide variety of positions, angles, height and orientation of the branches are the best thing of the technique.”18,19 (Figure 6).

The technique of Victor Spina and Orlando Lodovici
In 1959 and 1960, Victor Spina, together with Orlando Lodovici14,20, proposed the Z- plasty only to the cutaneous plane, which seemed sufficient to determine the proper increase in lip height.
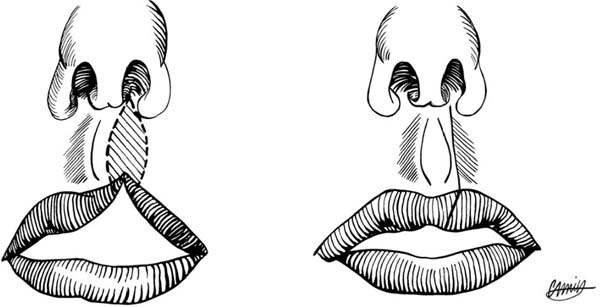
In his Z-plasty, the upper arm is medial, and the lower arm is lateral. He presents an ingenious repair of the vermilion without resections and the entire mucosa’s use in part decorticated and buried in the contralateral slope (Figure 7). Spina and Lodovici (1960)20 recognize that their method corresponds to Lemos’s (1956)13 with its own modifications to obtain better results. He spread the technique a lot throughout Brazil, which became known to some as the Lemos & Spina technique. It is a procedure widely used to this day21.


Other authors
Davies, in South Africa, published in 196522, cheiloplasty with two equal flaps of pure Z-plasty. It also employs a Z-plasty of all planes and curiously does not cite Lemos (1956)13. He admits that the biggest snarl of his technique is that the final scar crosses the filter crest.
In 1959, Clifford and Pool23 reviewed the principles of Z-plasty in cleft lip surgery, an article that deserves to be consulted. In 1949, Huffman and Lierle24 described a cleft repair technique based only on the principle of Z-plasty, mainly using accurate geometric measurements.
Today, it is known that in the use of Z-plasties in cheiloplasties, its principles cannot be violated. When the design of Z-plasty is not well planned, some valuable lip tissue can be redried, and the final scar may violate the repair lines of the lip filter. So, therefore, the importance of Lemos (1956)13 and Spina and Lodovici (1959, 1960)14,20.
Repair of the musculature of the unilateral cleft
The mentioned cheilo-Z-plasties, at the time of their performance, did not consider the adequate treatment of muscle deformities of the unilateral cleft lip to be performed. This point seems important for us to update these techniques.
Fara, in 196825, performed dissections in stillborns with fissures. He described the anomalous anatomical disposition of the muscular bundles of the fissure. He also noticed that there was hypoplasia (poverty) of fibers on the medial side. According to Randall et al., in 197426, “the functional treatment of cleft lip clefts implies reorienting the lip muscles, regardless of the type of skin incision to be used.” Another proposal for surgical reorientation of orbicular fibers described by Skoogin 197427 emphasizes the complete restoration of the lip’s muscular anatomy.
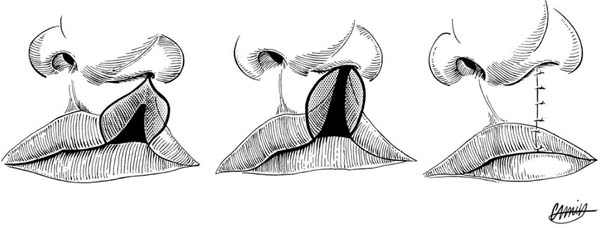
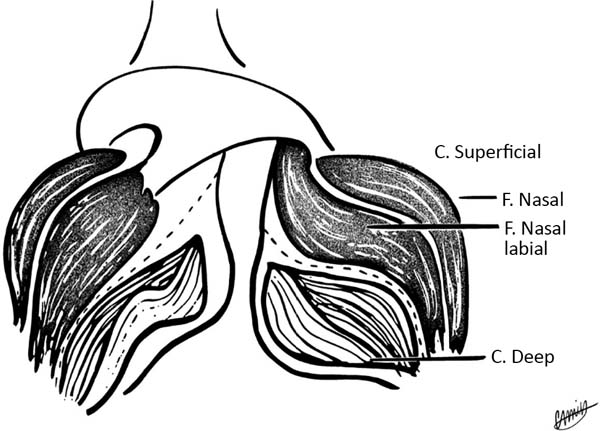
Nicholas, in 198328, described the anatomy of the orbicularis of the lips with two layers: one superficial whose fibers are related to facial mimicry and the other deep whose fibers account for the sphincter function of the lip, having importance in eating and retaining food in the mouth. The surface layer presents an important alteration of its insertions in patients with cleft lip29 (Figure 8).

Both Nicholas (1983)28, and Randall et al. (1974)26 and Kernahan (1978, 1983)30,31,32 highlight that the modern treatment of unilateral fissure undergoes an adequate orbicular muscle reconstitution because the result of cheiloplasty should be evaluated not only in the resting situation of the lip but also and, mainly, in activities such as smiling and whistling.
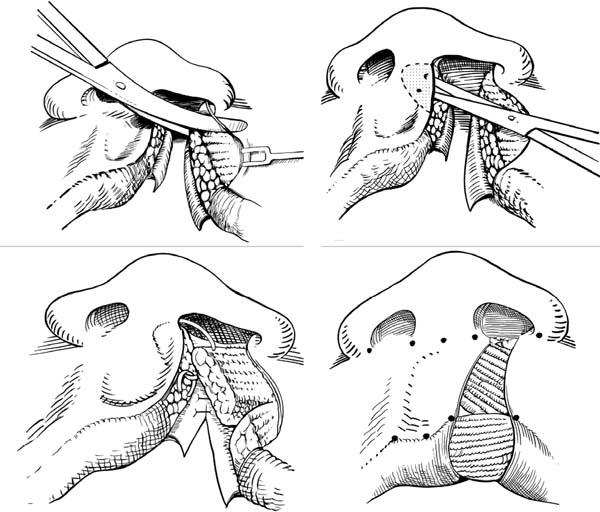
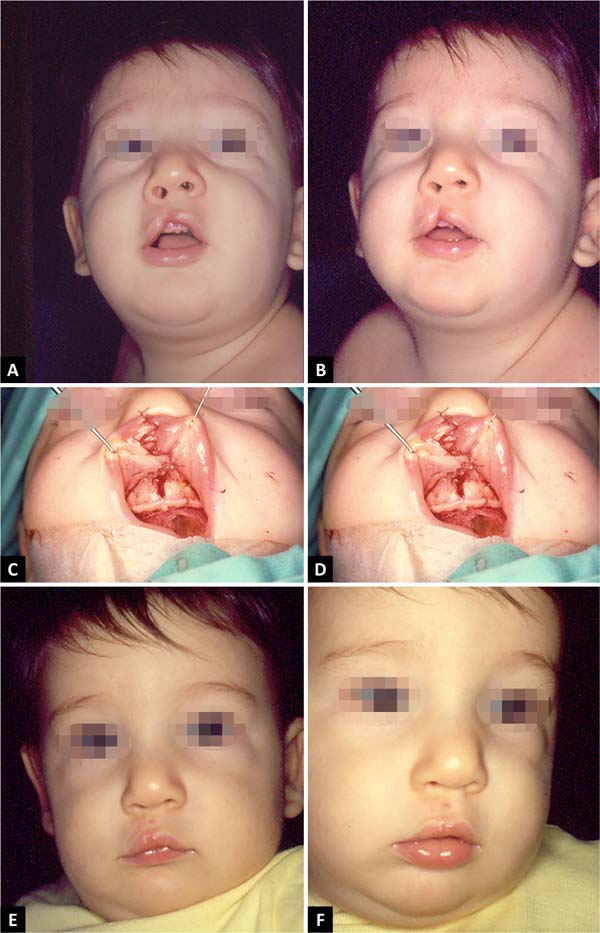
Although they attach the same importance to the musculature’s reconstitution, all these authors approach the musculature differently. We have always been interested in the technique proposed by Kernahan (1978, 1983)30,31 with which we obtained functionally and aesthetically very satisfactory results (Figure 9).
The proposal for a cheilo-Z-plasty
The use of Z-plasty in the treatment of unilateral fissures swelled with great benefits. For its simplicity, ease of execution and learning will always be a resource that can be used.

To keep alive the principles of Lemos (1956)13 and Spina and Lodovici (1959, 1960)14,20, with Z-plasties on the skin and labial mucosa and conservative treatment of lip vermilion flaps, appropriate treatment of the orbicular musculature should be added to them. In our hands, what offered us better results was the Kernahan technique (1978, 1983)30,31. We used this technique for incomplete cracks, narrow and aligned complete fissures.
Here is the scheme of the technique that seems to us the most appropriate:
CONCLUSION
In 1996, Dr. Perseu19 considered that despite the new techniques that emerged over time that seek to reconstruct the filter crest on the fissure side, some prefer Z-plasty for producing less scar retraction, a preserved cupid’s bow, with minimal tissue removed. The drawback is the interruption of the filter crest, common, however, to all techniques with non-rectilinear scars. It also points out that philosophically all its concepts that remain valid:
DEDICATION
Work dedicated to Perseu Castro de Lemos, master and friend of the senior author and who, in 1994, expressed: “I consider all my contributions to plastic surgery, cheilo-Z-plasty as the most important”1.

REFERENCES
1. Lemos P. Pelos caminhos da cirurgia plástica. Recife: Edições Bagaços; 1994.
2. Horner WE. Clinical report on the surgical department of the Philadelphia Hospital, Blockley for months of May, June and July 1837. Am J Med Sci. 1837;21:105-6.
3. Borges AF, Gibson T. The original Z-plasty. Br J Plast Surg. 1973 Jul;26(3):237-46.
4. Denonvilliers CP. De la méthode autoplastique par pivotempar appliquée à la restauration des paupières. Bull Gén Thér Méd Chirurg. 1863;65:110-22.
5. Cazelles EH. Du traitment de l’ectropion cicatriciel [tese]. Rognoux: Faculte de Médicine de Paris; 1860.
6. McCurdy SL. Z-plastic surgery: plastic operation to elongate cicatricial contraction of the neck, lips and eyelids and across the joints. Surg Gynecol Obst. 1913;16:209-11.
7. Borges AF. Historical review of Z-plastic techniques. Clin Plast Surg. 1977 Abr;2(4):207-16.
8. Berger VP. Autoplastie par dédoublement de la palmure et échange de lambeaux. In: Berger P, Banzet S, eds. Chirurgie ortopédique. Paris: Steinfeil; 1904. p.180-5.
9. Millard Junior DR. Cleft craft: the evolution of its surgery. Volume 1 I. The Unilateral Deformity. Boston: Little, Brown and Company; 1976.
10. Rose W. On harelip and cleft palate. London: HK Lewis; 1891.
11. Thompson JE. An artistic and mathematically accurate method of repairing the defect in cases of harelip. Surg Gynecol Obst. 1912;14:498-505.
12. Masters F, Georgiade N, Horton C, Pickrell K. Use of interlocking Z’s in repair of incomplete clefts of the lip. Plast Reconstr Surg. 1954 Out;14(4):287-92.
13. Lemos PC. Nova operação para lábio leporino simples. O Hospital. 1956;1(4):607-11.
14. Spina V, Lodovici O. Conservative technique for treatment of unilateral cleft lip. Reconstruction of the midline tubercle of the vermilion. Br J Plast Surg. 1960;13:110-7.
15. Petit P, Borde J, Malek R. Treatment of harelip by means of a plastic procedure using a equilateral triangular flap. Ann Chir Infant. 1961 Dez;2:111-6.
16. Lemos PC. Cheilo-Z-plasty. Rev Lat Am Cir Plast. 1962;4(3):270-4.
17. Lemos PC. Novas técnicas para a correção do lábio leporino simples, uni e bilateral (nota prévia). 5º Congresso Médico Estadual de Pernambuco (Garanhuns), 1953 (Nov).
18. Lemos PC. Tratamento da fissura labial unilateral. In: Lessa S, Carreirão S, eds. Tratamento das fissuras labiopalatinas. Rio de Janeiro: Editora Interamericana; 1981. p. 37.
19. Lemos PC. Quilozetaplastia técnica pessoal para o tratamento cirúrgico das fissuras labiais unilaterais. In: Tratamento das fissuras labiopalatinas. In: Lessa S, Carreirão S, Zanini S, eds. Tratamento das fissuras labiopalatinas. Rio de Janeiro: Revinter; 1996. p. 81.
20. Spina V, Lodovici O. Técnica conservadora para o tratamento do lábio leporino unilateral: reconstituição do tubérculo mediano. Rev Assoc Med Bras. 1959;5(5):325-30.
21. Anger J. Prof. Perseu Castro de Lemos e Prof. Spina: a história da plástica em Z na queiloplastia para a correção das fissuras lábio-palatinas unilaterais. Rev Soc Bras Cir Plást. 2005;20(4):245-7.
22. Davies D. The repair of unilateral cleft lip. Br J Plast Surg. 1965 Jul;18:254-64.
23. Clifford RH, Pool Junior R. The analysis of the anatomy and geometry of the unilateral cleft lip. Plast Reconstr Surg Transplant Bull. 1959 Out;24:311-20.
24. Huffman WC and Lierle DM. Studies on the patholic anatomy of the unilateral harelip nose. Plast Reconstr Surg. 1949 Mai;4(3):225-34.
25. Fara M. Anatomy and arteriography of cleft lips in stillborn children. Plast Reconstr Surg. 1968;42:29-36.
26. Randall P, Whitaker L, LaRossa D. The importance of muscle reconstruction in primary and secondary cleft lip repair. Plast Reconstr Surg. 1974 Set;54(3):313-23.
27. Skoog T. Plastic surgery: new methods and refinements. Stockholm: WB Saunders; 1974.
28. Nicolau PJ. The orbicularis oris muscle: a functional approach to its repair in cleft lip. Br J Plast Surg. 1983 Abr;36(2):141-53.
29. Giglio AT. Tratamento funcional das fissuras labiais unilaterais. In: Lessa S, Carreirão S, eds. Tratamento das fissuras labiopalatinas. 2ª ed. Rio de Janeiro: Revinter; 1996. p. 77.
30. Kernahan DA. Muscle repair in unilateral cleft lip, based on findings on eletrical stimulation. Ann Plast Surg. 1978;1(1):48-53.
31. Kernahan D, Bauer BS. Functional cleft lip repair: a sequential layred closure with orbicularis muscle realingment. Plast Reconstr Surg. 1983 Out;72(4):459-66.
32. Kernahan DA. The functional cleft lip repair with muscle alignment. In: Kernahan DA, Rosenstein SW, eds. Cleft lip and palate-a system of management. Baltimore: Williams & Wilkins Co.; 1990. p. 149.
1. Hospital da Plástica do Rio de Janeiro,
Rio de Janeiro, RJ, Brazil.
Corresponding author: Leila Lemos Azem, Rua Julio de Castilhos, 83/301, Rio de Janeiro, RJ, Brazil., Zip Code: 22081-025, E-mail: leilazem@globo.com
Article received: July 22, 2020.
Article accepted: January 10, 2021.
Conflicts of interest: none
Institution: Hospital da Plástica do Rio de Janeiro, Rio de Janeiro, RJ, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket