



Articles - Year 1997 - Volume 12 -
Spiegelian Hernia Secondary to Abdominoplasty
Hérnia de Spiegel após Abdominoplastia
ABSTRACT
After analyzing 690 hernioplasties performed during the period between 1960 and 1994, the authors found three cases of Spiegel's hernia, all diagnosed in patients that had undergone prior abdominoplasty. They suggest that plication of Spiegel's "linea semilunaris" associated with classical abdominoplasry may comribllle to the prevention ofSpiegeliall Hernia, since this plication reinforces a weak point in the anterolateral abdominal wall.
Keywords: Hernia, Spiegel's Linea Semilunaris Plication, Abdominoplasty
RESUMO
Os autores, após análise de 690 hernioplastias no período entre 1960 e 1994, encontraram três casos de Hérnia de Spiegel, todos diagnosticados em pacientes que já haviam se submetido a abdominoplastia prévia. Com isso, sugerem que a plicatura da linha semilunar de Spiegel associada à abdominoplastia clássica possa contribuir como método preventivo no aparecimento da hérnia, uma vez que a plicatura reforça um ponto débil da parede ântero-lateral do abdome.
Palavras-chave: Hérnia, Plicatura da Linha Semilunar de Spiegel, Abdominoplastia
Spiegel's hernia can be found under the name Spiegel, Spigel, Spigelius, Hernia of the semilunar line or Spontaneous Ventrolateral Hernia of the Abdomen.
Spiegel's semilunar line was named by Adrian Van Der Spiegel between 1578-1625, at the time professor of anatomy and surgery at the University of Padua. It is defined as the transition line between the internal oblique and the transverse muscles of the abdomen, extending from the eight or thc ninth costal cattilage to the pubic tubercule fonning a convex lateral curve which cxplains thc name semilunar. The aponeurosis between the semilunar line and the lateral margin of the abdominis rectus muscle is called Spiegel's band (Fig. 1).
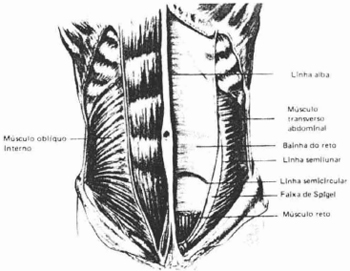
Fig. 1 - Anatomy of the abdominal wall, illustrating Spiegel's line.
This hernia is characterized by the protrusion of a peritoneal sac, an organ or preperitoneal fat from its nOrlllal position t1lrough a congenital or acquired orifice in Spiegel's band. Originally describe by La Chaussc, in 1746 according to Olson & colleagues(6); the hernia is usually located between the muscle layers of the abdominal wall and, therefore, is called interparietal, intersticial, intramuscular or intramural. Sir Astley Cooper (1804), introduced the theory that the possible increase in diameter of neurovascular orifices in Spiegel's band might pennit hemiation. This hypothesis, however, was disproved after a study publishcd by Zimmernlan & colleagues(11), who after 500 anatomic dissections, confimled thc rarity ofblood vcssels passing through the defect.
The most plausible theory concerning the origin of this hernia is bascd on thc fact that the anterolateral wall of the abdomen consists of two muscles on cach sidc of the anterior portion (abdominis rectus and pyramidal) and three muscles on the anterolateral portion (extemal oblique, internal oblique and transverse ofthe abdomen).
Each of these three muscles is wrapped by its fascia that unite medial1y to fonn the sheath of the abdominis rectus.
Above the arched or semicircular line of Douglas, the aponeurosis ofthe intemal oblique divides into two laminae, one together with aponeurosis of the extemal oblique passes over the abdomillis rectus while il,e other lamina, together with the aponeurosis ofthe extemal oblique passes over the abdominis rectus while the other lamina, together with the aponeurosis ofthe transversus abdominis and the transverse fascia shape the posterior portion of the sheath of the abdominis rectus. Below the semicircular line the three aponeurosis unite, only passing anteriorly to the abdominis rectus which remains separated from the peritonewn onlyby thetransversc fascia and looscconnecrive tissue. They b~come weak or even absent at the posterior lamina of the reetus sheath and the majority ofSpiegel ian Hemias occurs in this weak spot(7).
Material and Methods
The objective of this study, is to link Spiegelian Hemia to post-operative abdominoplasty patients and to recommend plication of Spiegel's line to prevent this.
Surgical cases of abdominoplasty patients on the service between 1960 to 1994, were examined and 16 cases were reeorded as fol1ows.
The three cases of Spiegel ian Hemia occurred in females and add up to a percentage of 18,75%.
Surgeries Accomplished after Abdominoplasties
A total of 690 hernioplasties performed during the above time period were examined. A description and photographs of a casc of this hemia is presented.
Fifteen months prior to her complaints, M.G.S., a white fcmale weighing 76 kg, underwent abdominoplasty.
Two months ago she began feeling lumbar pain in the iliac fossa on the left side.
Physical examination demonstrated a globulat abdomen, with signs ofabdominoplasty and with diffuse protrusion in the left flank and iliac fossa, lateral to the abdominis rectus muscle. The laboratory tcsts, ultrasonography and computerized tomography were inconclusive. The general and plastic surgeons suspected thc clinical diagnosis ofSpiegelian Hemia. The diagnosis was confirmed at surgery and the hernia and the dennoadipose dcformity by it were correeted (Figs. 2-9).

Fig. 2 - Profile of patient with Spiegel's hernia.

Fig. 3 - Frolll view of Spiegel's hernia.
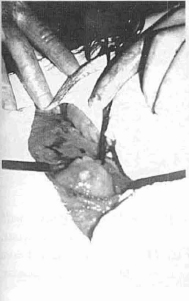
Fig. 4 - Spiegel hernia dissecred.

Fig. 5 - Excess peritoneum, resected.

Fig. 6 - Hernial contents isolated. Greater omentum.

Fig. 7 - Exposure for hernioplasry.

Fig. 8 - Hernioplasty with imbrication.
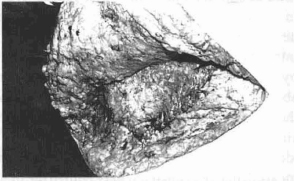
Fig. 9 - Hernioplasry wirth contralateral strengthening of Spiegel's line.
Results
Surgeries Accomplished after Abdominoplasties The disposable data, of the 690 hernioplasty cases, demonstrated only threc Spicgel hcmioplasties, which coincides with the three cases accomplished after abdominoplasty. This revealed that a total of 100% of cases of Spiegel hemioplasty on the service were perfonned after prior abdominoplasty; leading us to correlate this result.
Prospective studies are planned on patients submitted to abdominoplasty with plication of the Spiegcl semilunar line (Figs. 10, 11), together with midline plication, with the scope ofverifying whether or not this hemia appears after abdominoplasty.
Fig. 10 - Abdominoplasry with plication of the midline and of Spiegel's line.

Fig. 11 - Abdominoplasry with completed plications.
Discussion
Although there are few articles on the subject, Spiegel's hemia is not so rare and its diagnosis is not very often made. Reponed cases have almost always involved adults (however, they have already been described in children and the elderly), predominating between the fifth and sixth decades. It may present uni or bilaterally and the sex reatio is 1:1(1,4,6,10). All the patients in our series are females, perhaps because abdominoplasty is more common in this sex. 0 preference is apparent as to the side of the abdominal wall. However, its more obvious location is below the umbilical scar and more rarely on the cephalad portion of the abdomen(9). The explanation is that in the erect position the intra-abdominal pressure is greater below the umbilical scar due to the force of gravity exened by the organs. Responsible for the etiology ofSpiegel 's hemia, in addition to congenital anatomic defects arc factors which increase the intraabdominal pressure. Among these are: obesity, repeated pregnancies, ascitis, chronic cough, severe muscular effon, considerable weight loss due to dieting or disease, constipation, flatulent foods and those difficult to digest, intra-abdominal tumor and other causes. We would like to include abdominoplasty to this list as a cause of this hemia. based on our series and because of increased intra-abdominal pressure promoted by this surgery, both by the denno-adipose resection and the conventional abdominal midline plication. The case prescnted, displays the typical symptoms of intennittent pain on effort, similar to neuralgia, located in Spiegel's line, and identified by the patient above it. If the patient noted local edema, previously, it may help in the diagnosis that is sometimes difficult because of the abseence of pain.
Symptoms may vary somewhat, depending on the contents of the hemial sac which may be omental and intestinal for tbe most pan. Our patient presented a palpable mass in the region of Spiegel's line, which is uncommon, forthe examination may be difficult because the hernia is located interparietally in many cases.
Valsalva maneuvers may facilitate palpation of the hernial orifice which ranges from 0.5 to 2.0 cm, with description of orifices of lip to 6 or 8 em in diameter(9).
Diagnosis may be simplified by contrast X-ray, ultrasonographic mapping and computerized tomography. However, as in the ease presented, surgical exploration confimls the diagnosis.
Conclusion
Because of the largc increase in intra-abdominal prcssure consequent to classical abdominoplasty, a hernia may originate in the Spiegel semilunar line, which usually requires surgery. Although the surgery itself is simple, it subjects thc patient to an unnecessary surgcry, with its added risks and expense.
In agreement with what has been presented, we recommend plication of Spicgel's semilunar line to prevent the appearance of Spiegel ian Hemia, sinee the weak spot in the anterolateral abdominal wall is strengthened.
References
01. BAILEY D. Spiegelian Hernia (Report oftive cases and review ofthe literature). Br J Surg, 44: 503, 1957.
02. CONDON RE. Surgical anatomy ofthe transversus abdominis and transversalis fascia. Ann Surg, 173: 1-5, 1971.
O3. HARLESS MS, HIRSCH JE. Spiegelian or spontaneous lateral ventral hernia. Am J Surg, 100: 515-521,1960.
04. HOULlHAN TJ. A review of Spiegelian Hernias. Am J Surg, 131: 734-735, 1976.
05. KOONTZ AR. Hernia in the linea sernilunaris. Ann Surg, 135: 875-878,1952.
06.0LSO RO, DAVlS We. Spiegelian Hernia: Rare or obscure? Am J Surg, 116: 842-846,1968.
07. PEIXOTO HS, SILVA JAT. Hernia de Spiegel. J Bras Med,44: 121-122, 1983.
08. READ RC. Observations on the etiology of Spiegelian Hernia. Ann Surg, 152: 10041009, 1960.
09. SPANGEN L. Hernia de Spiegel. Clinicas Cirurgicas da America do Norte, 2: 369- 385, 1984.
10. SILVA AL, GUERRA AJ. Hernia Ventrolateral (Hernia de Spiegel). Hernias - Ed. Roca - Sao Paulo, 560-566, 1992.
11. ZIMMERMAN LM, ANSON BJ, MORGAN EH et al. Ventral Hernia due to normal banding of the abdominal muscles.Surg Gynecol Obstet, 78: 535-540, 1944.
I - First year residelll: "Centro de Formarção e Treinamento em Cirurgia Plastica, Hospital Mater Dei" (HMD) and "Clinica de Cirurgia Plastica Sebastião Nelson Ltda." (CCPSN)
II - General Surgeon; Member Brazilian College of Surgeons; former professor, Department of Surgery, Federal University ofMinas Gerais Medical Sclrool (UFMG); General Surgeon, HMD and "Hospital Socor"
III - President and Member, Brazilian Society of Plastic and Reconstructive Surgery (Minas Gerais Chaptel); Instructor "Centro de Formarção e Treinamento em Cirurgia Plastica ", HMD; President, Organizing Commission, 31st Brazilian Congress of Plastic Surgery
ADDRESSES FOR CORRESPONDENCE
1 - Rua Gonyalves Dias, 2700
30140-093 - Santo Agostinho
Belo Horizonte - MG - Brazil
2 - Av. do Contomo, 5051;
B. Serra 30110-100
Belo Horizonte - MG - Brazil
Tel. (031) 223-8844 - Fax (031) 225-6595
From the Hospital Mater Dei1 and General Surgery Team of Dr. Guido Monteiro da Cunha Magalhães and the CCPSN Ltda2.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket