



Articles - Year 1997 - Volume 12 -
Anatomic Study of the Communicating Venous System of the Anteromedial Region of the Leg
Estudo Anatômico do Sistema Venoso Comunicante da Região Ântero-Medial da Perna
ABSTRACT
This study demonstrates that drainage, important for the anteromedial fasciocutaneous flap of the leg, the communicating veins that unite the superficial to the deep sysrem of the oa:ompanying veins of the posterior tibial artery, continually poss between the soleus and flexor longus muscles and Ihat there are two communicating veins for each artery. The major number of communicating vessels are found in the lower third ofthe leg up to ten cm above the medial maleolus. In addition, the more proximal the communicating vessels are to the anterior wberosity of the tibia, the greater their diameter will be. No significant differences were encountered regarding the researched parameters, based on right or left side.
Keywords: Anatomy, Veins, Leg
RESUMO
Os achados do presente estudo vêm demonstrar que, em termos de drenagem venosa com importância ao retalho fasciocutâneo ântero-medial da perna, as veias comunicantes que unem o sistema superficial ao profundo das veias acompanhantes da artéria tibial posterior passam constantemente por entre os músculos sóleo e flexor longo dos dedos e que há duas veias comunicantes para cada artéria. Verificou-se que o maior número de comunicantes se encontra no terço inferior da perna, até 10 cm acima do maléolo medial, e que quanto mais proximais da tuberosidade anterior da tíbia estiverem as comunicantes, maior será seu calibre. Também não encontramos diferenças importantes quanto aos parâmetros pesquisados segundo a lateralidade.
Palavras-chave: Anatomia, Veias, Pernas
The superficial venous system ofthc lower leg and the magna and parva saphenous veins are directly connected to the deep venous system by a series ofcommunicating veins; these veins should not be confused with the perforating veins that pass through the deep fascia. The eommunicating branches are the main vessels that communicate directly with the deep veins, and are distributed along the intemlUscular fascial plane of the external surface of the muscles.
The perforators are the vessels that pass through the deep fascia and unite with the superficial veins. The communicating veins nomlally have valves that permit the blood to pass from the superficial to the deep system, and if these valves become insufficient, the blood will flow in both directions. The latter condition is associated with varicose ulcer, Linton(8).
The first reference in the literature mentioning the inclusion ofthe deep fascia in flaps was described by Bowen & Meares(3); Comlack & Lan,bcrt(4,5), classified the fasciocutaneous flaps according to the various types of vascularization; Liu & colleagues(7) studied the communicatinganeries ofthe posterior tibia and concluded that it was responsible for the blood supply ofall the anteromcdial surface of the leg, but do not mention studies regarding venous drainage of the region, which is the objective of tlllS study.
Therefore, it was decided to investigate the venous circulation ofthe anteromedial surface of the leg, which is part of the leg's anteromedial fasciocutaneous flap, keeping in mind its morphological function and surgical significance, important currently because ofits ability to restore skin losses to the lower limbs (see photos).

Fig. 1 - Catheterization of the GSV.
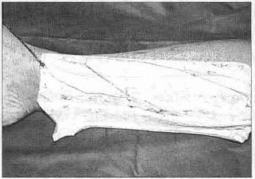
Fig. 2 - Dyed GSV and branches.
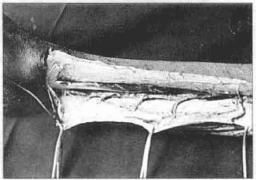
Fig. 3 - Dissected and dyed communicating veins.
Material and Methods
Fifteen fresh adult male cadavers were utilized, from the "Serviyo de Verificayao de Obitos da Univ. Federal de Sao Paulo - EPM" (Coroner's Office). Ages ranged from 32 to 75, both legs were dissected (total = 30 lower limbs).
Detemunation of the ethnic group was based on essential anthropological somatic features: skin color, hair, nose and lips. This characterization was somewhat difficult because of the high rate of miscegenation existing in Brazil, and the near absence of pure racial types, therefore including white and non-whites.
After identification, the cadaverwas placed in horizontal decubitus, with the lower limbs completely extended.
The length of the leg was detennined by the distance separating the tibial tuberosity up to the midpoint of the medial maleolus.
A transverse incisionoverthemedial maleolus through the skin and subcutaneous tissue exposed the great saphenous vein (GSV). With the help of a scalpel, the GSV was incised on the bias, and a polyethylene catheter introduced and fixed with a cotton suture. Clots were eliminated by rinsing with room temperature water. An Esmarch bandage was then placed from the distal third of the leg to the Ienee to prevent the dye's diffusion through the rest ofthe body. Blue neoprene latex (Artifix L-14) dye was slowly and continually injected (15-25 ml). An incision was made in the anteromedial region of the leg, along the body of the tibia, between its anterior tuberosity and the medial maleolus. The skin and the subcutancous tissuc wcre tumed asidc, cxposing the GSV. The medial gastricnemus and soleus muscles were rctracted and with the hclp of a 4 x magnifying lens, the communicating veins passing between the soleus ane flexor longus muscles were dissceted and measured.
The parameters studied are presented regarding the data of the superficial venous system and its communicating vessels, with the accompanying veins o the posterior tibial artery:
A) Limb length (cms);
B) Total number of communicating branches;
C) Extemal diameter of the proximal segment of thl GSV (mm);
D) Extcmal diametcr ofthc distal segment of the GSV (mm);
E) Extcmal diameter of the communicating vcssels(mm);
F) Graph showing the distribution ofthe communicatinl vcssels (cm).
Results
Our results will be presented according to the aforementioned parameters:
A) Limb length; B) Total number of communicating branehcs:
C) Extemal diamcterofthc proximal segment ofthe GSV;
D) External diameter of the distal segment of the GSV;
E) External diameter of the communicating vessels;
F) Graph showing the distribution of the communicating vessels.
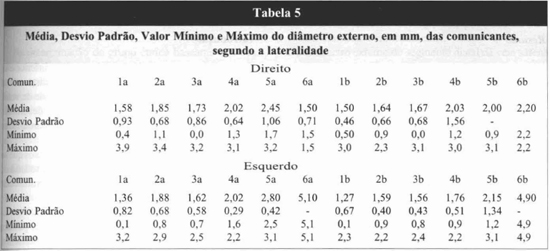
The results show that the diameter of the communicating veins on both sides is greater the closer they are to the anterior tuberosity of the tibia.
Discussion
The purpose of this anatomic study was to analyze the morphological aspects of the venous blood supply to the fasciocutaneous flap of the anteromedial region of the leg, with pedicle in the posterior tibial artery.
Contrary to Linton's studies(8), aimed at identifing the ligature of these communicating vessels, without giving due importance to the measurements of these branches, our study was directed at completing these data which were not stressed by the author.
After consulting a series of reports, we did n01 find sufficient data that could be compared to our results, from an anatomic point of vicw. and that could be applied clinically. Analyzing thc various tables wc note in tables 1,2,3 and 4 that therc was no significant differencc based on latcrality, whcn the Wilcoxon test was applied.
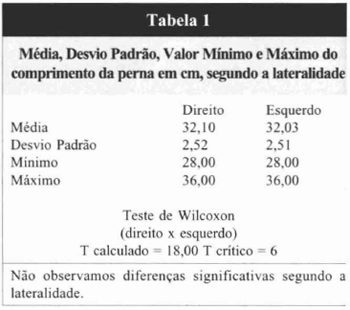
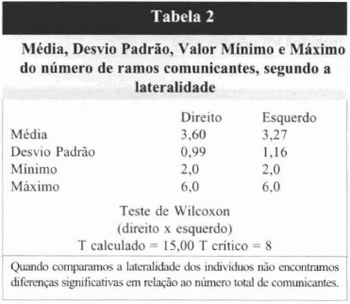
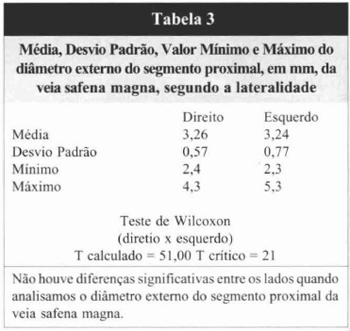
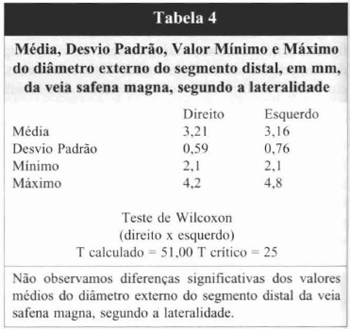
Table 2 shows that the number of communicating branches displayed a mean of 3.60 and 3.27, respectively for the right and left sides. Nevertheless, we point out that d,e nunlbcr of eommwucating veins varied from two to six for both sides, but the analysis of tables 3 and 4 evaluating the mean values of extemaldiameter of the proximal and distal segments respectively of the GSV, did not demonstrate significant differences.
The analysis of table 5, shows that the external diameter of the communicating bnUlehes is proportional to their proximity to the anterior tibial tuberosity. Anention is called to the strange aspect that is the confluence ofthe two commwljcating veins in the respective accompanying veins of the posterior tibial anery, followed by a single anery, i.e., therc are two veins for each artery.
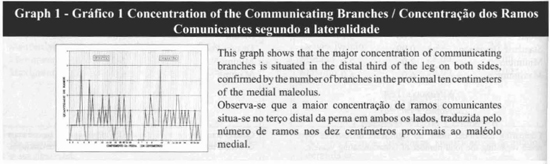
The graph illustrating the conccntration of the conU1lwucating branches shows dlat the majority of these vessels is distributed in the distal third of the limb, i.e., in dIe ten centimeters proximal to dIe medial malcolus. From a clinical point of view,this data permis the anteromedial fasciocutaneous flap ofdIe leg to be sectioned proximally, d,US maintaining its arteria-venous blood supply via d,e distal pedicle(1,2,6).
Conclusion
1. The communicating branches always pass between the soleus and flexor longus muscles.
2. The major number of communicating branches is situated in the lower third of the leg.
3. The diameter ofthe proximal eotrullunieatingbranches is greater than that of the distal ones.
4. There are two communicating veins for each artery.
5. There is no statistically significant difference regarding laterality.
References
01. AMARANTE J., COSTA H., REIS J., and SOARES R.A new distally based fasciocutaneous flap of the leg. Br J. Plast. Surg., 39: 338, 1986.
02. BARCLAY TL, CARDOSO E., SHARPE DT. and CROCKETT OJ. Repair of lower leg injuries with fasciocutaneous flaps. Br.J. Plast.Surg. 35: 127, 1982.
03. BOWE J. and MEARES A. Delayed local leg flaps.Br. J. Plast. Surg. 27: 167, 1974.
04. CORMACK GC and LAMBERTY BGH. Fasciocutaneous vessels. Their distribution on the trunk and limbs, and their clinical application in tissue transfer. Ann. Clin., 6: 121, 1984.
05 CORMACK GC and LAMBERTY BGH. The arterial anatomy of skin flaps. Edinbnrgh, Churchill Livingstone, 1986.
06. EL-SAADI MM. and KHASHABA. Tree anteromedial fasciocutaneous leg island for covering defects of the lower two thirds of the leg. Br. J. Plast. Surg.43: 536, 1990.
07. LIUK.,LIZ.,LINY.andCAOY.The reverse-flow posterior tibial artery island flap: anatomic study and 72 clinical cases. Plast. Reconstr. Surg., 3: 312,1990.
08. LINTON RR. The communicating veins of the lower leg and the operative technic for their ligation.Ann. Surg., 107: 582,1938.
I - Member of "Sociedade Brasileira de Cirurgia Pltistica" (SBCP) and A.M.B. Fellow ofIII/emational College Surgeons (FlCS), Member of "Sociedade Brasileira Craniomaxilofascial"
II - Tilular Member and Especialist of "Sociedade Brasileira de Cirurgia Plilslica (SBCP) ", Titular Member and especialist of "Sociedade Brasileira de Cintrgia da Miio", Master in "Medicina na Area de Cintrgia da FMUSP", Doctor in "Area de Ciencias Biol6gicas pela UNIFESP-EPM .., Prof of "Cirurgia da Mão do Hospital Darci Vargas"
ADDRESS FOR CORRESPONDENCE
Paulo Nuno Fernandes Farinha
Rua ltapeva, 490 - Cj. 114
Bela Vista - Sao Paulo CEP 01332-000
Tel.: (011) 289-4733
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket