



Articles - Year 1997 - Volume 12 -
Use of Prosthesis in the Femoral Region
Uso de Próteses na Região Femoral
ABSTRACT
The author presents his experience with cosmetic surgery of the legs, to improve the shape of the socalled "thin legs", resulting from muscular atrophy of the femoral region. Molded silicone-gel prosthesis are placed under the muscles ofthe inner thighs. The technique is simple and the surgical steps are described. A special instrument is employed which facilitates and helps the dissection and placement of the prosthesis through a small 5 cm incision in the subgluteal fold. A more harmonious contour of the legs in the femoral region is achieved.
Keywords: Próteses, Região Femoral, Pernas
RESUMO
O autor relata sua experiência na cirurgia estética das pernas para a melhora do contorno inestético das chamadas pernas finas face às hipotrofias da musculatura da região femoral. Próteses moldadas de silicone-gel são implantadas sob a musculatura da coxa interna. A técnica é simples e apresentada em suas minúcias. O autor utiliza um instrumento especial que facilita e ajuda a dissecção e colocação das próteses através de pequena incisão de 5 cm na região do sulco subglúteo. Logra-se um aspecto mais harmonioso do contorno das pernas nas regiões femorais.
Palavras-chave: Próteses, Região Femoral, Pernas
In the search for perfecting the shape of the lower limbs, plastic surgery accomplishes procedures which permit the increase in the perimeter of the femoral region. It is based on the same principles of placing prosthesis in the calves, since molded silicone-gel prosthesis are utilized. They are specially designed prosthesis, triangular in shape with its base cephalad, following the geometric shape of the lower limbs.
Sizes range from 18 to 24 cm in length, 6 to 8 cm in width and 2.5 to 3 cm in height (Fig. 1).
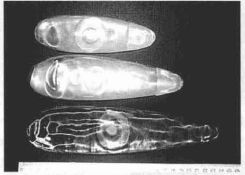
Fig. 1 - Types of Montellano silicone-gel leg prosthesis.
Material and Methods
Usually peridural anesthesia is used with the patient in ventral decubitus.
The approach is through the subglutealline, via a ± 5 cm skin incision. The subgluteal cellular tissue is dissected up to muscular aponeurosis: internal rectus, internal vastus and median aductor. Vertical dissection below these muscles, introducing the head ofthe special elevator in this opening (Fig. 2). The instrument is introduced gently toward the umer side ofthe knee, as already mentioned the undermining proceeds below these muscles.
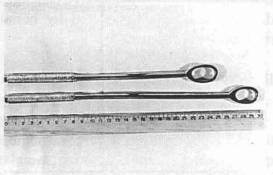
Fig. 2 - Leg elevators designed by the author.
Important structures are not injured, neither the internal saphenous nerve nor the femoral artery and vein are affected, since the blunt dissection is simple, atraumatic, with minimum bleeding and without major problems (Fig. 3). A guide is used to introduce the prosthesis in this region of the inner thigh, placing it along the pocket fashioned (Fig. 4). An adhesive bandage is used for the dressing which is completed by bennuda shorts of medium compression.
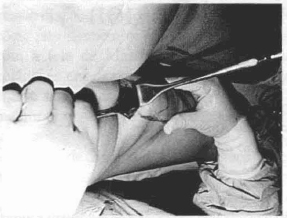
Fig. 3 - Atraumatic blunt dissectioll on the inner thigh.
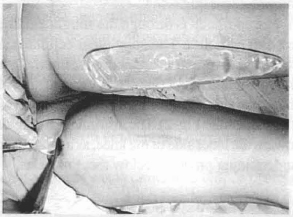
Fig. 4 - Introduction of the prosthesis in the tailored pocket.
Results
An increase in perimeter ranging from ± 2-3 cm is obtained throughout the femoral region, achieving a more pleasing aspect to the mid femoral thigh. The scar is concealed in the gluteal fold (Figs. 5,6).
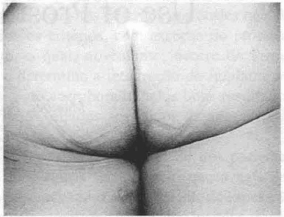
Fig. 5 - the scar is cancealed in the gluteal Fold.
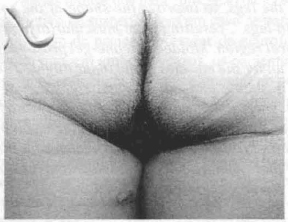
Fig. 6 - Aspect ojthe scars ill the sulcus, raising the bUllocks.
A total of 25 surgeries were perfonned. No capsular contractions nor distortions in the shape of the leg were observed in the immediate or late post-operative stages (Figs. 7,8,9, 10).

Fig. 7 - Preoperative. Thin thighs.
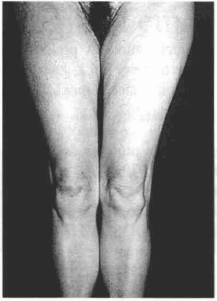
Fig. 8 - Post-operative aspect with prosthesis.

Fig. 9 - Preoperative. Posterior thigh.

Fig. 10 - Post-operative with femoral prosthesis.
Discussion
This surgery is indicated for muscle atrophy caused by poliomyelitis in this region, for burn and accident sequelae with deformation of the femoral region. The objective of most of these surgeries, is purely esthetic, for the so-called "thin legs" and "genu valgum" legs. Large size prosthesis are inserted for the most part.
This technique is similar to other inclusion surgeries and is one more option for the plastic surgeon's arsenal.
It is not only esthetic, but also reconstructive. X-rays taken in the late p.o. period, confinn maintenance ofthe prosthesis'position in the inner femoral region (Figs.11,12).

Fig. 11 - Marking the prosthesis of the inner femoral leg.

Fig. 12 - X-ray, position of the prosthesis. Inner thigh.
References
01. CARLSEN L. Calf augmentation. A preliminary report. Annals of Plastic Surgery Vol 2 - JWle, 1979.
02. FINOCHlETTO R. Cirurgia basica.Lopes Libreros Editores. Buenos Aires, 1962.
03. CLiCENSTEIN J. Corre~ao das aminotrofias dos membros por inclusiio de proteses de silicone. Rev Bras Cir, 69 (3/4): 1979.
04. GO ZALEZ UM. Tecnica quinirgica: Comunicacion personal. Sao Paulo, 1982.
05. HAKME F, GOMES B, SJOSTEDT C et al. Prevenção e tratamento da contratura capsular. Revista Bras. Cir, 74 (2): 59-64, 1984.
06. MONTELLANO L. Plastica da panturrilha. Anais XXll Cong Bras Cir Plast, Gramado, APLUB, 637,1985.
07. MO TELLANO L. Aesthetic calf surgery. Annals of the International Symposium "Recent Advances in Plastic Surgery", Sao Paulo, 343, 1989.
08. MONTELLANO L. Calf augmentation. Annals o Plastic Surgery,Vol. 27, Number 5, Little BroWl and Company. Boston, 1991.
09. MONTELLANO L. Anestesia loco-regional en cirurgia estetica. Sao Paulo. Ed. Hipocratcs, 407 1993.
10. MONTELLA 0 L. Atualiza~ao em cirurgi: plastica estetica. Sao Paulo. Robe Editorial 563, 1994.
11. SPADAFORA A, SANMARCO T. Cirurgia de obesidad, flaccidez cutanea y envejecimiento Lopes Libreros Editores, Buenos Aires 1974.
12. TESTUT L, JACOB O. Anatomia topografica. Salva Editores, 1961.
13. ZE TE 0 S, MO TELLANO L. Plastia dt aumento de panturrilla. Cir Ibero- Latinnamericana, Vol. XJI, Nwn. 3, 1986.
I - Member, Brazilian Society of Plastic Surgery (SBCP) Chief, Plastic Surgely Service "Hospital Pau-Americano do Rio de Janeiro" Chief," CTQ, "Hospital Municipal Souza Aguiar do Rio de Janeiro"
ADDRESS FOR CORRESPONDENCE
Av. Oswaldo Cruz, 103/804
CEP: 22250-060 - Rio de Janeiro - RJ - Brazil
From the "Hospital Pan-Americano do Rio de Janeiro"
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket